Tetanus Prophylaxis and Soft Tissue Management in Orthopaedic Trauma

Key Takeaway
Tetanus remains a rare but life-threatening complication of open fractures. Proper management requires strict adherence to ATLS prophylaxis protocols, distinguishing between tetanus-prone and clean wounds. This guide details the administration of tetanus toxoid and human tetanus immune globulin, alongside essential principles of soft tissue debridement, fracture fixation, and thromboembolic prophylaxis in complex orthopaedic trauma patients.
Introduction to Tetanus in Orthopaedic Trauma
The management of open fractures and severe soft tissue injuries requires a comprehensive, strategic approach that extends beyond mechanical stabilization. Among the most critical, yet frequently overlooked, medical considerations in the acute trauma setting is the prevention of tetanus. While widespread vaccination programs have relegated tetanus to a rare complication in most developed nations, the catastrophic neurological consequences of Clostridium tetani infection demand unwavering vigilance from the orthopaedic surgeon.
This masterclass delineates the evidence-based protocols for tetanus prophylaxis, the evaluation of the tetanus-prone soft tissue envelope, and the integration of these principles into the broader context of fracture management and thromboembolic prophylaxis.
Epidemiology and Pathophysiology
According to the Centers for Disease Control and Prevention (CDC), tetanus incidence in the United States is exceptionally low, with an average of 29 cases reported annually (an incidence of 0.10 per million population). However, the clinical severity remains profound. The overall mortality rate among reported cases is approximately 13%. Crucially, the mortality rate in patients aged 65 or older is nearly three times higher than in younger cohorts.
This age-related vulnerability is directly correlated with waning immunity and inadequate vaccination coverage. CDC data indicates that tetanus vaccination coverage is only 57% in individuals between the ages of 18 and 64, and drops to a concerning 44% in those 65 years of age and older.
The Pathogen: Clostridium tetani
Clostridium tetani is an obligate anaerobic, gram-positive, spore-forming bacillus ubiquitous in soil, dust, and animal feces. The spores are highly resilient, capable of surviving extreme temperatures and chemical disinfectants. When introduced into an anaerobic environment—such as devitalized, ischemic, or necrotic tissue typical of high-energy open fractures—the spores germinate into vegetative bacilli. These bacilli produce tetanospasmin, a potent neurotoxin that retrogradely travels to the central nervous system, blocking the release of inhibitory neurotransmitters (GABA and glycine) and resulting in the pathognomonic spastic paralysis and autonomic instability.
Defining the Tetanus-Prone Wound
The fundamental principle of tetanus prevention in trauma is recognizing the wound environment that facilitates spore germination. The Subcommittee on Advanced Trauma Life Support (ATLS) of the American College of Surgeons has established strict criteria for identifying tetanus-prone wounds.
A wound is considered tetanus-prone if it exhibits any of the following characteristics:
* Age of Wound: More than 6 hours elapsed since the time of injury.
* Configuration: Stellate, avulsion, or severe abrasion patterns.
* Depth: Penetration deeper than 1 cm.
* Mechanism of Injury: Missile (ballistic), crush, burn, or frostbite injuries.
* Tissue Viability: Presence of infected, devitalized, denervated, or ischemic tissue.
* Contamination: Visible contaminants including dirt, feces, soil, or saliva.
