Comprehensive Surgical Management of Anterior Shoulder Instability

Key Takeaway
Examination under anesthesia and diagnostic arthroscopy are critical for evaluating anterior shoulder instability. Surgical management requires a tailored approach based on the Instability Severity Index Score (ISIS) and precise anatomical reconstruction. The modified Bankart procedure, utilizing a subscapularis split, provides excellent exposure while protecting the axillary nerve, ensuring optimal capsulolabral repair and restoration of glenohumeral stability.
EXAMINATION USING ANESTHETIC AND ARTHROSCOPY
The evaluation of the unstable shoulder is a complex diagnostic challenge that requires a meticulous synthesis of clinical history, physical examination, and advanced imaging. However, the true extent of capsuloligamentous laxity is often masked by involuntary muscle guarding in the awake patient. Examination under anesthesia (EUA) combined with diagnostic arthroscopy remains the gold standard for confirming the clinical diagnosis and uncovering unsuspected planes of instability, particularly in patients with multidirectional instability patterns.
Biomechanics of Examination Under Anesthesia
During EUA, the elimination of dynamic muscular stabilizers allows the surgeon to isolate and assess the static restraints of the glenohumeral joint.
For the assessment of anterior instability, the patient's arm is abducted, and precise anterior and posterior stress is applied while the scapula is firmly stabilized. In a normal shoulder, minimal anterior translation of the humeral head occurs. The most significant and reliable findings of anterior instability are demonstrable when the arm is placed at 40 degrees and 80 degrees of external rotation. At these positions, the inferior glenohumeral ligament (IGHL) complex is tensioned; failure of this complex allows abnormal translation.
Clinical Pearl: A translation of two grades more than the opposite, uninvolved side yields a 93% sensitivity and a 100% specificity for clinically significant instability. Always compare the affected shoulder to the contralateral side to establish the patient's baseline physiological laxity.
For the assessment of posterior instability, the arm is flexed, adducted, and pushed posteriorly. It is critical to recognize that normal shoulders may permit posterior displacement of up to 50% of the diameter of the glenoid without representing pathological instability. Pathological posterior instability is diagnosed when translation exceeds this physiological norm, particularly if it reproduces a palpable clunk or remains unreduced upon release of the posterior force.
The Role of Diagnostic Arthroscopy
Arthroscopy is seamlessly combined with the EUA and serves as an unparalleled technique for confirming the presence, direction, and severity of shoulder instabilities. The examiner should systematically grade the instability in all planes, remembering that the EUA and arthroscopy are utilized to support—not replace—the clinical history and awake examination.
While some authors advocate for the use of intraoperative fluoroscopy to evaluate the exact amount and direction of displacement, routine fluoroscopy is generally unnecessary for an experienced shoulder surgeon. Arthroscopy should be performed comprehensively to identify all intraarticular pathology, including labral tears, capsular stretching, chondral defects, and loose bodies, so that treatment may be rendered accordingly.
Surgical Warning: Arthroscopy portals and total operative time must be strictly limited during the diagnostic phase. Excessive fluid extravasation into the periarticular soft tissues can severely distort tissue planes, making subsequent open surgical exposure exponentially more difficult and increasing the risk of neurovascular traction injuries.
Advanced Imaging and Pathoanatomy
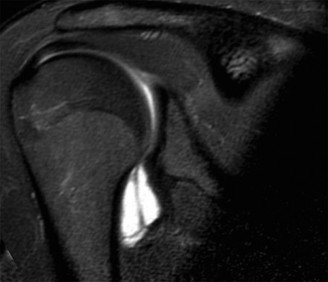
Preoperative magnetic resonance imaging (MRI) or MR arthrography is essential for identifying specific capsuloligamentous injuries. One such critical finding is the Humeral Avulsion of the Glenohumeral Ligament (HAGL) lesion, which can be easily missed if not specifically sought.


