Masterclass in Wrist Arthrodesis: Haddad-Riordan and AO/ASIF Techniques

Key Takeaway
Total wrist arthrodesis is a highly effective salvage procedure designed to provide a stable, pain-free wrist while maximizing grip strength. This comprehensive guide details the classic Haddad and Riordan slot-graft technique alongside modern AO/ASIF dynamic compression plating. Key surgical steps include meticulous joint preparation, precise 15-degree dorsiflexion positioning, and careful evaluation of the distal radioulnar joint to prevent postoperative ulnocarpal complications.
INTRODUCTION TO WRIST ARTHRODESIS
Total wrist arthrodesis remains the gold standard salvage procedure for end-stage radiocarpal and intercarpal arthropathy. When joint-preserving procedures, proximal row carpectomy, or partial fusions are no longer viable, a complete arthrodesis provides a stable, pain-free platform that reliably restores powerful grip strength.
Historically, the procedure relied heavily on extensive bone grafting and prolonged cast immobilization, as popularized by the classic Haddad and Riordan technique. In contemporary orthopedic practice, the advent of AO/ASIF dynamic compression plating has revolutionized the procedure, offering rigid internal fixation, higher union rates, and the elimination of prolonged postoperative casting.
This comprehensive surgical guide details both the foundational Haddad and Riordan slot-graft technique and the modern AO/ASIF compression plate technique, providing orthopedic residents, fellows, and practicing consultants with an evidence-based roadmap for successful surgical execution.
INDICATIONS AND CONTRAINDICATIONS
Primary Indications
- Post-Traumatic Osteoarthritis: End-stage arthritis secondary to scapholunate advanced collapse (SLAC), scaphoid nonunion advanced collapse (SNAC), or highly comminuted intra-articular distal radius fractures.
- Rheumatoid Arthritis: Severe inflammatory arthropathy with carpal subluxation, ulnar translation, and loss of functional hand mechanics.
- Salvage Procedures: Failed partial wrist fusions (e.g., four-corner fusion), failed total wrist arthroplasty, or failed proximal row carpectomy.
- Neuromuscular Disorders: Spastic hemiplegia or brachial plexus palsies requiring a stable post for tendon transfers.
- Tumor Resection: Reconstruction following the excision of primary bone tumors of the distal radius or carpus.
Contraindications
- Active local or systemic infection.
- Open physes in pediatric patients (relative contraindication; requires physeal-sparing techniques).
- Severe soft tissue compromise or inadequate dorsal skin coverage.
- A functional, painless wrist with preserved motion (where partial fusion may be indicated).
BIOMECHANICS AND PREOPERATIVE PLANNING
Optimal Positioning for Fusion
The functional success of a wrist arthrodesis is entirely dependent on the angle of fusion. The wrist must be positioned to optimize the length-tension relationship of the extrinsic finger flexors, thereby maximizing grip strength.
Clinical Pearl: The Angle of Arthrodesis
The universally accepted optimal position for wrist arthrodesis is 10 to 15 degrees of dorsiflexion and slight ulnar deviation (0 to 5 degrees). Excessive dorsiflexion (beyond 20 degrees) can lead to extensor tendon irritation and fatigue, while volar flexion severely compromises grip strength and hand function.
Evaluation of the Distal Radioulnar Joint (DRUJ)
In their extensive review of complications following AO/ASIF wrist arthrodesis, Zachary and Stern emphasized a critical preoperative mandate: the rigorous clinical and radiographic evaluation of the DRUJ.
Fusing the radiocarpal joint alters the biomechanics of forearm rotation. If pre-existing DRUJ arthritis, instability, or ulnocarpal impaction is present and ignored, the patient will experience persistent postoperative ulnar-sided wrist pain.
* Concomitant Procedures: If DRUJ pathology is identified, surgeons must be prepared to perform a concurrent Darrach procedure (distal ulna resection), a Suave-Kapandji procedure (DRUJ arthrodesis with distal ulna pseudarthrosis), or ulnar shortening osteotomy.
