First MTP Arthroscopy and Hindfoot Endoscopy: A Master Surgical Guide
Key Takeaway
First metatarsophalangeal (MTP) joint arthroscopy and hindfoot endoscopy are advanced, minimally invasive techniques for treating forefoot and hindfoot pathology. This comprehensive guide details the precise surgical steps, portal placements, and biomechanical considerations for first MTP arthroscopy, peroneal and posterior tibial tendoscopy, and endoscopic calcaneoplasty. Utilizing specialized distraction and small-joint instrumentation allows orthopedic surgeons to achieve excellent clinical outcomes while minimizing soft tissue morbidity.
INTRODUCTION TO SMALL JOINT ARTHROSCOPY AND ENDOSCOPY
The evolution of minimally invasive techniques in foot and ankle surgery has fundamentally transformed the management of both forefoot and hindfoot pathology. Historically, surgical intervention for conditions such as hallux rigidus, peroneal tendon subluxation, and Haglund syndrome required extensive open exposures, often leading to significant soft tissue morbidity, prolonged rehabilitation, and a high risk of wound complications.
Today, first metatarsophalangeal (MTP) joint arthroscopy, tendoscopy, and endoscopic calcaneoplasty represent the pinnacle of modern operative orthopaedics. Supported by extensive literature—including foundational work by van Dijk, Ferkel, and Lui—these techniques offer direct visualization of intra-articular and extra-articular structures, allowing for precise débridement, synovectomy, and osteophyte resection. This masterclass provides a rigorous, step-by-step academic guide to these procedures, tailored for the practicing consultant, orthopedic fellow, and resident.
FIRST METATARSOPHALANGEAL JOINT ARTHROSCOPY
The first MTP joint is a complex, dual-articulation structure comprising the metatarsophalangeal and metatarsosesamoid joints. It is subjected to immense biomechanical forces during the terminal stance phase of the gait cycle, bearing up to 119% of total body weight. Consequently, it is highly susceptible to degenerative joint disease (hallux rigidus), osteochondral lesions, and inflammatory arthropathies.
Indications and Patient Selection
Arthroscopy of the first MTP joint is primarily indicated for intra-articular pathology where joint preservation is the goal.
- Early to Moderate Hallux Rigidus: Coughlin and Shurnas Grades I and II, where dorsal impingement is the primary pain generator.
- Osteochondral Defects (OCDs): For evaluation, débridement, and microfracture of the metatarsal head.
- Synovitis and Inflammatory Arthritis: Diagnostic biopsy and therapeutic synovectomy (e.g., rheumatoid arthritis, gouty arthropathy).
- Loose Bodies: Extraction of chondral or osteochondral fragments.
- Unexplained First MTP Pain: Diagnostic arthroscopy following inconclusive advanced imaging (MRI/CT).
Surgical Warning: Advanced hallux rigidus (Grade III/IV) with near-complete loss of joint space and extensive circumferential osteophytes is a relative contraindication for arthroscopy. These patients are better served by arthrodesis or arthroplasty.
Patient Positioning and Setup
Meticulous setup is paramount for successful small joint arthroscopy. The joint space of the first MTP is inherently tight, necessitating continuous, controlled distraction.
- Positioning: Place the patient in the supine position on the operating table. A thigh tourniquet or calf tourniquet is applied to ensure a bloodless field.
- Distraction: Apply a sterile Chinese finger trap to the hallux. Suspend the foot from a distraction tower (identical to those utilized in wrist arthroscopy).
- Traction Force: Apply approximately 10 to 15 pounds of longitudinal traction. This opens the joint space, preventing iatrogenic scuffing of the articular cartilage during instrument insertion.
- Joint Insufflation: Prior to portal placement, inject 2 to 3 mL of normal saline into the joint using a 21-gauge needle to distend the capsule.
Portal Placement and Anatomy
The standard approach utilizes two primary dorsal portals. The extensor hallucis longus (EHL) tendon serves as the central anatomical landmark.
- Dorsomedial Portal: Established just medial to the EHL tendon at the level of the joint line. Care must be taken to avoid the medial dorsal cutaneous nerve.
- Dorsolateral Portal: Established just lateral to the EHL tendon. The surgeon must protect the terminal branches of the deep peroneal nerve and the dorsal venous arch.
