Mastering Trauma Principles: Damage Control Orthopaedics and Polytrauma Management

Key Takeaway
The management of polytrauma requires a multidisciplinary approach centered on rapid physiological stabilization and strategic fracture management. This guide details the critical transition from Early Total Care (ETC) to Damage Control Orthopaedics (DCO), emphasizing the mitigation of the systemic immune response syndrome (SIRS). It provides evidence-based protocols for soft-tissue classification, compartment syndrome evaluation, and the precise application of temporary external fixation to optimize patient survival and functional recovery.
TRAUMA PRINCIPLES AND POLYTRAUMA MANAGEMENT
The treatment of patients with multiple trauma requires highly specialized resources, multidisciplinary coordination, and rapid physiological assessment—capabilities that are often unavailable in smaller community hospitals. The acute stabilization of long bone, pelvic, and spinal fractures must adhere to stringent, evidence-based trauma center protocols.
Treatment in a Level I or Level II trauma center has been unequivocally documented to improve the survival and functional outcomes of patients with multiple injuries. The centralization of trauma care has yielded dramatic epidemiological shifts. For instance, following the development of Germany's highly organized trauma system, mortality from polytrauma plummeted from 40% in 1972 to 18% in 1991. Similarly, in San Diego County, the implementation of a regionalized trauma center system decreased overall mortality from 26% to 8%. Furthermore, the frequency of suboptimal assessment decreased from 22% to 1%, suboptimal care from 32% to 4%, delay in evaluation from 41% to 10%, and delay in treatment from 63% to 7%.
Beyond mortality benefits, the length of hospital stay and the overall cost of treatment are significantly lower in patients who are triaged directly to trauma centers compared to those who require secondary transfer. Therefore, the gold standard for the management of multiply-injured patients—both in terms of clinical efficacy and health economics—is immediate referral to a dedicated trauma center.
The Advanced Trauma Life Support (ATLS) Protocol
Management of a patient who has sustained multiple injuries requires specific, reliable, and reproducible methods of evaluation. The Advanced Trauma Life Support (ATLS) system, developed by the American College of Surgeons, remains the universal standard for evaluating trauma patients. The primary survey is dictated by the ABCDE mnemonic:
- A - Airway: Must be free and unobstructed, with simultaneous cervical spine protection.
- B - Breathing: Ensure adequate ventilation and oxygenation. Rule out tension pneumothorax, massive hemothorax, and flail chest.
- C - Circulation: Assess central and peripheral perfusion. The goal is brisk capillary refill and maintenance of normotension. Hemorrhage control is paramount.
- D - Disability: Rapid neurological assessment (GCS, pupillary response) and identification of severe musculoskeletal, urological, and reproductive injuries.
- E - Environment/Exposure: Completely undress the patient to identify all injuries, followed by immediate prevention of hypothermia.
Clinical Pearl: An estimated 5% to 20% of patients with multiple trauma have injuries that are missed during the initial primary survey. Factors contributing to missed injuries include altered consciousness (TBI, intubation), profound hemodynamic instability precluding a thorough secondary survey, distracting injuries, and inadequate initial radiographs. A formal tertiary survey must be conducted once the patient is physiologically stable.