SURGICAL ANATOMY AND EXPOSURES
A thorough understanding of the dorsal compartments of the wrist is mandatory to avoid iatrogenic injury during exposure.
* First Dorsal Compartment: Abductor pollicis longus (APL) and extensor pollicis brevis (EPB).
* Second Dorsal Compartment: Extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB).
* Third Dorsal Compartment: Extensor pollicis longus (EPL), which wraps around Lister's tubercle.
* Fourth Dorsal Compartment: Extensor digitorum communis (EDC) and extensor indicis proprius (EIP).
The surgical interval for wrist arthrodesis typically exploits the space between the first and second dorsal compartments or the third and fourth compartments, depending on the specific technique and hardware utilized.
SURGICAL TECHNIQUE 1: THE HADDAD AND RIORDAN APPROACH
The Haddad and Riordan technique utilizes an autologous iliac crest bone graft inlaid into a precisely cut slot spanning the distal radius, carpus, and metacarpals. While largely superseded by plate osteosynthesis, it remains a vital technique in cases of severe bone loss, infection salvage where hardware is contraindicated, or when rigid plating is not feasible.
Step 1: Incision and Superficial Dissection
- Begin with a J-shaped skin incision. Start 2.5 to 3.8 cm proximal to the radial styloid on the midlateral aspect of the forearm.
- Extend the incision distally across the radial styloid.
- Curve the incision dorsally to terminate at the base of the second metacarpal.
- Nerve Protection: Meticulously mobilize and retract the superficial branch of the radial nerve (SBRN). The SBRN is highly susceptible to traction injury and subsequent painful neuroma formation.
Step 2: Deep Exposure and Retraction
- Identify the surgical interval between the first dorsal compartment (APL, EPB) and the second dorsal compartment (ECRL, ECRB).
- Incise the dorsal carpal ligament within this interval. Crucially, leave the ligament attached to the volar aspect of the radius to serve as a soft-tissue interposition layer during closure.
- Perform a subperiosteal mobilization. Retract the APL and EPB radially, and retract the wrist and finger extensors ulnarly.
Step 3: Tendon and Capsule Management
- Identify the Extensor Carpi Radialis Longus (ECRL) tendon. Divide it just proximal to its insertion at the base of the second metacarpal.
- Surgical Tip: Leave a sufficient distal stump of the ECRL so that it can be securely sutured during the closure phase.
- Perform a thorough capsulectomy. Remove the dorsal capsule from the radiocarpal joint, the intercarpal joints, and the second carpometacarpal (CMC) joint to expose the articular surfaces.
Step 4: Vascular Control and Joint Preparation
- Locate the dorsal branch of the radial artery. Ligate and divide its branches contributing to the dorsal carpal arch to prevent postoperative hematoma.
- Using sharp curettes, rongeurs, and a high-speed burr, systematically denude the radiocarpal and intercarpal joints of all articular cartilage down to bleeding subchondral bone. This step is paramount for achieving a robust biological fusion mass.
Step 5: Graft Harvesting and Slot Preparation
- Prepare a separate surgical site at the ipsilateral pelvis. Using an oscillating saw and sharp osteotomes, harvest a corticocancellous graft from the inner table of the iliac crest. The graft should measure approximately 3.8 cm long by 2.5 cm wide.
- Return to the wrist. Position the wrist in the optimal 15 degrees of dorsiflexion.
- Using an oscillating saw, cut a precise rectangular slot spanning the distal end of the radius, across the denuded carpal bones, and into the bases of the second and third metacarpals.
🚨 SURGICAL WARNING: DRUJ Protection
When cutting the slot into the distal radius, do not cut through the medial cortex of the radius. Penetrating the medial cortex will inadvertently enter the Distal Radioulnar Joint (DRUJ), leading to severe postoperative rotational pain, instability, and radioulnar synostosis.