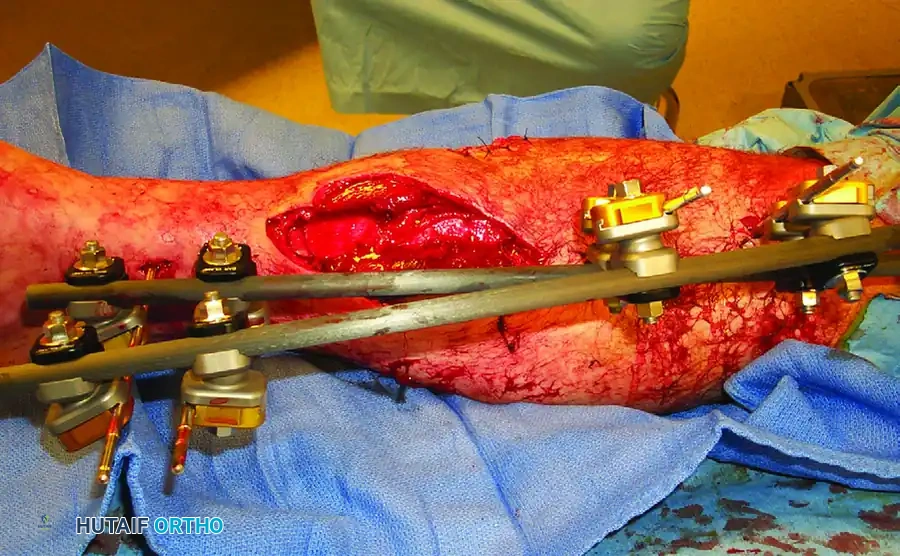
Surgical Warning: The presence of necrotic muscle or a severe crush component exponentially increases the risk of an anaerobic microenvironment. Radical surgical debridement is not merely a principle of infection control; it is the primary mechanical defense against tetanus germination.
Soft Tissue Assessment and Fracture Blisters
The condition of the soft tissue envelope dictates the timing and strategy of surgical intervention. High-energy trauma frequently results in severe dermal ischemia and venous congestion, manifesting clinically as fracture blisters.
Fracture blisters represent a cleavage at the dermo-epidermal junction. They are broadly categorized into clear fluid-filled blisters and blood-filled blisters.
* Clear Blisters: Indicate a superficial separation where the dermis remains largely intact and viable.
* Blood Blisters: Represent a deeper injury with complete disruption of the dermo-epidermal junction and significant dermal ischemia. Incising through a blood blister carries a high risk of full-thickness skin necrosis and deep infection.
FIGURE 53-48 Blood blister. The presence of blood-filled fracture blisters indicates severe underlying soft tissue trauma, necessitating a delay in definitive internal fixation until the soft tissue envelope has stabilized.
Evidence-Based Tetanus Prophylaxis Protocols
The administration of tetanus prophylaxis is dictated by two factors: the condition of the wound (clean vs. tetanus-prone) and the patient's immunization history.
1. The Actively Immunized Patient
Patients who have completed a primary tetanus toxoid active immunization series require only a booster dose of tetanus toxoid if their last dose was administered more than 5 years ago (for tetanus-prone wounds) or more than 10 years ago (for clean, minor wounds). It is now established that the protection produced by active immunization is highly durable, effectively reactivating the immune mechanism for at least 6 to 10 years.
2. The Unimmunized or Unknown Status Patient
Patients with an incomplete primary series, or those whose immunization history is unknown, require aggressive prophylaxis, particularly in the presence of a tetanus-prone wound.
* Clean Wounds: Administer the tetanus toxoid vaccine to initiate or complete the primary series.
* Tetanus-Prone Wounds: Administer Human Tetanus Immune Globulin (HTIG), 250 Units IM, in addition to initiating the tetanus toxoid active immunization series.
Pharmacologic Considerations: HTIG vs. Equine Antitoxin
Historically, equine tetanus antitoxin was utilized for severe type III open wounds. However, Human Tetanus Immune Globulin (HTIG) is now the absolute standard of care. The protective level of antibodies provided by HTIG lasts significantly longer than that of equine antitoxin, and it carries a vastly reduced risk of anaphylaxis and serum sickness. By the time the passive immunity from HTIG begins to wane, the patient's active immunization (toxoid) has typically become effective.
Clinical Pearl: The "Separate Syringe" Rule
Human tetanus immune globulin does not interfere with simultaneous active immunization with tetanus toxoid; however, to prevent in vivo neutralization, separate syringes and separate anatomical sites of injection (e.g., contralateral deltoids) must be used.
Longitudinal Immunization and The "Dormant Spore" Phenomenon
For unimmunized patients, the initial toxoid dose must be followed by a second dose 4 weeks later, and a third dose 6 to 12 months later. If surgical manipulation of the wound or fracture is necessary at 1 to 2 months post-injury, the 250 U dose of HTIG should be repeated.