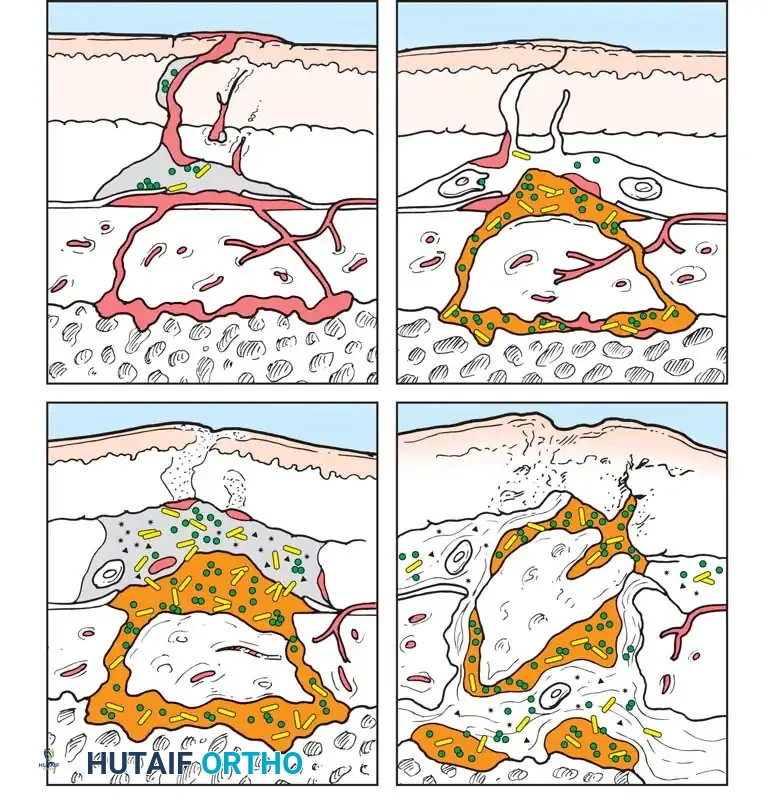
THE PATHOPHYSIOLOGY OF POLYTRAUMA: SIRS AND THE "SECOND HIT"
Polytrauma and the massive tissue disruption it causes result in the activation of cellular factors that exert profound systemic effects. This diffuse inflammatory reaction, mediated by cytokines (such as IL-6, IL-1, and TNF-α), is known as Systemic Immune Response Syndrome (SIRS).
The initial trauma serves as the "First Hit," priming the patient's immune system. Subsequent prolonged surgical interventions (such as definitive intramedullary nailing of bilateral femur fractures) act as a "Second Hit," which can hyperactivate the primed immune system, leading to a catastrophic cytokine storm, Acute Respiratory Distress Syndrome (ARDS), Multiple Organ Dysfunction Syndrome (MODS), and death.
Early Total Care (ETC) vs. Damage Control Orthopaedics (DCO)
Since the early 1990s, the prevailing philosophy was Early Total Care (ETC), which advocated for the definitive stabilization of all major fractures within the first 24 hours. Studies by Bone et al. and Johnson et al. demonstrated that early stabilization of femoral shaft fractures significantly reduced pulmonary complications (ARDS, fat emboli syndrome, pneumonia). Bone et al. found that only 2% of patients with femoral shaft fractures stabilized within 24 hours developed pulmonary complications, compared to 38% in whom stabilization was delayed beyond 48 hours.
However, as our understanding of the "Second Hit" phenomenon evolved, it became clear that ETC is detrimental to patients who are physiologically exhausted or hemodynamically unstable. This realization birthed Damage Control Orthopaedics (DCO).
DCO involves the rapid, temporary immobilization of fractures (typically via external fixation) to obtain mechanical stability, control hemorrhage, and recover limb length, while minimizing surgical time and physiological burden.
Surgical Warning: Operative treatment for definitive fixation must never be undertaken if hemodynamic stabilization is not achieved, if life-threatening coagulopathy or acidosis persists, or if the patient requires escalating vasopressor support.
Pape et al. noted a significant decrease in the frequency of ARDS in borderline and unstable patients treated with temporary external fixation of femoral fractures compared to those treated with immediate intramedullary nailing. In a prospective multicenter study, Pape et al. also demonstrated a blunted inflammatory cytokine response with external fixation compared to the massive spike seen with immediate intramedullary reaming and nailing.
