Excision of Dorsal and Volar Wrist Ganglions: A Comprehensive Surgical Guide
Key Takeaway
Wrist ganglion excision requires meticulous dissection to prevent recurrence and neurovascular injury. For dorsal ganglions, the stalk is typically traced to the scapholunate interval. Volar ganglions require careful mobilization of the radial artery and protection of the palmar cutaneous branch of the median nerve. Complete excision of the cyst complex, including its capsular origin, is the gold standard for minimizing recurrence rates in both approaches.
INTRODUCTION AND PATHOPHYSIOLOGY
Ganglion cysts are the most common soft-tissue tumors of the hand and wrist, accounting for approximately 50% to 70% of all such masses. These benign, mucin-filled cysts typically arise from adjacent joint capsules or tendon sheaths. The exact etiology remains a subject of academic debate, though the prevailing theory suggests that mucoid degeneration of connective tissue, combined with a one-way "check-valve" mechanism at the capsular level, leads to the accumulation of highly viscous synovial fluid.
Dorsal wrist ganglions predominantly originate from the dorsal scapholunate interosseous ligament (SLIL) interval. Conversely, volar wrist ganglions typically arise from the radiocarpal joint (specifically the radioscaphoid interval) or the scaphotrapezial joint. While many ganglions are asymptomatic and resolve spontaneously, surgical excision is indicated for patients experiencing persistent pain, mechanical symptoms, weakness, or significant cosmetic deformity that has failed conservative management (such as aspiration and corticosteroid injection).
This comprehensive guide details the operative techniques for both dorsal and volar wrist ganglion excisions, emphasizing precise anatomical dissection, neurovascular protection, and the critical step of capsular origin resection to minimize recurrence.
ANATOMY AND BIOMECHANICS
A profound understanding of wrist anatomy is paramount for safe and effective ganglion excision. The surgical approach must navigate complex neurovascular and tendinous structures.
Dorsal Wrist Anatomy
The dorsal wrist is organized into six extensor compartments defined by the extensor retinaculum. A dorsal ganglion typically presents between the third and fourth extensor compartments. The key structures encountered include:
* Extensor Pollicis Longus (EPL): Resides in the third compartment, angling around Lister's tubercle.
* Extensor Digitorum Communis (EDC): Resides in the fourth compartment.
* Extensor Carpi Radialis Longus (ECRL) and Brevis (ECRB): Reside in the second compartment, inserting at the base of the second and third metacarpals, respectively.
* Extensor Retinaculum: The fibrous band that prevents bowstringing of the extensor tendons.
* Scapholunate Interosseous Ligament (SLIL): The dorsal portion of this ligament is the thickest and most biomechanically critical for carpal stability. The stalk of a dorsal ganglion almost universally originates from the capsule overlying this ligament.
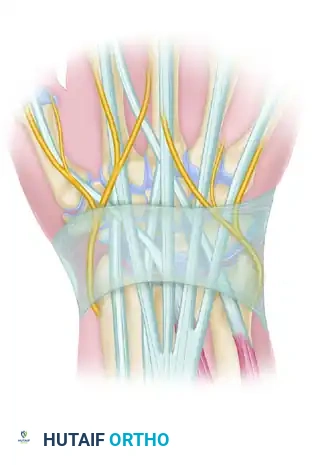
Volar Wrist Anatomy
Volar ganglions are intimately associated with the radial artery and the flexor tendons. Key structures include:
* Flexor Carpi Radialis (FCR): The ganglion is usually situated just radial to this tendon.
* Radial Artery: Often courses directly over, or even through, the lobulations of a volar ganglion cyst.
* Palmar Cutaneous Branch of the Median Nerve (PCBMN): Arises approximately 5 cm proximal to the wrist crease and travels distally between the FCR and palmaris longus. Injury to this nerve results in debilitating neuromas.
Surgical Pearl: The fundamental biomechanical principle of ganglion excision is the complete removal of the "check-valve" stalk and a small window of the surrounding joint capsule. Failure to excise this capsular origin is the primary cause of postoperative recurrence, which can be as high as 15% to 20% in inadequately resected cases.
PREOPERATIVE PREPARATION
- Clinical Evaluation: Confirm the diagnosis via transillumination and physical examination. Assess for occult carpal instability.
- Imaging: Standard posteroanterior (PA) and lateral radiographs of the wrist are mandatory to rule out underlying osseous pathology (e.g., carpal boss, osteoarthritis, or scapholunate advanced collapse). Magnetic Resonance Imaging (MRI) or ultrasound may be utilized for atypical or occult cysts.
- Vascular Assessment: For volar ganglions, perform an Allen test preoperatively to assess the integrity of the radial and ulnar arterial contributions to the hand. This is critical, as the radial artery may require extensive dissection or, in rare catastrophic cases, ligation.
SURGICAL TECHNIQUE: EXCISION OF A DORSAL WRIST GANGLION
Positioning and Setup
The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (Bier block or brachial plexus block) or general anesthesia is administered. The limb is exsanguinated, and the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above systolic blood pressure). Loupe magnification (2.5x to 3.5x) is highly recommended.
