Revision Hip Success: Unpacking The Case Title Acetabular Grafting
Key Takeaway
This article provides essential research regarding Revision Hip Success: Unpacking The Case Title Acetabular Grafting. Acetabular impaction grafting, detailed in this case title, treats a loosened hip replacement with a large acetabular bone defect. The procedure reconstructs the acetabulum using metallic meshes and morselized bone allograft, followed by cementing a new cup. This restores hip function for patients experiencing groin pain and walking restrictions, such as a 78-year-old female.
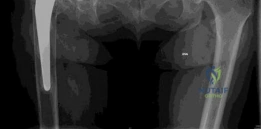
You are presented with this 82-year-old male 15 years post-primary THA. He has progressive groin pain and instability. Examine the provided radiograph and describe your findings. What is the most likely diagnosis?
Candidate: The radiograph shows a cementless THA with superior and medial migration of the acetabular component. There is clear evidence of osteolysis with radiolucent lines in the DeLee and Charnley zones. The medial wall has breached the Kohler line, suggesting protrusio. The femoral component appears well-fixed. The clinical and radiographic presentation is classic for aseptic loosening secondary to particulate wear debris.
Failing to mention the "well-fixed" status of the femur, or identifying the cup as loose without describing the specific patterns of bone loss (e.g., Kohler line violation, superior dome deficiency). Candidates often forget to mention the absence of infection signs.
Systematically describe the acetabular position, the status of the medial wall (Kohler’s line), and the femoral interface. Mention the "DeLee and Charnley zones." Explicitly state: "The patient has a Paprosky Type IIIA acetabular defect with severe superior and medial migration. The femoral stem is stable. Given the insidious history and radiographic appearance, the diagnosis is aseptic loosening due to macrophage-induced periprosthetic osteolysis."
How would you classify this acetabular defect using the Paprosky system, and what does this classification tell you about the surgical reconstructive strategy?

Candidate: This is a Paprosky Type IIIA defect. It indicates superior migration > 3 cm and medial migration past the Kohler line, with ischial involvement but preserved teardrop/column integrity. Reconstruction requires restoring the center of rotation, which will necessitate structural support, likely using a combination of morselized allograft for the cavitary defects and a structural augment for the segmental dome defect to ensure initial stability.
Confusing IIIA and IIIB. IIIB implies complete obliteration of the teardrop and severe ischial lysis, which is a much more complex "pelvic discontinuity" adjacent category. If you misclassify, your entire surgical plan becomes logically inconsistent.
Define the classification criteria: Type IIIA involves significant superior migration (>3cm) and medial wall deficiency, but the teardrop is not obliterated and there is no pelvic discontinuity. The surgical goal is to avoid superiorizing the center of rotation to prevent abductor deficiency. Use the words "restoration of the anatomic center of rotation," "cavitary vs. segmental management," and "mechanical stability via porous metal augments."
The femoral component is well-fixed. Describe your decision-making process regarding the femoral stem in this revision surgery.

Candidate: I would retain the femoral component. Removing a well-fixed porous-coated stem is unnecessary and highly morbid, carrying risks of fracture or requiring an extended trochanteric osteotomy. I will use the existing modular trunnion to exchange the head, selecting an offset/neck length that restores leg length and soft-tissue tension once the acetabular reconstruction is complete.
Suggesting that you "might as well change the stem" to be safe. In an 82-year-old, the biological cost of stem removal is far higher than the benefit of putting in a newer stem if the current one is stable.
Focus on the "benefit-to-risk ratio." Emphasize that stem retention minimizes blood loss, surgical time, and fracture risk. Mention checking for "trunnionosis" (corrosion) on the existing neck before placing a new modular head. This shows you are thinking about both macro-stability and the micro-environment of the modular junction.