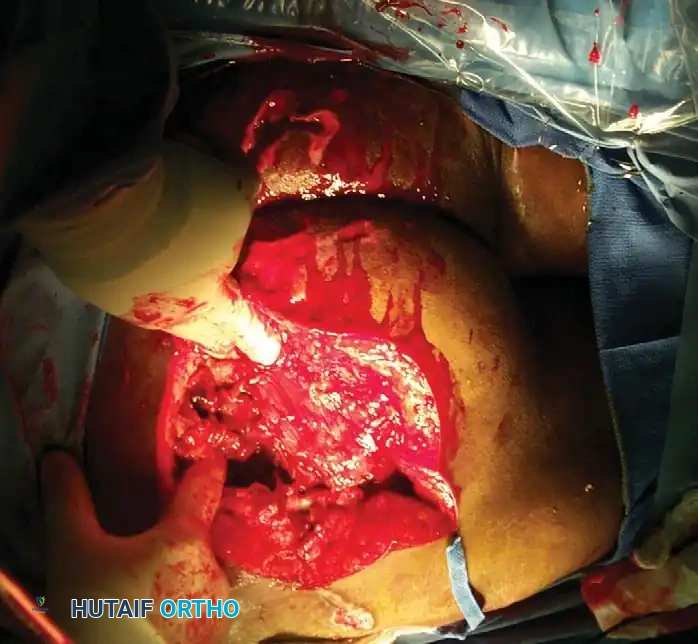
SOFT-TISSUE INJURY CLASSIFICATION
The extent of soft-tissue damage dictates the timing and type of surgical intervention. High-energy trauma imparts massive kinetic energy to the soft-tissue envelope, resulting in extensive microvascular thrombosis, necrosis, and a highly uncertain prognosis for bone healing.
AO-ASIF Soft-Tissue Injury Classification
The AO-ASIF classification provides a comprehensive framework for evaluating closed and open injuries, muscle-tendon damage, and neurovascular compromise.
Skin Lesions (Closed Fractures - IC)
* IC 1: No skin lesion.
* IC 2: No skin laceration, but contusion present.
* IC 3: Circumferential degloving.
* IC 4: Extensive, closed degloving (Morel-Lavallée lesion).
* IC 5: Necrosis from contusion.
Skin Lesions (Open Fractures - IO)
* IO 1: Skin breakage from inside out.
* IO 2: Skin breakage < 5 cm, edges contused.
* IO 3: Skin breakage > 5 cm, devitalized edges.
* IO 4: Full-thickness contusion, avulsion, soft-tissue defect.


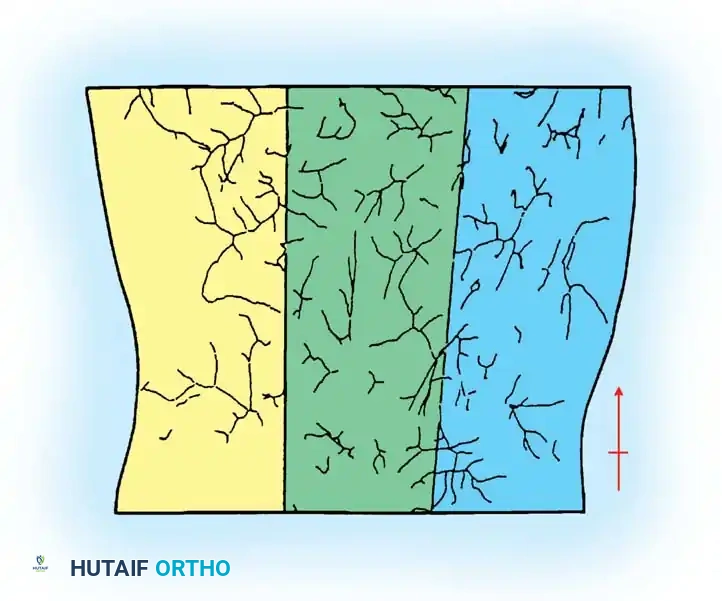
Tscherne Classification of Closed Fractures
Tscherne and Gotzen developed a highly practical grading system for soft-tissue injury in closed fractures:
- Grade 0: Little or no soft-tissue injury (indirect violence).
