Antiprotrusio Cages: Key to Hip Arthroplasty with Acetabular Loss

Key Takeaway
This topic focuses on Antiprotrusio Cages: Key to Hip Arthroplasty with Acetabular Loss, Hip arthroplasty with acetabular reconstruction involves addressing bone deficiency, which can be primary (e.g., dysplasia) or secondary (e.g., component loosening or osteolysis). For massive secondary bone stock deficiency where a standard cementless acetabular component cannot achieve reliable initial stability, antiprotrusio cages are indicated to provide critical support and fixation, enhancing the stability and outcome of the surgery.
Introduction and Epidemiology
Acetabular bone deficiency presents one of the most formidable challenges in revision total hip arthroplasty (THA). This deficiency may occur primarily due to conditions such as developmental dysplasia of the hip, inflammatory arthritis, or seronegative arthropathy. Alternatively, and more commonly in the contemporary revision setting, it presents secondarily. Secondary causes include aseptic or septic loosening of primary acetabular components, particulate-induced osteolysis, periprosthetic trauma, or iatrogenic bone loss during the extraction of well-fixed cementless components.

The primary goal of acetabular reconstruction is the restoration of the anatomic center of rotation, achieving rigid initial stability of the implant, and establishing a construct that allows for long-term biologic fixation or durable mechanical support. In cases of mild to moderate bone loss (Paprosky Types I and II), hemispherical porous-coated cementless cups, often supplemented with multiple screws, provide excellent long-term survivorship. However, the use of antiprotrusio cages is indicated in situations where an uncemented porous-coated acetabular component will not gain reliable initial stability due to massive structural failure of the acetabular rim or profound medial wall defects.

Antiprotrusio cages, such as the Burch-Schneider or Ganz reinforcement rings, are designed to span massive segmental and cavitary defects. By mechanically bridging the deficient acetabulum, these devices transfer physiological loads from the prosthetic joint directly to the remaining intact host bone of the ilium and ischium. This mechanical bypass protects underlying morcellized or structural allograft, allowing for graft incorporation while providing a stable foundation for the cemented polyethylene liner.

The epidemiology of revision THA utilizing antiprotrusio cages typically involves an older, more medically complex patient population with a history of multiple prior hip surgeries. As the aggregate number of primary THAs performed globally continues to rise, the absolute burden of complex revisions involving catastrophic bone loss or pelvic discontinuity is concomitantly increasing, necessitating a thorough understanding of cage reconstruction techniques among arthroplasty surgeons.
Surgical Anatomy and Biomechanics
Osteology of the Acetabulum
The acetabulum is a hemispherical cavity formed by the embryologic confluence of the ilium, the ischium, and the pubis at the triradiate cartilage. Each of these innominate bone components contributes to the complex three-dimensional architecture of the anterior and posterior walls and columns. The anterior column extends from the iliac crest to the pubic symphysis, while the posterior column extends from the sciatic notch to the ischial tuberosity.

Critical surgical landmarks for acetabular reconstruction include the anterior and posterior walls, the superior dome, and the medial wall "teardrop." The teardrop represents the confluence of the medial acetabular wall and the quadrilateral plate, serving as a vital radiographic marker for the native center of rotation and the inferior margin of the acetabulum. The normal acetabulum is oriented with approximately 45 degrees of inclination and 15 degrees of anteversion relative to the true pelvic plane.

Biomechanical Principles of Antiprotrusio Cages
The fundamental biomechanical principle of the antiprotrusio cage is load distribution. In the presence of massive uncontained defects, physiological weight-bearing forces would cause medial migration (protrusio) or superior migration of a standard hemispherical cup.

The cage acts as a structural bridge. The superior flange is contoured and fixed with screws to the dense cortical bone of the ilium, while the inferior flange is slotted into or fixed against the ischium. This configuration bypasses the deficient medial wall and acetabular columns, transferring joint reactive forces to the robust native pelvis.