Superficial Dissection and Nerve Protection
Make a transverse or longitudinal incision centered over the apex of the ganglion mass. A transverse incision often provides a superior cosmetic result by following Langer's lines, though a longitudinal incision allows for easier proximal-distal extension if required.
Carefully dissect through the subcutaneous tissues. Identify and meticulously protect the sensory branches of the superficial radial nerve radially and the dorsal branch of the ulnar nerve ulnarly. Retract these sensory branches using blunt Ragnell or Sen retractors.
Exposure of the Extensor Retinaculum
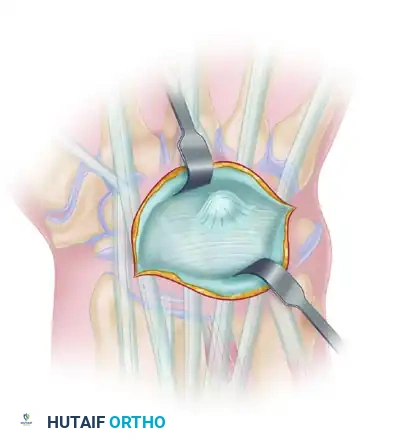
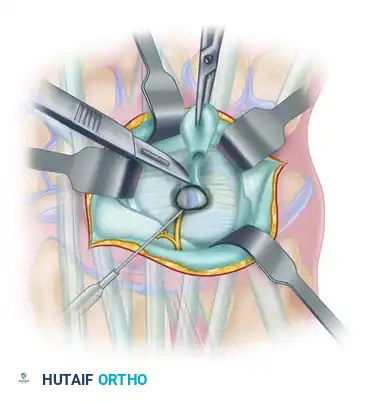
Deepen the dissection to expose the extensor retinaculum. The ganglion cyst will typically be visible as a bluish, translucent bulge protruding through or stretching the retinacular fibers, usually between the EPL (third compartment) and the EDC (fourth compartment).
Retinacular Incision and Cyst Identification
Incise the extensor retinaculum longitudinally over the cyst. Take care not to inadvertently incise the underlying cyst wall, as premature rupture deflates the mass and makes tracing the stalk significantly more difficult.
Once the retinaculum is opened, deploy self-retaining retractors or have an assistant maintain exposure. Identify the Extensor Carpi Radialis Longus, Extensor Carpi Radialis Brevis, and Extensor Digitorum Communis tendons, mobilizing them radially and ulnarly as needed to fully expose the cyst complex.
Dissection of the Cyst and Stalk
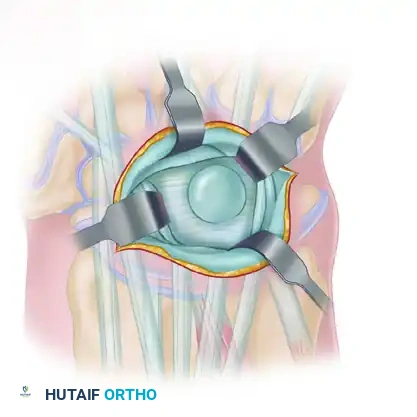
Using a combination of sharp dissection with a #15 scalpel blade and blunt dissection with tenotomy scissors, begin freeing the cyst from the surrounding paratenon and soft tissues.
Work circumferentially around the cyst, progressing from superficial to deep. As the dissection deepens, the cyst will narrow into a distinct pedicle or "stalk" that dives toward the carpal bones.
Surgical Warning: Do not pull forcefully on the cyst dome. Excessive traction will tear the delicate cyst wall, spilling mucin into the surgical field and obscuring the anatomical planes necessary to trace the stalk to its origin.
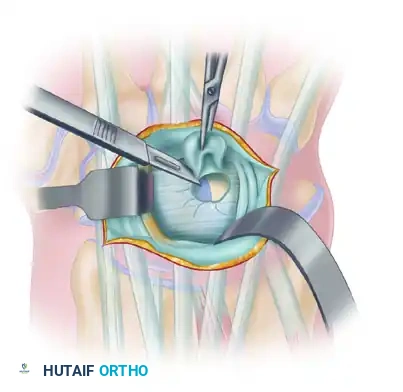
Excision of the Capsular Origin
Trace the stalk down to its origin at the dorsal wrist capsule, which is almost invariably located at the scapholunate interval.
To ensure complete eradication of the check-valve mechanism, excise the stalk along with a 5 mm to 1 cm margin of the surrounding dorsal capsule.
Pitfall: While excising the capsular window, you must visualize the underlying scapholunate interosseous ligament (SLIL). Do not resect the SLIL. The dorsal band of the SLIL is the primary stabilizer of the scapholunate joint; its iatrogenic transection will result in catastrophic scapholunate dissociation (DISI deformity).
Once the cyst and capsular window are removed en bloc, inspect the joint space. Cauterize the capsular margins lightly with bipolar electrocautery to destroy any remaining micro-cysts. Do not attempt to close the capsular defect; leaving it open does not lead to instability and may reduce recurrence.
SURGICAL TECHNIQUE: EXCISION OF A VOLAR WRIST GANGLION
Volar ganglion excision is inherently more hazardous due to the proximity of the radial artery and median nerve branches.