Figure 47-32 (A, B, C): MR angiograms demonstrating a HAGL lesion. Note the characteristic J-sign indicating the avulsion of the inferior glenohumeral ligament from its humeral attachment.
ANTERIOR INSTABILITY OF THE SHOULDER
Principles of Surgical Treatment
More than 150 operations and countless modifications have been devised to treat traumatic recurrent anterior instability of the shoulder. There is no single "best" procedure; rather, the optimal operation is the one that addresses the specific pathoanatomy of the individual patient.
Factors that have been universally stressed as critical in achieving a successful result are adequate surgical exposure and meticulous, accurate surgical technique. The pathological condition must be precisely defined, and a procedure must be selected that corrects this condition as anatomically as possible.
Ideally, the chosen procedure for recurrent instability should fulfill the following criteria:
1. Has a low recurrence rate.
2. Has a low complication rate.
3. Has a low reoperation rate.
4. Does no harm (specifically, avoids over-constraining the joint which leads to secondary osteoarthritis).
5. Maintains physiological range of motion, particularly external rotation.
6. Is applicable in the vast majority of cases.
7. Allows direct observation of the joint pathology.
8. Corrects the specific anatomical defect.
9. Is technically reproducible.
Operative procedures can be performed open or arthroscopically with comparable long-term results, provided patient selection is appropriate. When the appropriate procedure is accomplished to restore the anatomy, outcomes of Bankart repairs are heavily influenced by preoperative risk factors.
The Instability Severity Index Score (ISIS)
To guide surgical decision-making between arthroscopic and open stabilization, Balg and Boileau developed the Instability Severity Index Score (ISIS). This scoring system evaluates preoperative prognostic factors to predict the risk of recurrence following an arthroscopic Bankart repair.
Table 47-6: Instability Severity Index Score (ISIS)
* Age at surgery (yr): < 20 years (2 points) | > 20 years (0 points)
* Degree of sport participation: Competitive (2 points) | Recreational or none (0 points)
* Type of sport: Contact or forced overhead (1 point) | Other (0 points)
* Shoulder hyperlaxity: Anterior or inferior hyperlaxity present (1 point) | Normal laxity (0 points)
* Hill-Sachs lesion (AP radiograph): Visible in external rotation (2 points) | Not visible in external rotation (0 points)
* Glenoid loss of contour (AP radiograph): Loss of contour present (2 points) | No lesion (0 points)
* Total Maximum Score: 10 points
Clinical Application: A score of over 3 to 6 points suggests a higher risk of recurrence with isolated arthroscopic soft-tissue repair, often prompting the surgeon to consider an open procedure or a bone-block augmentation (e.g., Latarjet).
Algorithm for Preferred Surgical Treatment
At present, the preferred surgical procedures for isolated soft-tissue injuries without significant bone loss are arthroscopic Bankart repairs or capsular plication procedures. When an open procedure is indicated, the Jobe capsulolabral reconstruction or Neer capsular shift is preferred for anterior instability, and a glenoid-based shift is utilized for posterior instability.
Table 47-7: Preferred Surgical Treatment Algorithm
* Traumatic Bankart: Jobe capsulolabral reconstruction.
* Acute Bony Bankart: Screw or anchor fixation.
* Hyperlaxity: Rotator interval closure.
* HAGL Lesion: Suture anchor repair (open or arthroscopic).
* Multidirectional Instability: Repair Bankart/Kim lesions; Anterior-inferior prominent requires a Neer capsular shift (humeral side); Posterior prominent requires a glenoid side shift.
* Glenoid Bone Loss:
* Erosional bone loss > 25%: Latarjet procedure.
* Erosional bone loss > 40%: Eden-Hybinette procedure (iliac crest bone graft).
* Humeral Head Bone Loss (Hill-Sachs):
* 20% + glenoid defect or hyperlaxity: Jobe capsular reconstruction + capsular shift + interval closure to decrease rotation, or arthroscopic remplissage.
* 25% (approx. 6 mm deep): Arthroscopic Remplissage.