Furthermore, the cage serves a crucial biological function by acting as a mechanical shield for underlying bone graft. In the technique of impaction bone grafting (IBG), the cage protects the healing allograft from excessive shear and compressive forces, facilitating gradual creeping substitution and restoration of host bone stock over time.
Indications and Contraindications
Acetabular bone deficiency may occur primarily due to dysplasia, but this type of deficiency usually does not require the use of an antiprotrusio cage, as standard cementless components placed at the true anatomic center or a high hip center are often sufficient. Certain conditions, such as rheumatoid arthritis, juvenile idiopathic arthritis, ankylosing spondylitis, and Paget disease, may predispose to acetabular protrusio but also typically do not require an antiprotrusio cage if the peripheral rim remains intact.
The antiprotrusio cage is most frequently utilized in cases of secondary bone stock deficiency so massive that the use of a cementless press-fit acetabular component is precluded. This corresponds primarily to Paprosky Type IIIA and Type IIIB defects, as well as select cases of pelvic discontinuity when combined with posterior column plating.

Operative Versus Non Operative Management of Acetabular Defects
| Clinical Scenario | Recommended Management Strategy | Rationale and Considerations |
|---|---|---|
| Paprosky Type I / IIA / IIB | Standard Cementless Hemispherical Cup | >50% host bone contact allows for reliable biologic ingrowth. |
| Paprosky Type IIC | Cementless Cup with Medial Wall Bone Graft | Medial wall is deficient but rim is intact; graft prevents protrusio. |
| Paprosky Type IIIA | Jumbo Cup, Trabecular Metal Augments, or Cage | Severe superior migration. Rim is deficient. Cages used if <50% host bone contact is achievable with modern porous metals. |
| Paprosky Type IIIB | Antiprotrusio Cage or Custom Triflange | Massive uncontained defect. Ischial lysis present. Cage spans defect from ilium to ischium. |
| Pelvic Discontinuity | Cup-Cage Construct, Custom Triflange, or Cage with Plating | Disassociation of superior and inferior pelvis. Requires rigid internal fixation and spanning construct. |
| Active Periprosthetic Joint Infection | Two-Stage Exchange (Explantation and Spacer) | Absolute contraindication to definitive cage reconstruction until infection is eradicated. |
| Medically Unfit / Non-Ambulatory | Resection Arthroplasty (Girdlestone) or Observation | High surgical morbidity of complex revision outweighs benefits in non-ambulatory patients. |

Contraindications to the use of an antiprotrusio cage include active periprosthetic joint infection, inadequate iliac or ischial bone stock to support the flanges of the cage, and severe medical comorbidities that preclude a lengthy and hemodynamically demanding surgical procedure.
Pre Operative Planning and Patient Positioning
Clinical Evaluation
The natural history of massive acetabular bone defects requiring an antiprotrusio cage is progressive pain and functional decline. Patients invariably require revision surgery to return to functional activities.

The clinical history must be meticulously directed to determine whether the source of pain is extrinsic or intrinsic to the hip joint. The patient's pain may be extrinsic, stemming from lumbar radiculopathy, spinal stenosis, or intrapelvic pathology. In such cases, revision hip surgery may fail to relieve pain completely. Intrinsic pain is usually, but not always, located in the groin and exacerbated by weight-bearing. Start-up pain is a characteristic clinical indication of component loosening.

Infection must always be assessed with careful questioning regarding previous infections, fevers, chills, wound drainage, and pain at rest. Medical comorbidities must be rigorously evaluated to determine the presence of any conditions that may compromise the outcome of the surgery or place the patient at an increased risk of perioperative complications.
Physical examination should include a visual inspection of the skin for the placement of prior incisions and signs of infection. The appropriate incision for the surgical approach must be utilized, ensuring an adequate (minimum 6 cm) skin bridge between prior incisions to prevent full-thickness skin necrosis.
Imaging and Diagnostic Workup
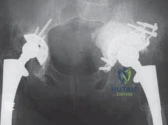
Plain radiographs, including an anteroposterior (AP) view of the pelvis, and AP and true lateral views of the hip, should be obtained to classify bone loss and to adequately plan the procedure preoperatively. Judet views (iliac and obturator obliques) are highly recommended to assess the integrity of the anterior and posterior columns.