Clinical Pearl: Always use a "nick and spread" technique. Incise only the epidermis with a #11 blade, then use a small hemostat to bluntly dissect down to the joint capsule to protect the delicate dorsal neurovascular structures.
Surgical Technique
- Instrumentation: Utilize a 1.9-mm or 2.7-mm, 30-degree short arthroscope. A 2.0-mm or 2.9-mm aggressive shaver is typically required for synovectomy and osteophyte resection.
- Diagnostic Sweep: Introduce the arthroscope through the dorsomedial portal. Perform a systematic 8-point examination: dorsal capsule, medial gutter, lateral gutter, central articular surfaces (metatarsal head and proximal phalanx base), and the plantar metatarsosesamoid articulation.
- Cheilectomy: For hallux rigidus, introduce the shaver or a small arthroscopic burr through the dorsolateral portal. Resect the dorsal osteophyte on the metatarsal head until a smooth contour is achieved and dorsal impingement is eliminated upon passive dorsiflexion.
- Microfracture: If an OCD is identified, débride the lesion to stable vertical margins using a curette, and perform microfracture using a specialized awl or K-wire to stimulate fibrocartilage formation.
TENDOSCOPY OF THE FOOT AND ANKLE
Tendoscopy allows for the endoscopic evaluation and treatment of tendon sheaths, minimizing the scarring and adhesions associated with open tenosynovectomies.
Peroneal Tendoscopy
The peroneal tendons (peroneus longus and brevis) are frequently implicated in lateral hindfoot pain, particularly in athletes.
- Indications: Chronic tenosynovitis, low-grade partial tears, and evaluation of the superior peroneal retinaculum for subluxation.
- Technique: Portals are established along the course of the tendon sheath, typically 1-2 cm distal to the fibular tip and 2-3 cm proximal to the lateral malleolus.
- Groove Deepening: In cases of peroneal dislocation or subluxation, tendoscopy can be utilized to evaluate the retromalleolar groove. Endoscopic groove deepening can be performed using a burr to deepen the fibular sulcus while preserving the fibrocartilaginous floor, followed by thermal shrinkage or repair of the retinaculum.
Posterior Tibial Tendoscopy
Posterior tibial tendon dysfunction (PTTD) is the leading cause of adult-acquired flatfoot deformity.
- Indications: Stage I PTTD (tenosynovitis without deformity) that has failed conservative management.
- Technique: The patient is positioned supine with the leg externally rotated. Portals are placed 1-2 cm distal to the medial malleolus (near the navicular insertion) and 2-3 cm proximal to the malleolus. A 2.7-mm scope is used to perform a thorough tenosynovectomy, removing hypertrophic synovium and assessing for longitudinal split tears.
ENDOSCOPIC CALCANEOPLASTY AND ACHILLES TENDOSCOPY
Endoscopic procedures are highly efficacious for conditions surrounding the Achilles tendon insertion, specifically Haglund's deformity (retrocalcaneal exostosis) and retrocalcaneal bursitis. Clinical literature demonstrates good to excellent results in 80% to 100% of patients undergoing endoscopic calcaneoplasty, with significantly faster recovery times compared to open resection.
