Tackling Paprosky Type IIIA: Acetabular Augment in Revision Hip

Key Takeaway
We review everything you need to understand about Tackling Paprosky Type IIIA: Acetabular Augment in Revision Hip. A **Paprosky Type IIIA** acetabular defect is a severe form of acetabular bone loss, often seen in revision total hip replacement. It is characterized by superolateral hip center migration greater than three centimeters and significant destruction of the superior acetabular rim. This advanced defect typically results from loosening and osteolysis, causing substantial pain and functional impairment requiring complex reconstruction.
A 68-year-old patient presents with a painful, unstable primary total hip arthroplasty performed 12 years ago. Physical examination reveals a significant Trendelenburg gait. Radiographic assessment shows a failed acetabular component with superolateral bone loss. You are presented with the following radiograph.
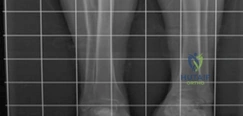
How would you classify this acetabular defect, and what are the critical anatomical landmarks that define this specific Paprosky classification?
Candidate: This is a Paprosky Type IIIA defect. It is characterized by severe superolateral bone loss with upward migration of the hip center. However, the teardrop, Kohler’s line, and the ischium remain intact, which differentiates it from a IIIB defect.
Candidates often confuse IIIA and IIIB. Failing to mention the status of the teardrop or Kohler's line suggests an incomplete understanding of the pelvic column integrity, which is essential for determining if a standard cup + augment is sufficient or if a cup-cage construct is required.
Acknowledge the Paprosky IIIA classification. Specifically note: 1) Superior migration of the hip center by 10-30mm; 2) Intact teardrop and Kohler's line (medial wall integrity); 3) Preserved ischium; and 4) >50% remaining host bone contact, which is the requisite for achieving primary mechanical stability for a hemispherical shell.
You have decided to utilize a highly porous metal augment. During preoperative planning using 3D CT, you see the following topographical map. What are the biomechanical objectives of this reconstruction regarding the hip center, and why is this critical for long-term survivorship?

Candidate: The goal is to restore the anatomic center of rotation. If the cup is placed too high and lateral, it shortens the abductor moment arm, which increases the joint reaction force and leads to a Trendelenburg gait and accelerated component wear.
Focusing only on "filling the gap" without discussing the biomechanics of the abductor lever arm. The examiner is looking for an understanding of the relationship between the hip center, muscle force, and joint reaction forces.
Articulate that restoring the anatomic hip center optimizes the moment arm of the gluteus medius/minimus. A high-lateral position (up-and-out) exponentially increases the joint reaction force (JRF). Mention that porous metal augments allow us to bridge the defect to reach the anatomic floor, thereby normalizing JRF and improving long-term survivorship through biological ingrowth.
During the procedure, you have fixed the augment to the ilium. You are now preparing to cement the shell to the augment. What is your technical strategy to ensure a successful "monolithic" construct, and what must you avoid regarding the bone-implant interface?
Candidate: I use PMMA cement to bridge the interface between the porous metal augment and the shell. I must be careful not to let cement touch the host bone, as that would prevent the porous metal from integrating with the bone.
Forgetting that the augment must first be rigidly fixed to the host bone via screws before the shell is cemented. Applying cement to the host bone interface is a "cardinal sin" in this technique.
Structure the answer: 1) Augment is secured to host bone via titanium cancellous screws in the safe zones (e.g., Wasielewski quadrants); 2) Shell is impacted; 3) PMMA is used strictly as a "grout" between the augment and shell; 4) Emphasize that no cement must interface with the bone-facing porous surfaces to ensure unhindered secondary biological fixation (osteointegration).