FIGURE 69-80 (A): Radial view demonstrating the precise slot cut into the distal radius, carpal bones, and the bases of the second and third metacarpals. Note the preservation of the medial radial cortex.
Step 6: Graft Placement and Fixation
- Impact the harvested iliac crest graft into the prepared bed. The cortical surface of the graft should sit flush with the dorsal cortex of the radius and metacarpals, while the cancellous surface interfaces with the deep carpal bed.

FIGURE 69-80 (B): Dorsal view illustrating the shape of the inner iliac crest graft and its final seated position (broken line) within the prepared slot.
- Supplemental Fixation: If the wrist remains rotationally or sagittally unstable after graft impaction, insert a smooth Kirschner wire (K-wire) obliquely or longitudinally. The wire should engage the base of the second metacarpal and drive proximally into the distal radius. Cut the wire beneath the skin in the palm (to be removed 6 to 8 weeks postoperatively).
Step 7: Closure
- Repair the dorsal carpal ligament deep to the APL and EPB to prevent tendon bowstringing and provide a smooth gliding surface.
- Suture the divided ECRL tendon back to its distal stump.
- Close the subcutaneous tissues and skin in layers. Apply a sterile dressing and a rigid sugar-tong splint to control forearm rotation and wrist flexion/extension.
SURGICAL TECHNIQUE 2: AO/ASIF DYNAMIC COMPRESSION PLATING
The modern standard of care for wrist arthrodesis utilizes rigid internal fixation via dynamic compression plating. This technique, championed by the AO Foundation, provides superior biomechanical stability, significantly higher union rates, and eliminates the morbidity associated with prolonged cast immobilization.
Advantages of the AO/ASIF Technique
- Immediate Stability: Allows for early mobilization of the digits, reducing postoperative stiffness.
- High Union Rates: Dynamic compression across the radiocarpal joint promotes primary bone healing.
- Anatomic Contouring: Modern pre-contoured wrist fusion plates are manufactured with a built-in 10 to 15-degree dorsal bend, ensuring optimal functional positioning without the need for intraoperative plate bending.
Step-by-Step Plating Technique
- Exposure: A straight dorsal longitudinal incision is made in line with Lister's tubercle, extending from the distal third of the radius to the base of the third metacarpal.
- Compartment Management: The third dorsal compartment is opened, and the Extensor Pollicis Longus (EPL) is mobilized and retracted radially. The fourth compartment (EDC) is elevated subperiosteally and retracted ulnarly. Lister's tubercle is flattened using a rongeur or burr to create a flat bed for the plate.
- Joint Preparation: The radiocarpal joint (scaphoid lunate, radius), midcarpal joint (capitate), and the third carpometacarpal joint are decorticated. Cancellous bone graft (autograft from the distal radius or allograft) is packed into the interstices.
- Plate Application: A specialized 3.5mm/2.7mm pre-contoured wrist fusion plate is applied dorsally.
- The distal end of the plate is secured to the diaphysis of the third metacarpal using 2.7mm screws.
- The proximal end is secured to the distal radius using 3.5mm screws.
- A dedicated lag screw is often passed through the plate, traversing the radius and compressing directly into the capitate to ensure rigid radiocarpal coaptation.
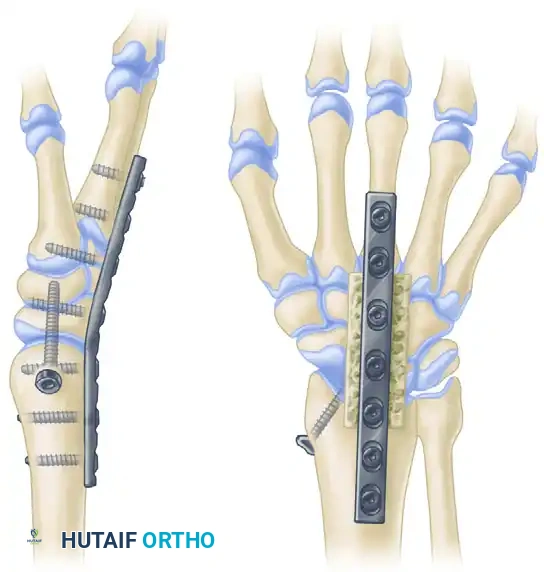
FIGURE 69-81: Arthrodesis of the wrist utilizing a pre-contoured dynamic compression plate. Note the central lag screw providing direct compression across the radiocarpal articulation, and the built-in dorsal extension angle optimizing grip biomechanics.
