Classification & Management of Soft Tissue Injuries in Trauma

Key Takeaway
Soft tissue injury classification is paramount in orthopedic trauma, dictating surgical timing, fixation strategies, and limb salvage potential. Systems like the Gustilo-Anderson and Tscherne classifications provide prognostic value for infection and healing. Modern polytrauma management relies on these frameworks to transition between Early Total Care (ETC) and Damage Control Orthopaedics (DCO), optimizing patient survival and functional outcomes through staged interventions.
INTRODUCTION TO SOFT TISSUE INJURIES IN ORTHOPAEDIC TRAUMA
In the realm of operative orthopaedics, the paradigm has long shifted from a purely bone-centric approach to one that equally prioritizes the soft tissue envelope. The management of orthopaedic injuries can have a profound effect on the patient’s ultimate functional recovery and may save the patient’s life and limb. Just as the bony injury must be classified to evaluate the fracture adequately and to validate results for comparative studies, trauma-associated soft tissue injuries must be rigorously evaluated.
The degree of soft tissue compromise dictates the timing of surgery, the choice between internal and external fixation, the necessity for soft tissue coverage (flaps), and the overall prognosis regarding infection, nonunion, and amputation. This comprehensive guide explores the foundational classification systems—including Gustilo-Anderson, Tscherne, and the AO/OTA frameworks—and details the modern application of Damage Control Orthopaedics (DCO) in the multiply injured patient.
FRACTURE MORPHOLOGY AND ENERGY TRANSFER
The morphology of a fracture is a direct historical record of the energy imparted to the limb. High-energy mechanisms (e.g., motor vehicle collisions, crush injuries) produce complex, comminuted fracture patterns that are invariably associated with severe periosteal stripping, muscle contusion, and vascular compromise. Conversely, low-energy mechanisms (e.g., ground-level falls) typically result in simple transverse or spiral patterns with minimal soft tissue disruption.
The Orthopaedic Trauma Association (OTA) classification of long bone fractures categorizes bony injuries based on their morphology, which serves as an initial proxy for expected soft tissue damage.
Simple Fracture Patterns
Simple fractures typically result from lower-energy torsional or bending forces. The soft tissue hinge is often preserved, allowing for standard open reduction and internal fixation (ORIF) or intramedullary nailing without extensive soft tissue morbidity.


Wedge and Butterfly Patterns
As energy increases, bending forces combined with axial loads create wedge or "butterfly" fragments. The degree of comminution correlates directly with the stripping of the periosteal blood supply.




Complex, Segmental, and Bone Loss Patterns
High-energy trauma results in segmental fractures, severe comminution, or frank bone loss. These patterns are almost universally associated with profound soft tissue devitalization, compartment syndrome risk, and the need for staged reconstructive protocols.







Clinical Pearl: Never evaluate an X-ray in isolation. A highly comminuted or segmental fracture pattern on a radiograph is a "red flag" for severe soft tissue injury, even if the skin appears intact. Anticipate significant swelling and prepare for potential compartment syndrome monitoring.
GUSTILO-ANDERSON CLASSIFICATION OF OPEN FRACTURES
Open wounds have been classified in several ways, but the most universally adopted system remains the Gustilo and Anderson classification. Originally described in 1976 based on 1,025 open fractures and modified in 1984, this system offers critical prognostic information regarding the outcome of infected fractures and guides antibiotic and surgical management.
The modified classification is based on the size of the wound, the degree of soft tissue damage, periosteal stripping, and the presence of vascular injury.
Type I Open Fractures
- Definition: Clean wound less than 1 cm long.
- Mechanism: Typically a low-energy injury where the bone pierces the skin from the inside out.
- Soft Tissue Status: Minimal muscle contusion; simple fracture pattern (transverse or short oblique).
- Management: Intravenous first-generation cephalosporin (e.g., Cefazolin) for 24 hours. Surgical debridement and irrigation, followed by definitive fixation (often intramedullary nailing for long bones).