Pathoanatomy and Neurovascular Landmarks
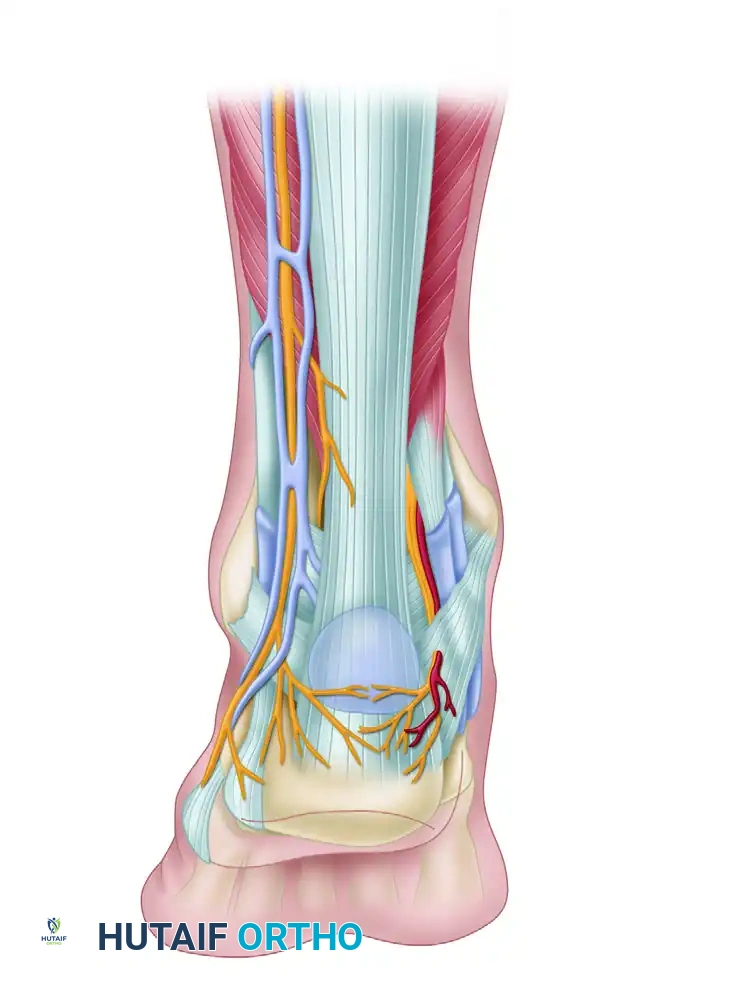
Understanding the posterior ankle anatomy is critical to safely establishing endoscopic portals. The retrocalcaneal space is bordered anteriorly by the posterior calcaneal tuberosity, posteriorly by the Achilles tendon, and superiorly by the deep fascia of the leg.
As illustrated in the anatomical dissection above, the surgeon must navigate a complex neurovascular network:
* Lateral Structures: The sural nerve and lesser saphenous veins course along the posterolateral aspect of the ankle. The lateral calcaneal nerve branch provides sensation to the lateral heel.
* Medial Structures: The tibial nerve and posterior tibial artery lie posteromedially behind the medial malleolus. The medial calcaneal nerve and its branches supply the medial heel.
* Target Area: The retrocalcaneal bursa sits directly between the anterior aspect of the Achilles tendon and the posterosuperior bone spur (Haglund's lesion) of the calcaneus.
Patient Positioning
The patient is placed in the prone position. A thigh tourniquet is applied. The foot is allowed to hang freely over the edge of the operating table, allowing the surgeon to dynamically dorsiflex and plantarflex the ankle to assess impingement during the procedure.
Portal Placement
A two-portal technique is standard for endoscopic calcaneoplasty.
- Lateral Portal: Placed just lateral to the Achilles tendon, at the level of the superior aspect of the calcaneal tuberosity. This portal must be made carefully to avoid the sural nerve.
- Medial Portal: Placed just medial to the Achilles tendon, at the exact same horizontal level as the lateral portal. The scalpel should only penetrate the skin, followed by blunt dissection with a hemostat to avoid the medial calcaneal nerve branches.
Surgical Pitfall: Placing the portals too anteriorly increases the risk of injuring the neurovascular bundles (tibial nerve medially, sural nerve laterally). Portals must remain tightly adjacent to the medial and lateral borders of the Achilles tendon.
Surgical Technique: Endoscopic Calcaneoplasty
- Space Preparation: Introduce a 4.0-mm, 30-degree arthroscope through the lateral portal. Introduce a 4.0-mm shaver through the medial portal.
- Bursectomy: The initial view is often obscured by hypertrophic bursal tissue. Perform a thorough resection of the retrocalcaneal bursa to expose the anterior surface of the Achilles tendon and the posterior calcaneal exostosis.
- Bone Resection: Once the bone spur is clearly visualized, exchange the shaver for a 4.0-mm or 5.5-mm hooded arthroscopic burr.