Clinical Pearl: Third Metacarpal Fixation
When securing the plate to the third metacarpal, ensure the screws are bicortical but do not protrude excessively into the volar soft tissues, as this can cause flexor tendon irritation or rupture.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol varies significantly depending on the surgical technique employed.
Haddad and Riordan Protocol (Non-Rigid Fixation)
- Days 0-14: The patient is immobilized in the initial postoperative sugar-tong splint. Elevation and active digit motion are strictly enforced to prevent edema and stiffness.
- Days 10-14: The initial bandage is changed, and sutures are removed. A solid, well-molded sugar-tong cast is applied to control supination and pronation.
- Weeks 2-6: The sugar-tong cast is worn for an additional 4 weeks.
- Weeks 6-12: The patient is transitioned to a short-arm cast, which is maintained until solid bony union is evident both clinically (absence of pain on stress) and radiographically (trabecular bridging across the fusion mass).
- K-Wire Removal: If supplemental K-wires were used, they are typically removed in the clinic at the 6 to 8-week mark.
AO/ASIF Plating Protocol (Rigid Fixation)
- Days 0-14: A bulky compressive dressing and a volar resting splint are applied. Immediate, aggressive active range of motion of the fingers, thumb, and elbow is initiated on postoperative day one.
- Days 10-14: Sutures are removed. Because the plate provides rigid internal osteosynthesis, prolonged casting is unnecessary. The patient is transitioned to a removable thermoplastic wrist splint.
- Weeks 2-6: The splint is worn for protection during heavy activities and sleep but is removed multiple times daily for hygiene and digit rehabilitation.
- Weeks 6+: Once radiographic consolidation is observed (typically 6-8 weeks), the splint is discontinued, and progressive strengthening is initiated.
COMPLICATIONS AND MANAGEMENT
While total wrist arthrodesis is a highly successful procedure, surgeons must be vigilant regarding potential complications:
- Nonunion / Pseudarthrosis: Most commonly occurs at the third carpometacarpal joint. Risk factors include smoking, inadequate cartilage debridement, and insufficient rigid fixation. Management requires revision plating and supplemental iliac crest bone grafting.
- Hardware Prominence: The dorsal soft tissue envelope of the wrist is thin. Plates, particularly standard straight plates that require manual bending, can irritate the overlying extensor tendons. Extensor tenosynovitis or tendon rupture (especially the EPL or EDC) may necessitate hardware removal once the fusion is solidly united (typically after 12-18 months).
- Ulnocarpal Impaction / DRUJ Pain: As highlighted by Zachary and Stern, failure to address pre-existing DRUJ pathology will result in persistent pain during forearm rotation. Salvage requires a secondary Darrach or Suave-Kapandji procedure.
- Neuroma Formation: Injury to the superficial branch of the radial nerve or the dorsal branch of the ulnar nerve during exposure can lead to debilitating neuropathic pain. Meticulous soft tissue handling and the use of blunt retractors are mandatory.
CONCLUSION
Total wrist arthrodesis is a definitive, durable solution for end-stage wrist arthropathy. Whether utilizing the classic Haddad and Riordan slot-graft technique for complex salvage scenarios or employing modern AO/ASIF dynamic compression plating for rapid rehabilitation, the principles of success remain identical: meticulous joint preparation, precise functional positioning in 15 degrees of dorsiflexion, and rigorous protection of the distal radioulnar joint. Mastery of these techniques ensures the restoration of a stable, powerful, and pain-free hand for the patient.
You Might Also Like