Type II Open Fractures
- Definition: Laceration more than 1 cm long, but without extensive soft tissue damage, skin flaps, or avulsions.
- Mechanism: Moderate energy.
- Soft Tissue Status: Slight to moderate crush injury; moderate comminution of the fracture.
- Management: Extended debridement. Antibiotic coverage typically includes a first-generation cephalosporin, though some protocols add Gram-negative coverage depending on contamination.
Type III Open Fractures
Type III fractures result from high-energy trauma, regardless of the size of the wound. This group includes segmental or severely comminuted fractures, even those with seemingly innocuous 1-cm lacerations (e.g., high-velocity gunshot wounds or agricultural injuries).
Type IIIA
- Definition: Extensive soft tissue lacerations or flaps, but maintains adequate soft tissue coverage of the bone.
- Characteristics: Massive contamination may be present, but local soft tissue (muscle/skin) is sufficient to close over the fracture or implant without requiring a distant flap.


Type IIIB
- Definition: Extensive soft tissue loss with periosteal stripping and bone exposure.
- Characteristics: These injuries are usually massively contaminated. The critical defining feature is that local soft tissue is inadequate for coverage, necessitating a rotational or free tissue transfer (flap) for closure.
- Management: Serial debridements, application of Negative Pressure Wound Therapy (NPWT), and stabilization with external fixation or intramedullary nailing. Flap coverage should ideally be performed within 3 to 7 days.

Type IIIC
- Definition: Open fractures associated with an arterial injury that requires repair, regardless of the size of the soft tissue wound.
- Characteristics: This classification has profound prognostic significance, carrying the highest risk of amputation.
- Management: Requires immediate multidisciplinary intervention (Orthopaedics and Vascular Surgery). The sequence typically involves temporary shunting, rapid skeletal stabilization (external fixation), followed by definitive vascular repair and fasciotomies.

Surgical Warning: The final grading of a Gustilo-Anderson open fracture can only be accurately determined in the operating room after thorough surgical debridement. A wound that appears as a Type II in the emergency department may reveal extensive deep muscle necrosis and periosteal stripping, upgrading it to a Type IIIB.
TSCHERNE AND GOTZEN CLASSIFICATION
While the Gustilo-Anderson system addresses open fractures, the Tscherne and Gotzen classification, widely used in Europe, is invaluable because it explicitly grades the soft tissue injury in closed fractures. This system recognizes that severe soft tissue damage and compartment syndrome can occur without a break in the skin.
Closed Fractures (Grades 0-3)
- Grade 0: Little or no soft tissue injury. Typical of indirect trauma (e.g., low-energy torsion).
- Grade 1: Superficial abrasion with local contusional damage to skin or muscle. Mild to moderate fracture severity.
- Grade 2: Deep contaminated abrasion with local contusional damage to skin and muscle. High risk for impending compartment syndrome.
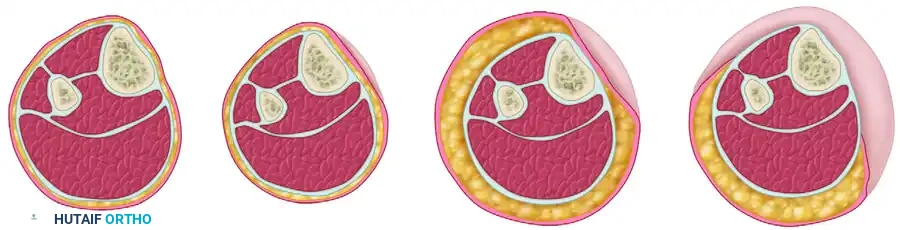
- Grade 3: Extensive contusion or crushing of skin, or destruction of muscle. Subcutaneous degloving (Morel-Lavallée lesion) and established compartment syndrome fall into this category.