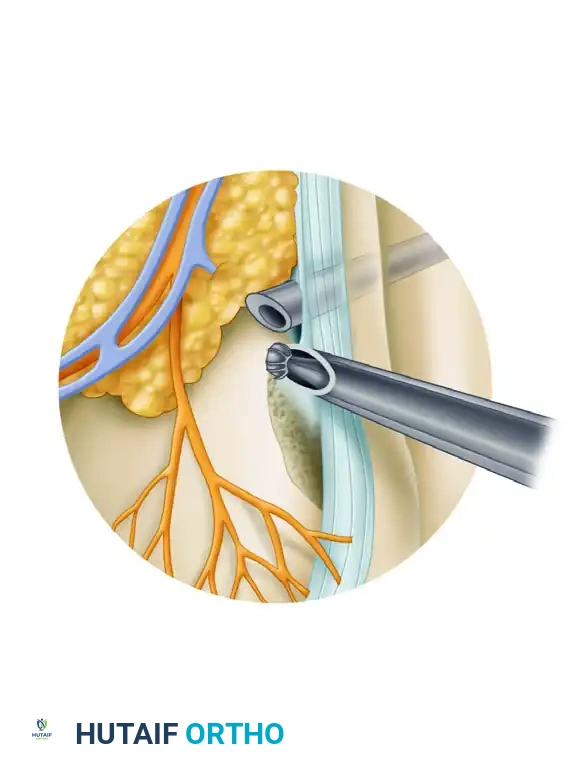
- Excision of Haglund Deformity: As demonstrated in the surgical diagram above, the scope is typically placed through the medial portal while the burr is introduced laterally (or vice versa, depending on the location of the apex of the spur). Resect the posterosuperior prominence of the calcaneus.
- Dynamic Assessment: The resection should extend from medial to lateral until the posterior calcaneus is completely flat. Dorsiflex the ankle fully while viewing the space; there should be no residual impingement between the calcaneus and the anterior Achilles tendon.
- Fluoroscopic Confirmation: It is highly recommended to use intraoperative lateral fluoroscopy to confirm adequate resection of the Haglund deformity before concluding the procedure.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management following small joint arthroscopy and endoscopy is generally accelerated compared to open procedures, though it must be tailored to the specific pathology treated.
First MTP Arthroscopy
- Days 1-14: The patient is placed in a rigid postoperative shoe. Heel-weight-bearing is permitted immediately.
- Weeks 2-6: Sutures are removed at 2 weeks. Aggressive passive and active range of motion (ROM) exercises of the hallux are initiated to prevent capsular adhesions.
- Return to Activity: Transition to normal footwear by week 4. Return to high-impact sports is typically achieved by 6 to 8 weeks, provided there is no pain with terminal dorsiflexion.
Endoscopic Calcaneoplasty
- Days 1-14: The patient is placed in a controlled ankle motion (CAM) boot with a small heel wedge to decrease tension on the Achilles tendon. Weight-bearing as tolerated is allowed.
- Weeks 2-6: The heel wedge is gradually reduced. Physical therapy focuses on eccentric Achilles stretching and strengthening.
- Return to Activity: Running and high-impact activities are generally restricted until 8 to 10 weeks postoperatively, ensuring the tendon insertion has recovered from the adjacent mechanical débridement.
COMPLICATIONS AND AVOIDANCE
While minimally invasive, these procedures carry specific risks that the orthopedic surgeon must meticulously mitigate:
- Nerve Injury: The most common complication in foot and ankle arthroscopy is iatrogenic nerve injury. The superficial peroneal nerve, sural nerve, and medial dorsal cutaneous nerves are at highest risk. Strict adherence to the "nick and spread" portal technique is mandatory.
- Tendon Laceration: Aggressive use of the shaver in tendoscopy or endoscopic calcaneoplasty can result in partial laceration of the Achilles, peroneal, or posterior tibial tendons. Always keep the shaver blade facing away from the tendon substance.
- Inadequate Resection: In endoscopic calcaneoplasty, failure to resect the medial or lateral borders of the calcaneal spur can lead to persistent impingement. Intraoperative fluoroscopy is the gold standard for preventing this pitfall.
- Infection and Wound Healing: Though rare in arthroscopy, diabetic patients and smokers remain at higher risk for portal site necrosis or deep space infection.
CONCLUSION
First metatarsophalangeal joint arthroscopy, tendoscopy, and endoscopic calcaneoplasty are highly effective, evidence-based modalities in the modern orthopedic armamentarium. By mastering the intricate regional anatomy, utilizing precise portal placement, and adhering to strict biomechanical principles, the orthopedic surgeon can achieve superior clinical outcomes, rapid rehabilitation, and high patient satisfaction rates. As technology and instrumentation continue to evolve, the indications for these minimally invasive techniques will undoubtedly expand, further solidifying their role as the standard of care for complex foot and ankle pathology.
You Might Also Like