- Grade 1: Superficial abrasion with local contusional damage to skin or muscle.
- Grade 2: Deep contaminated abrasion with local contusional damage to skin and muscle. High risk of compartment syndrome.
- Grade 3: Extensive contusion or crushing of skin, or destruction of muscle. Often associated with severe degloving or compartment syndrome.
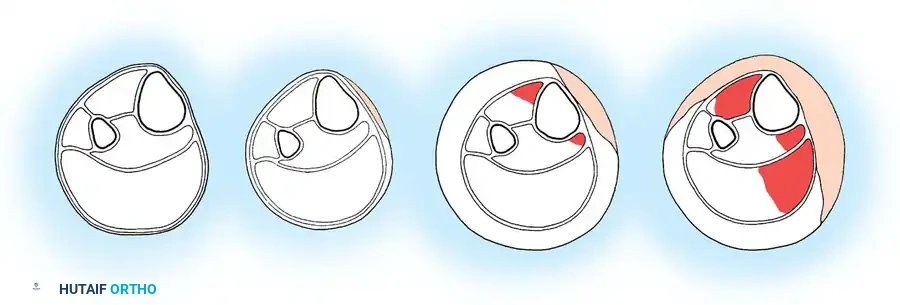
COMPARTMENT SYNDROME AND VASCULAR INJURIES
Vascular injury or compartment syndrome must be identified and treated promptly to avoid irreversible tissue ischemia. Muscle and nerve necrosis can become irreversible if ischemia persists for 6 hours or more.
The diagnosis of compartment syndrome is primarily clinical (pain out of proportion, pain with passive stretch, tense compartments). However, in the obtunded polytrauma patient, objective compartment pressure monitoring is mandatory.
Heckman et al. demonstrated that irreversible muscle damage occurs when tissue pressures rise to within 10 to 30 mm Hg of the mean arterial pressure. Today, the universally accepted threshold for fasciotomy is the Delta P (ΔP).
* ΔP = Diastolic Blood Pressure - Compartment Pressure.
* A ΔP of < 30 mm Hg is an absolute indication for immediate four-compartment fasciotomy.
Surgical Pitfall: Never rely on the presence of distal pulses to rule out compartment syndrome. Arterial flow continues long after capillary perfusion pressure has been exceeded. Pulselessness is a late, often irreversible sign of catastrophic ischemia.
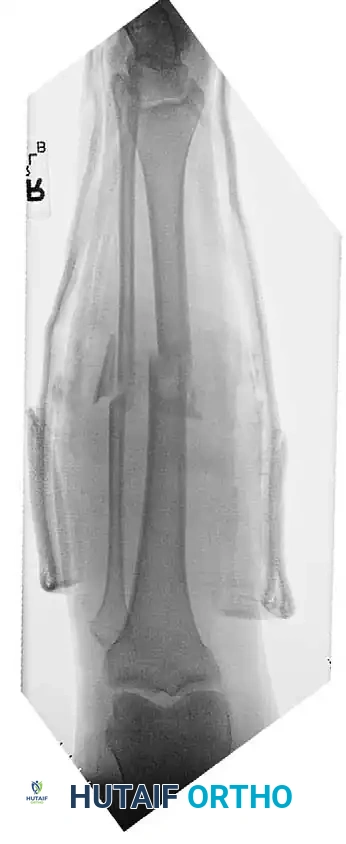
OPEN FRACTURES: PRINCIPLES AND EVOLUTION
Open fractures are surgical emergencies that should be conceptualized as incomplete amputations. The primary goals are the prevention of infection, achievement of bony union, and restoration of function.
Tscherne described four historical eras of open fracture treatment:
1. Life Preservation: The pre-antiseptic era, marked by massive mortality (Volkmann reported 38.5% mortality in 1878).
2. Limb Preservation: World War I and II, characterized by the introduction of the Thomas splint, which reduced femur fracture mortality from 80% to 15.6%.