Computed tomography (CT) scans with metal artifact reduction sequence (MARS) protocols are essential to assess the remaining bone stock. This is especially important in cases of severe superior or posterior bone loss that may require structural allograft reconstruction. The CT scan helps determine the volume of morcellized allograft required, the need for structural bone, and dictates the surgical approach if posterior column plating is necessary.

CT scans with intravascular contrast are highly useful in situations where a prior implant has migrated medial to Kohler’s line and the proximity of the implant to the external iliac vessels and intra-abdominal contents is unknown. This allows for the involvement of a vascular surgeon if intrapelvic exploration is required.

Laboratory and Nuclear Medicine Studies
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are mandatory screening tools to detect occult periprosthetic joint infection. Aspiration of the hip to assess for infection (synovial fluid WBC count, polymorphonuclear percentage, and cultures) is highly valuable if either the ESR, CRP, or clinical suspicion is elevated.

In complex diagnostic scenarios, nuclear medicine studies such as technetium Tc 99m methylene diphosphonate bone scans in combination with gallium citrate, indium 111–labeled leukocyte scans, positron emission tomographic scans with 18F-fluorodeoxyglucose (PET-FDG), and sulfur colloid scans may help differentiate aseptic loosening from septic failure.

Patient positioning depends heavily on the chosen surgical approach. The lateral decubitus position is standard for posterolateral or direct lateral approaches, utilizing rigid pelvic fixation devices to allow for accurate intraoperative assessment of component version and inclination.
Detailed Surgical Approach and Technique
Surgical Exposure and Explantation
The surgical approach must provide extensile access to the ilium, ischium, and the entire acetabular rim. A posterolateral approach is most commonly utilized, often combined with an extended trochanteric osteotomy (ETO). The ETO provides unparalleled visualization of the acetabulum, facilitates the safe extraction of distally well-fixed femoral stems, and protects the abductor mechanism from excessive traction injury during complex acetabular reconstruction.

Following arthrotomy and dislocation, the failed acetabular component is carefully explanted. Explantation must be performed meticulously using curved gouges, osteotomes, or specialized explant systems (e.g., Explant) to preserve all remaining host bone.

Once the implant is removed, aggressive debridement of the reactive pseudocapsule and all particulate-induced granulomatous tissue is performed. This exposes the true extent of the cavitary and segmental bone defects. The host bone is then sequentially reamed to bleeding subchondral bone to create a vascularized bed for bone graft incorporation. Care must be taken to avoid over-reaming, which could further compromise the medial wall or columns.

Bone Grafting Techniques
Reconstruction of the bone stock is a critical step prior to cage insertion. Massive cavitary defects are managed with impaction bone grafting (IBG). Fresh-frozen allograft femoral heads are milled into 8 to 10 mm chips. The graft is washed to remove marrow elements and fat, thereby enhancing its osteoconductive potential.

The morcellized graft is introduced into the cavitary defects and vigorously impacted using specialized tamps and reverse-reaming techniques. This creates a dense, mechanically stable neo-acetabulum. If massive uncontained segmental defects are present, structural allografts (such as a distal femur or femoral head) may be contoured and fixed to the host bone with screws to contain the morcellized graft.
Cage Selection, Contouring, and Insertion
The appropriate antiprotrusio cage is selected based on templating and intraoperative trialing. The cage must be carefully contoured using heavy bending irons to match the specific topography of the patient's hemipelvis.

The inferior flange is typically inserted first. In a Burch-Schneider configuration, the inferior flange is slotted into the ischium. A precise osteotomy is made in the ischium to accept the flange, ensuring it does not protrude posteriorly where it could impinge upon the sciatic nerve.

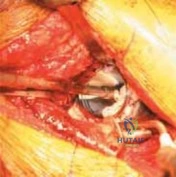
Once the ischial flange is seated, the cage is impacted into the prepared acetabular bed, compressing the underlying bone graft. The superior flange is then brought into intimate contact with the lateral cortex of the ilium.
Fixation and Cementation
Rigid internal fixation is paramount. Multiple 6.5 mm cancellous or cortical screws are placed through the superior flange into the dense bone of the iliac wing. Additional screws are placed through the dome of the cage into the safe zones of the acetabulum (the posterosuperior and posteroinferior quadrants, avoiding the anterior quadrants to prevent injury to the external iliac and obturator neurovascular bundles).