Surgical Pitfall: Delayed Reconstruction
An old open fracture that has healed and remained free of drainage for many months or even years may still harbor viable, dormant spores of C. tetani encapsulated within scar tissue or sclerotic bone. Consequently, reconstructive procedures—such as nonunion takedown or autogenous bone grafting—must never be performed until the surgeon verifies the patient is actively immunized with a recent tetanus toxoid booster.
Principles of Fracture Management and Reconstruction
Fracture management in the context of severe soft tissue injury is one of the most challenging problems an orthopaedic surgeon faces. It requires an approach that is both strategic (long-term functional goals) and tactical (immediate soft tissue and bone stabilization).
As Gill profoundly stated: "Study principles rather than methods. A mind that grasps principles will devise its own methods."
Maximizing Fatigue Life of the Fixation Construct
In cases of severe open fractures, delayed unions and nonunions are frequent complications due to periosteal stripping and endosteal ischemia. The primary biomechanical goal during reconstruction is to maximize the fatigue life of the fracture fixation construct.
* Autogenous Bone Grafting: The gold standard for stimulating osteogenesis in an atrophic or oligotrophic environment. It provides osteoconductive scaffolding, osteoinductive growth factors, and osteogenic cells.
* Early Weight-Bearing: Controlled, progressive weight-bearing methods should be instituted as early as the fracture pattern and fixation construct allow. Axial loading stimulates secondary bone healing via callus formation (Wolff's Law) and prevents disuse osteopenia, thereby protecting the implant from cyclical fatigue failure.
Thromboembolic Prophylaxis in Orthopaedic Trauma
Beyond infection and nonunion, the systemic demands on the polytrauma patient introduce the critical risk of deep vein thrombosis (DVT) and pulmonary embolism (PE). The "lethal triad" of trauma (coagulopathy, hypothermia, acidosis) complicates the standard administration of chemical prophylaxis.
The Anticoagulation Dilemma
No treatment for thromboembolic complications is without significant risk. The surgeon must constantly balance:
1. Hemorrhagic Complications: Secondary to early chemical anticoagulation in a patient with multiple injuries, solid organ damage, or traumatic brain injury.
2. Embolic Risk: The catastrophic threat of a fatal PE in a hypercoagulable, immobilized trauma patient.
Prophylactic Modalities
- Mechanical Prophylaxis: Physical methods, such as graduated compression stockings and intermittent pneumatic compression (foot pumps), are the safest initial step. However, they are frequently inapplicable in patients with severe lower extremity fractures, external fixators, or massive soft tissue degloving.
- Chemical Prophylaxis: Low-molecular-weight heparins (short-chain heparins) are the pharmacological standard. Current evidence suggests that the combination of early mechanical foot pumps (when anatomically feasible) followed by short-chain heparins—initiated once the acute bleeding risk has subsided—provides the safest and most effective prophylaxis profile.
- Vena Cava Filters: For high-risk polytrauma patients who possess absolute contraindications to chemical anticoagulation (e.g., active intracranial hemorrhage, severe pelvic/acetabular fractures with ongoing retroperitoneal bleeding, or unstable spinal fractures), prophylactic inferior vena cava (IVC) filters are favored. However, the surgeon must remain cognizant of the long-term risks of IVC filters, including device migration, caval thrombosis, and chronic venous stasis. Retrievable filters should be utilized and removed as soon as the patient can safely transition to chemical prophylaxis.
Conclusion
The successful management of orthopaedic trauma demands a holistic mastery of both local tissue mechanics and systemic physiology. The prevention of tetanus through meticulous adherence to ATLS immunization protocols and radical surgical debridement is non-negotiable. By combining these infectious disease principles with biomechanically sound fracture fixation and vigilant thromboembolic prophylaxis, the orthopaedic surgeon can navigate the immense complexities of polytrauma, ultimately restoring function and preserving life.
You Might Also Like