3. Infection Avoidance: The advent of antibiotics and aggressive surgical debridement.
4. Functional Preservation: The modern era, utilizing advanced internal/external fixation, microsurgical soft-tissue coverage, and early rehabilitation.


Initial Management of Open Fractures
From the time of injury until the patient is in the operating room, the wound must be protected by a sterile dressing, and the extremity splinted to prevent further soft-tissue stripping by sharp bone ends.
- Hemorrhage Control: Direct pressure is the standard. Tourniquets are reserved for life-threatening arterial bleeding that fails direct pressure. Blind clamping of vessels in the emergency department is strictly contraindicated due to the high risk of iatrogenic nerve injury.
- Antibiotics: Intravenous antibiotics must be administered as soon as possible (ideally within 1 hour of injury). A first-generation cephalosporin is standard; aminoglycosides are added for Gustilo-Anderson Type III injuries, and high-dose penicillin for gross agricultural contamination (Clostridium coverage).

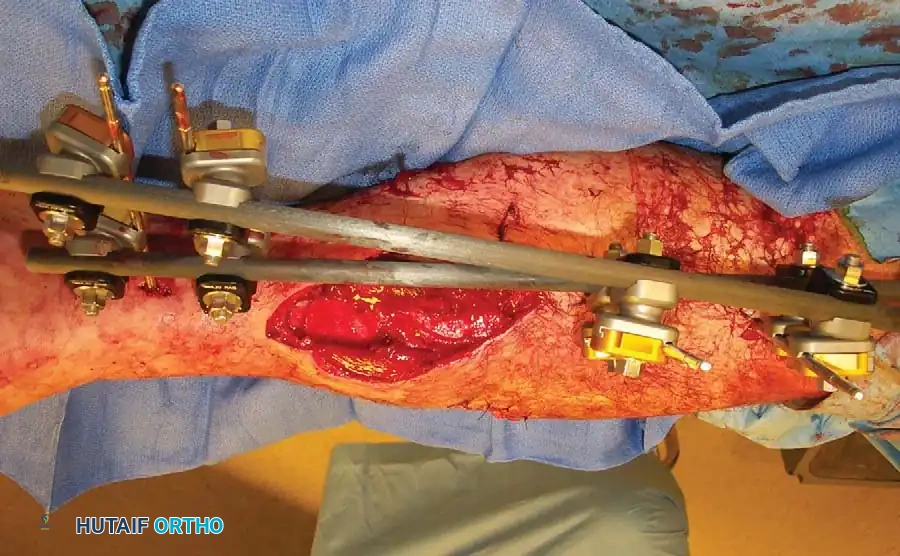
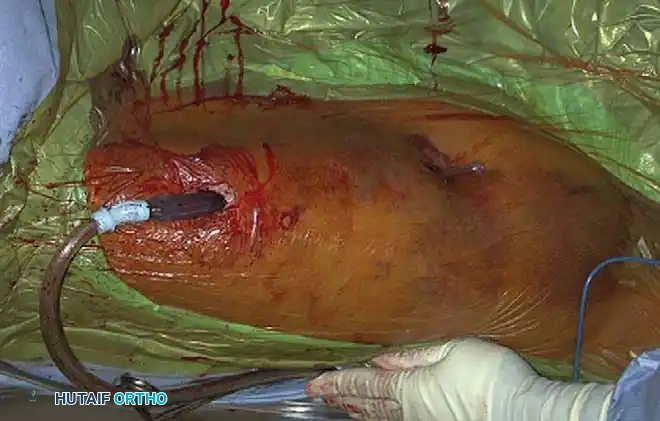
SURGICAL TECHNIQUE: DAMAGE CONTROL EXTERNAL FIXATION
When a polytrauma patient is deemed too unstable for definitive fixation (e.g., severe acidosis, hypothermia, coagulopathy), Damage Control Orthopaedics via rapid external fixation is indicated.