Incision and Superficial Dissection
Under tourniquet control, make a longitudinal or curvilinear incision centered over the ganglion. The mass is usually situated just radial to the flexor carpi radialis (FCR) tendon.
Meticulously dissect through the subcutaneous fat. Avoid injury to the palmar cutaneous branch of the median nerve (PCBMN). This nerve lies ulnar to the FCR tendon but can have aberrant branches. Retract the FCR tendon ulnarly.
Radial Artery Mobilization
Carefully dissect the radial artery under loupe magnification. The radial artery is frequently found to course directly over, or even weave through, several lobes of the ganglion cyst.
Surgical Pearl: Use bipolar electrocautery and fine tenotomy scissors to dissect the adventitia of the radial artery away from the cyst wall. Mobilize the artery over a sufficient length (often 3 to 4 cm) to allow it to be gently retracted radialward using a vessel loop. Never use aggressive traction on the artery, as this can induce vasospasm or intimal tearing.
Dissection of the Volar Stalk
With the radial artery retracted radialward and the FCR retracted ulnarward, dissect the ganglion cyst using blunt and sharp dissection in a proximal-to-distal direction.
Carry the dissection down along the stalk of the ganglion to its origin. Volar ganglions may arise from several distinct regions, including:
* Radioscaphoid joint
* Scapholunate interval (volar aspect)
* Scaphotrapezial joint
* Trapeziometacarpal joint
On rare occasions, a volar-appearing mass may actually be a projection of a dorsal ganglion cyst that has tracked circumferentially under the first extensor compartment tendons.
Capsular Excision and Closure
Excise the origin of the stalk along with a small portion of the surrounding volar capsule. As with the dorsal approach, do not over-resect the volar extrinsic carpal ligaments (e.g., radioscaphocapitate ligament), as this can lead to carpal instability.
Cauterize the capsular margins and thoroughly irrigate the wound with sterile saline.
HEMOSTASIS AND CLOSURE (BOTH APPROACHES)
- Tourniquet Deflation: Prior to closure, deflate the tourniquet. This step is absolutely critical, especially in volar ganglion excisions, to inspect the integrity of the radial artery and ensure adequate perfusion to the hand.
- Hemostasis: Use hemostats and bipolar electrocautery to control any further bleeding. Meticulous hemostasis prevents postoperative hematoma formation, which can increase scarring and stiffness.
- Wound Closure: The extensor retinaculum (in dorsal approaches) may be loosely reapproximated, but it is often left open or repaired in a step-cut fashion to prevent postoperative bowstringing while avoiding tendon constriction. Close the subcutaneous tissue with interrupted absorbable sutures (e.g., 4-0 Vicryl). Close the skin with non-absorbable monofilament sutures (e.g., 4-0 or 5-0 Nylon) or a subcuticular closure based on surgeon preference.
- Dressing: Apply a sterile, non-adherent dressing followed by a bulky soft dressing. A volar resting splint is applied with the wrist in slight extension (for dorsal excisions) or neutral (for volar excisions) to protect the surgical site and minimize immediate postoperative edema.
POSTOPERATIVE PROTOCOL AND REHABILITATION
- Days 0-7: The patient is instructed to keep the limb elevated above heart level to minimize swelling. Immediate active range of motion (ROM) of the fingers, thumb, elbow, and shoulder is highly encouraged to prevent stiffness and promote tendon gliding.
- Days 7-14: The patient returns to the clinic for wound inspection and suture removal. The rigid splint is typically discontinued at this stage.
- Weeks 2-6: Patients are transitioned to a removable wrist orthosis, to be worn during heavy activities. Gentle, progressive active and active-assisted wrist ROM exercises are initiated. Formal occupational therapy may be prescribed if the patient exhibits significant stiffness, scar tethering, or kinesiophobia.
- Weeks 6+: Unrestricted return to normal activities and heavy lifting is generally permitted once full, painless ROM and grip strength are restored.
COMPLICATIONS AND PITFALLS
While ganglion excision is a routine outpatient procedure, complications can be significant if anatomical principles are violated.
- Recurrence: The most common complication. Recurrence rates are minimized (<5%) by ensuring complete excision of the capsular stalk and a window of the adjacent joint capsule.
- Nerve Injury: Neuromas of the superficial radial nerve, dorsal ulnar sensory nerve, or palmar cutaneous branch of the median nerve are highly debilitating. Meticulous superficial dissection and gentle retraction are mandatory.
- Vascular Injury: Injury to the radial artery during volar ganglion excision can lead to pseudoaneurysm, thrombosis, or hand ischemia. Preoperative Allen testing and intraoperative loupe magnification are essential safeguards.
- Carpal Instability: Iatrogenic transection of the dorsal scapholunate interosseous ligament (SLIL) during dorsal capsular resection will cause a DISI deformity. The surgeon must clearly visualize the ligamentous fibers and resect only the overlying capsule.
- Postoperative Stiffness: Prolonged immobilization is detrimental. Splinting should rarely exceed 7 to 10 days, and early digital motion must be enforced from postoperative day one.
You Might Also Like