* 40%: Latarjet procedure to indirectly treat the defect by increasing the glenoid rotational arc.
* Anterior humeral head > 30%: McLaughlin procedure.
* Capsular Deficiency: Achilles tendon allograft capsular reinforcement.
THE BANKART OPERATION
Historical Context and Original Technique
In the original Bankart operation, the subscapularis tendon and the underlying shoulder capsule are opened vertically. The lateral leaf of the capsule is reattached directly to the anterior glenoid rim. A medial leaf of the capsule is then imbricated over the lateral leaf, and the subscapularis is approximated.
The Bankart operation is strictly indicated when the labrum and the capsule are separated from the glenoid rim (the classic Bankart lesion) or if the anterior capsule is pathologically thin and redundant. The primary advantage of this historical procedure is that it corrects the labral defect and imbricates the capsule without requiring any metallic internal fixation devices, which were prone to catastrophic complications in the past. The main disadvantage of the original procedure is its significant technical difficulty and the morbidity associated with complete subscapularis detachment.
Modern Modifications and the Subscapularis Split
Since the original description of the Bankart procedure, numerous modifications have allowed the operation to be performed with greater ease, enhanced anatomical precision, and significantly less surgical trauma.
To minimize morbidity, the procedure can be performed through a subscapularis split rather than a complete tenotomy. In larger, more muscular individuals where a simple split provides inadequate exposure, the subscapularis split can be extended superiorly approximately 1 cm medial to the biceps tendon, releasing the subscapularis muscle in an L-shaped fashion.
This L-type release provides excellent, wide exposure of the rotator interval. The inferior third of the subscapular muscle can be safely retracted inferiorly to expose the inferior capsule, while simultaneously protecting the axillary nerve and the anterior humeral circumflex vessels (the "three sisters").
Surgical Pearl: The subscapularis split approach preserves the neuromuscular integrity of the subscapularis and virtually eliminates the possibility of postoperative tendon detachment or catastrophic subscapularis failure—a known complication of traditional vertical tenotomies.
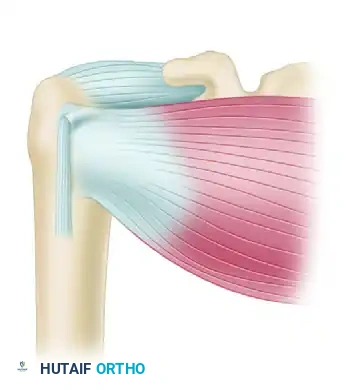
Figure 47-33 (A): Division of the subscapularis tendon. The lower fourth of the subscapularis tendon is left intact to protect the anterior humeral circumflex artery and the axillary nerve.
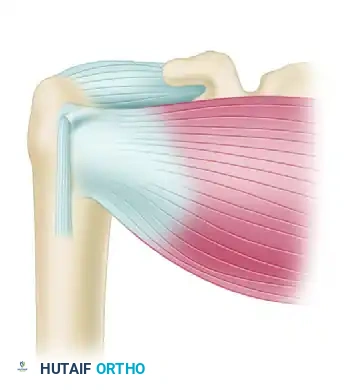
Figure 47-33 (B): The subscapularis muscle is split horizontally in line with its fibers and retracted superiorly and inferiorly to expose the underlying redundant joint capsule.
The Modified Open Bankart Procedure (Montgomery and Jobe)
A procedure similar to that described by Montgomery and Jobe has been utilized with high success rates for more than a decade. It is highly effective for both recurrent traumatic dislocations and recurrent microtraumatic subluxations presenting with anterior and inferior instability. Notably, it is rarely necessary to osteotomize the coracoid process to obtain adequate exposure when utilizing this modified approach.
Keys to Surgical Success:
1. Maximizing Healing Potential: The anterior scapular neck must be meticulously decorticated and abraded to a bleeding bone bed to promote robust soft-tissue-to-bone healing.
2. Restoring Glenoid Concavity: The labral bumper must be recreated to restore the concavity-compression mechanism of the glenohumeral joint.