1. Preoperative Planning and Positioning
- The patient is positioned supine on a radiolucent trauma table.
- Ensure the entire limb is prepped and draped free to allow for traction and multi-planar fluoroscopy.
- Orthopaedic damage control measures can occasionally be undertaken in the emergency department or ICU if the patient is too unstable for transport, though the operating room is strongly preferred.
2. Pin Placement and Safe Corridors
- Femur: Half-pins (5.0 mm or 6.0 mm) are placed laterally or anterolaterally. Avoid the medial neurovascular bundle. Ensure pins are placed far enough from the fracture site to avoid contaminating the future zone of intramedullary nailing.
- Tibia: Pins are placed on the anteromedial face of the tibia (subcutaneous border).
- Technique: Make a generous stab incision. Use blunt dissection down to the bone to protect cutaneous nerves and veins. Use a drill sleeve. Pre-drill both cortices with a sharp drill bit to prevent thermal necrosis, which is the leading cause of pin-tract infection and loosening. Insert the Schanz pins bicortically.
3. Frame Construction and Reduction
- Apply bar-to-pin clamps and connect them with carbon fiber or radiolucent rods.
- Apply longitudinal traction to restore length, correct rotation, and align the mechanical axis.
- Tighten the clamps sequentially. A delta frame or multi-planar construct can be utilized if additional stiffness is required.

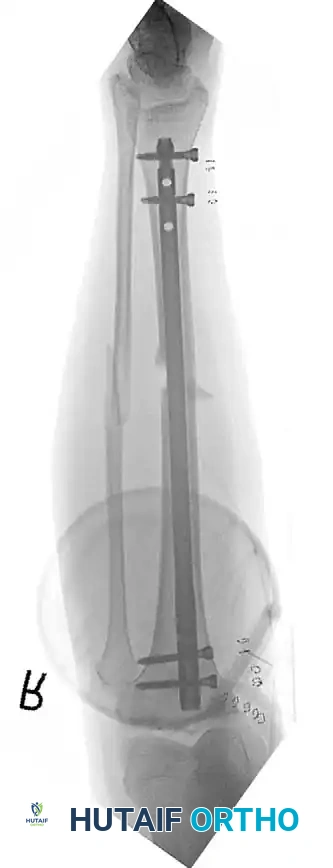
POSTOPERATIVE PROTOCOLS AND CONVERSION TO DEFINITIVE FIXATION
The goal of DCO is to bridge the patient through the acute physiological crisis. Once the patient's lactate has cleared, coagulopathy is reversed, and inflammatory markers have peaked and begun to trend downward (typically between days 5 and 10), the patient is optimized for conversion to definitive fixation.
Pin-Tract Management and Infection Risk
Lerner et al. noted complications of pin track infection with emergency external fixation; however, Harwood et al. demonstrated that there is no significant increase in deep infection rates if the conversion from external fixation to intramedullary nailing is performed in a timely manner—defined strictly as within 14 days of the initial injury.
If pin sites show signs of superficial infection (erythema, purulent discharge), the external fixator should be removed, the pin tracts aggressively debrided and over-reamed, and the patient placed in skeletal traction or a cast until the soft tissues sterilize, prior to definitive internal fixation.

Long-Term Functional Outcomes
The ultimate functional recovery of the polytrauma patient depends heavily on the initial decisions made in the trauma bay. Early stabilization of the spine, pelvis, and major articular fractures decreases the sequelae of forced recumbency (DVT, decubitus ulcers, pneumonia).

By adhering strictly to the principles of Damage Control Orthopaedics, respecting the soft-tissue envelope, and timing definitive surgical interventions to match the patient's physiological reserve, the orthopaedic surgeon plays a pivotal, life-saving role in the modern multidisciplinary trauma team.
You Might Also Like