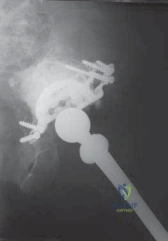
Following rigid fixation of the cage, the construct is thoroughly irrigated and dried. A highly cross-linked all-polyethylene acetabular liner is then cemented into the cage. The cement is pressurized into the cage's metallic mesh or perforations. The surgeon must meticulously control the version and inclination of the polyethylene liner during cement curing, targeting 40-45 degrees of inclination and 15-20 degrees of anteversion, independent of the orientation of the underlying cage.
Complications and Management
The use of antiprotrusio cages in the setting of massive acetabular defects is a salvage procedure associated with a significantly higher complication profile compared to primary THA or less complex revisions.

Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage Strategies and Management |
|---|---|---|---|
| Aseptic Loosening / Cage Failure | 10% - 25% at 10 years | Fatigue fracture of the superior flange, failure of graft incorporation, inadequate initial fixation. | Revision to a custom triflange acetabular component (CTAC) or modern cup-cage construct. |
| Instability / Dislocation | 5% - 15% | Altered abductor mechanics, impingement, malposition of the cemented liner. | Closed reduction. If recurrent, revision of the cemented liner to a constrained geometry or dual mobility bearing. |
| Periprosthetic Joint Infection | 3% - 8% | Prolonged operative time, massive dead space, poor soft tissue envelope, multiple prior surgeries. | Acute: DAIR (Debridement, Antibiotics, Implant Retention). Chronic: Two-stage exchange arthroplasty. |
| Sciatic Nerve Palsy | 2% - 6% | Retractor injury, lengthening of the limb, direct trauma from posterior ischial flange placement. | Removal of offending hardware if direct compression exists. Ankle-foot orthosis (AFO) and observation. |
| Vascular Injury | < 1% | Screw penetration into anterior quadrants, aggressive medial wall debridement. | Immediate intraoperative vascular surgery consultation, packing, and formal vascular repair. |

Meticulous surgical technique, particularly regarding the contouring of the cage and the placement of the ischial flange, is critical to minimizing these complications. The ischial flange must be deeply seated within the bone to avoid posterior prominence, which is a classic cause of delayed sciatic neuropathy.

Post Operative Rehabilitation Protocols
Postoperative rehabilitation following antiprotrusio cage reconstruction is significantly more conservative than following primary THA. The primary objective during the initial postoperative phase is to protect the mechanical construct from excessive shear forces while facilitating the early stages of biological incorporation of the massive structural and morcellized allografts.
Patients are typically restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) on the operative extremity for a minimum of 6 to 12 weeks. Radiographic evaluation is performed at 6 weeks to assess for hardware migration or failure.

Hip precautions are strictly enforced, tailored to the surgical approach utilized. If an extended trochanteric osteotomy was performed, active hip abduction is restricted until radiographic evidence of osteotomy union is observed. Deep vein thrombosis (DVT) prophylaxis is mandatory, typically utilizing low-molecular-weight heparin or direct oral anticoagulants for 28 to 35 days, coupled with mechanical prophylaxis, given the prolonged period of restricted mobility.
Summary of Key Literature and Guidelines
The historical evolution of the antiprotrusio cage is rooted in the pioneering work of Burch, Schneider, and Ganz. Long-term survivorship data for these devices demonstrate their efficacy as a durable salvage option. Studies by Berry et al. and Gill et al. have shown 10-year survivorship rates ranging from 75% to 85% when utilized for severe bone loss, though survivorship precipitously declines in the presence of un-plated pelvic discontinuity.
In the contemporary era, the indications for standalone antiprotrusio cages are evolving. The advent of highly porous metals
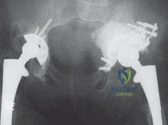
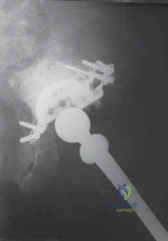
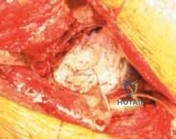
Clinical & Radiographic Imaging