3. Anatomical Capsular Fixation: The capsule must be secured exactly at the articular margin of the anterior glenoid rim. Medialization of the repair on the scapular neck will result in persistent laxity and recurrent instability.
4. Re-creating Physiological Capsular Tension: This is achieved through precise superior and inferior capsular advancement and imbrication (a capsular shift), eliminating the redundant inferior pouch.
5. Supervised Goal-Oriented Rehabilitation: Surgery is only half the treatment. A strict, phased postoperative rehabilitation protocol is mandatory to protect the repair while gradually restoring functional range of motion and dynamic muscular control.
Postoperative Protocol
Following an open capsulolabral reconstruction, the patient is placed in a sling with the arm in internal rotation.
* Phase I (0-4 weeks): Absolute protection of the repair. Passive forward flexion is allowed up to 90 degrees, but external rotation is strictly limited to neutral (0 degrees) to prevent tension on the anterior capsular repair and the subscapularis split.
* Phase II (4-8 weeks): The sling is discontinued. Active-assisted and active range of motion begins. External rotation is gradually progressed by 10-15 degrees per week.
* Phase III (8-12 weeks): Strengthening of the rotator cuff and periscapular stabilizers is initiated.
* Phase IV (3-6 months): Return to sport-specific activities is permitted only when full, painless range of motion is achieved, and dynamic strength is at least 90% of the contralateral shoulder. Contact athletes may require 6 months before returning to unrestricted play.
📚 Medical References
- anterior shoulder instability: when and why? J Bone Joint Surg 87A:419, 2005.
- Miniaci A, MacLeod M: Transfer of the latissimus dorsi muscle after failed repair of a massive tear of the rotator cuff: a two to fi ve-year review, J Bone Joint Surg 81A:1120, 1999.
- Misamore GW, Ziegler DW, Rushton JL: Repair of the rotator cuff: a comparison of results in two populations of patients, J Bone Joint Surg 77A:1335, 1995.
- Moren-Hybbinette I, Moritz U, Schersten B: The clinical picture of the painful diabetic shoulder: natural history, social consequences and analysis of concomitant hand syndrome, Acta Med Scand 221:73, 1987.
- Morrison DS, Bigliani LU: The clinical signifi cance of variations in acromial morphology, Orthop Trans 11:234, 1987.
- Moseley HF, Goldie I: The arterial pattern of the rotator cuff of the shoulder, J Bone Joint Surg 45B:780, 1963.
- Mudge MK, Wood VE, Frykman GK: Rotator cuff tears associated with os-acromiale, J Bone Joint Surg 66A:427, 1984.
- Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion defi cits and posterior shoulder tightness in throwers with pathologic internal impingement, Am J Sports Med 34:385, 2006.
- Nam EK, Synder SJ: The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions, Am J Sports Med 31:798, 2003.
- Nasca RJ: The use of freeze-dried allografts in the management of global rotator cuff tears, Clin Orthop Relat Res 228:218, 1988.
- Neault MA, Gunache CA: Arthroscopic rotator cuff repair, Oper Tech Sports Med 10:93, 2002.
- Neer CS II: Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report, J Bone Joint Surg 54A:41, 1972.
- Neer CS II: Impingement lesions, Clin Orthop Relat Res 173:70, 1983.
- Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy, J Bone Joint Surg 65A:1232, 1983.
- Neer CS, Marberry TA: On the disadvantages of radical acromionectomy, J Bone Joint Surg 63A:416, 1981.
- Neer CS II, Poppen NK: Supraspinatus outlet, Orthop Trans 11:234, 1987.
- Neer CS II, Sutterlee CC, Palsey RM, et al: On the value of the coracohumeral ligament release. In Post M, Morrey BE, Hawkins RJ, eds: Surgery of the shoulder, St Louis, 1990, Mosby. Neibauer JS: Acromial splitting incision for repair of shoulder capsule, J Bone Joint Surg 60A:681, 1987.
- Neviaser JS: Adhesive capsulitis of the shoulder, J Bone Joint Surg 27:211, 1945.
- Neviaser JS, Neviaser RJ, Neviaser TJ: The repair of chronic massive ruptures of the rotator cuff of the shoulder by use of a freeze-dried rotator cuff, J Bone Joint Surg 60A:681, 1978.
- Neviaser RJ: Tears of the rotator cuff, Orthop Clin North Am 11:295, 1980.
- Neviaser RJ, Neviaser TJ: Transfer of subscapularis and teres minor for massive defects of rotator cuff. In Bayley I, Kessel L, eds: Shoulder surgery, Berlin, 1982, Springer-Verlag. Neviaser RJ, Neviaser TJ: Reconstruction of chronic tears of the rotator cuff. In Bateman JE, Welsh RP, eds: Surgery of the shoulder, Philadelphia, 1984, Decker. Neviaser RJ, Neviaser TJ: Reoperation for failed rotator cuff repair: analysis of 46 cases, Orthop Trans 13:509, 1989.
- Neviaser RJ, Neviaser TJ, Neviaser JS: Concurrent rupture of the rotator cuff and anterior dislocation of the shoulder in the older patient, J Bone Joint Surg 70A:1308, 1988.
- Nicholson GP: Treatment of anterior-superior shoulder instability with a reverse ball and socket prosthesis, Oper Tech Orthop 13:235, 2003.
- Nirschl RP: Rotator cuff tendinitis: basic concepts of pathoetiology, Instr Course Lect 38:439, 1989.
- Nofsinger CC, Williams GR Jr, Iannotti JP: Calcifi c tendinitis of the trapezius insertion, J Shoulder Elbow Surg 8:162, 1999.
- Norwood LA, Barrack R, Jacobson KE: Clinical presentation of complete tears of the rotator cuff, J Bone Joint Surg 71A:499, 1989.
- Nottage WM: Rotator cuff repair with or without acromioplasty, Arthroscopy 19(suppl 1):229, 2003.
- O’Brien SJ, Schwartz RS, Warren RF, et al: Capsular restraints to anterior-posterior motion of the abducted shoulder: a biomechanical study, J Shoulder Elbow Surg 4:298, 1995.
- Ogata S, Uhthoff HK: Acromial enthesopathy and rotator cuff repair: a radiologic and histologic post mortem investigation of the coracoacromial arch, Clin Orthop Relat Res 254:39, 1990.
- Ogilvie-Harris DJ, Biggs DJ, Fitsialos DP, et al: The resistant frozen shoulder: manipulation versus arthroscopic release, Clin Orthop Relat Res 319:238, 1995.
- Ogilvie-Harris DJ, Demaziere A: Arthroscopic debridement versus open repair for rotator cuff tears: a prospective cohort study, J Bone Joint Surg 75B:416, 1993.
- Ong BC, Sekiya JK, Rodosky MW: Open techniques for repair of large and massive rotator cuff tears, Oper Tech Sports Med 10:69, 2002.
- Ozaki J, Fujimoto S, Nakagawa Y, et al: Tears of the rotator cuff of the shoulder associated with pathologic changes of the acromion: a study in cadavers, J Bone Joint Surg 70A:1224, 1988.
- Paavolainen P, Slatis P, Bjorkenheim JM: Transfer of the tuberculum majus for massive ruptures of the rotator cuff. In Post M, Morrey BF, Hawkins RJ, eds: Surgery of the shoulder , St Louis, 1990, Mosby. Pal B, Anderson J, Dick WC, et al: Limitation of joint mobility and shoulder capsulitis in insulin and non-insulin-dependent diabetes mellitus, Br J Rheumatol 25:147, 1987.
- Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic fi ndings in the overhead throwing athletes: evidence for posterior internal impingement of the rotator cuff, Arthroscopy 16:35, 2000.
- Park HB, Yokota A, Gill HS, et al: Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome, J Bone Joint Surg 87A:1446, 2005.
- Patte D, Goutallier D, Scheffer JC: Large cuff ruptures: repair results by muscle advancement. In Post M, Morrey BF, Hawkins RJ, eds: Surgery of the shoulder, St Louis, 1990, Mosby. Pattee CA, Snyder SJ: Sonographic evaluation of the rotator cuff: correlation with arthroscopy, Arthroscopy 4:15, 1988.
- Patterson RL, Darrach W: Treatment of acute bursitis by needle irrigation, J Bone Joint Surg 19:993, 1937.
- Paulos LE, France EP, Harner CO: Biomechanical evaluation of rotator cuff fi xation methods. In Post M, Morrey BF, Hawkins RJ, eds: Surgery of the shoulder, St Louis, 1990, Mosby. Payne LZ, Altchek DW, Craig EV, et al: Arthroscopic treatment of partial rotator cuff tears in young athletes: a preliminary report, Am J Sports Med 25:299, 1997.
- Pearle AD, Kelly BT, Voos JE, et al: Surgical technique and anatomic study of latissimus dorsi and teres major transfers, J Bone Joint Surg 88A:1524, 2006.
- Pearsall AW, Osbahr DC, Speer KB: An arthroscopic technique for treating patients with frozen shoulder, Arthroscopy 15:2, 1992.
- Peterson CJ, Gentz CF: Ruptures of the supraspinatus tendon: the signifi cance of distally pointing acromioclavicular osteophytes, Clin Orthop Relat Res 174:143, 1983.
- Pinguad, Charlot: Scapulagie. In Dechambre: Dictionaire encyclopédique des sciences medicales, vol 2, Paris, 1879.
- Placzek JD, Roubal RJ, Kulig K, et al: Theory and technique of translational manipulation for adhesive capsulitis, Am J Orthop 33:173, 2004.
- Post M: Rotator cuff repair with carbon fi lament polylactic acid, Clin Orthop Relat Res 196:154, 1985.
- Post M: Diagnosis and treatment of suprascapular nerve entrapment, Clin Orthop Relat Res 368:92, 1999.
- Post M, Mayer J: Suprascapular nerve entrapment, Clin Orthop Relat Res 223:126, 1987.
- Post M, Silver R, Singh M: Rotator cuff tear: diagnosis and treatment, Clin Orthop Relat Res 173:78, 1983.
- Pouliart N, Gagey O: Reconciling arthroscopic and anatomic morphology of the humeral insertion of the inferior glenohumeral ligament, Arthroscopy 21:979, 2005.
- Rathbun JB, Macnab I: The microvascular pattern of the rotator cuff, J Bone Joint Surg 52B:540, 1970.
- Reed SC, Glossop N, Ogilvie-Harris DJ: Full-thickness rotator cuff tears: a biomechanical comparison of suture versus bone anchor techniques, Am J Sports Med 24:46, 1996.
- Resch H, Povacz P, Ritter E, et al: Transfer of the pectoralis major muscle for the treatment of irreparable rupture of the subscapularis tendon, J Bone Joint Surg 82A:372, 2000.
- Rizk TE, Pinals RS: Frozen shoulder, Semin Arthritis Rheum 11:440, 1982.
- Rizk TE, Pinals RS: Histocompatibility type and racial incidence in frozen shoulder, Arch Phys Med Rehabil 65:33, 1984.
- Rockwood CA: The role of anterior impingement in lesions of the rotator cuff, J Bone Joint Surg 62B:274, 1980.
- Rockwood CA: The management of patients with massive rotator cuff defects by acromioplasty and rotator cuff debridement, Orthop Trans 10:622, 1986.
- Rockwood CA, Williams GR, Burkhead WZ: Debridement of massive, degenerative lesions of the rotator cuff. Paper presented at the Seventh Open Meeting of the American Shoulder and Elbow Surgeons, Anaheim, Calif, 1991.
- Rodosky MW, Bigliani LU: Indications for glenoid resurfacing in
You Might Also Like