Open Fractures (Grades 1-4)
The Tscherne classification for open fractures parallels the Gustilo system but places a heavier emphasis on ischemia and compartment syndrome:
* Grade 1: Skin lacerations caused by a bone fragment from inside; little or no contusion.
* Grade 2: Any type of skin laceration with circumscribed skin/soft tissue contusion and moderate contamination.
* Grade 3: Severe soft tissue damage, often with major vessel/nerve injury. All fractures accompanied by ischemia, severe comminution, or compartment syndrome belong here.
* Grade 4: Subtotal and total amputation.
COMPREHENSIVE AO-ASIF AND OTA CLASSIFICATION SYSTEMS
AO-ASIF Soft Tissue Injury Classification
To create a more granular and universally applicable system, the AO-ASIF group added an extensive soft tissue classification scheme that closely follows Tscherne and Gotzen. It evaluates four distinct domains, grading each on a scale of increasing severity:
1. Skin Lesions (Closed - IC): Ranges from IC 1 (No skin lesion) to IC 5 (Necrosis from contusion).
2. Skin Lesions (Open - IO): Ranges from IO 1 (Inside-out breakage) to IO 4 (Full-thickness contusion, avulsion, soft tissue defect).
3. Muscle-Tendon Unit Injury (MT): Ranges from MT 1 (No injury) to MT 5 (Compartment syndrome/crush injury).
4. Neurovascular Injury (NV): Ranges from NV 1 (No injury) to NV 5 (Combined neurovascular injury including subtotal/complete amputation).
The 2010 OTA Open Fracture Classification
Recognizing the limitations and inter-observer variability of the Gustilo system, the classification committee of the OTA recommended a new scheme in 2010. This system uses five categories of assessment, providing a systematic approach at the time of arrival:
* Skin injury
* Muscle injury
* Arterial injury
* Contamination
* Bone loss
While highly comprehensive, its complexity may make it less reproducible for rapid general use compared to the entrenched Gustilo-Anderson system. However, it remains an excellent tool for academic research and precise clinical documentation.
POLYTRAUMA AND TRAUMA SCORING SYSTEMS
A number of trauma scoring systems have been proposed to quantitate the degree of soft tissue injury in relation to the fracture and the potential for systemic complications. These include:
* Trauma Score (TS) and Revised Trauma Score (RTS)
* Injury Severity Score (ISS)
* Modified Abbreviated Injury Severity Scale (MISS)
* Pediatric Trauma Score (PTS)
* NISSSA (Nerve Injury, Ischemia, Soft Tissue Injury, Skeletal Injury, Shock, and Age)
* Hanover Fracture Scale-97 (HFS-97)
These systems attempt to predict functional performance, impairment, and mortality. Polytrauma and the resuscitation procedures often required in multiply injured patients result in the activation of a systemic inflammatory cascade. The timing of orth
📚 Medical References
- soft tissue injuries, J Orthop Trauma 17:683, 2003.
- Hudson DA, Knottenbelt JD, Krige JEJ: Closed degloving injuries: results following conservative surgery, Plast Reconstr Surg 89:853, 1992.
- Kudsk KA, Sheldon GF, Walton RL: Degloving injuries of the extremities and torso, J Trauma 21:835, 1981.
- Madden JE, Edlich RF, Custer JR, et al: Studies in the management of the contaminated wound. IV. Resistance to infection of surgical wounds made by knife, electrosurgery, and laser, Am J Surg 119:222, 1970.
- Morel-Lavallée: Decollements traumatiques de la peau et des couches sous-jacentes, Arch Gen Med 1:20, 1863.
- Moussa FW, Gainor BJ, Anglen JO, et al: Disinfecting agents for removing adherent bacteria from orthopaedic hardware, Clin Orthop Relat Res 329:255, 1996.
- Norris BL, Kellam JF: Soft tissue injuries associated with highenergy extremity trauma: principles of management, J Am Acad Orthop Surg 5:37, 1997.
- Orcutt S, Kilgus D, Ziner D: The treatment of low-grade open fractures without operative debridment. Read at the annual meeting of the Orthopaedic Trauma Association, October 28, 1988, Dallas, Texas. Rodeheaver GT, Petty JG, Edgerton MT, Edlich RF: Wound cleansing by high pressure irrigation, Surg Gynecol Obstet 141:357, 1975.
- Ronceray J: Drainage actif, par resection aponevrotique partielle, des epanchements de Morel-Lavallée, La Nouvelle Presse Medicale 5:1305, 1976.
- Routt MLC Jr, Simonian PT, Ballmer F: A rational approach to pelvic trauma: resuscitation and early defi nitive stabilization, Clin Orthop Relat Res 318:61, 1995.
- Tseng S, Tornetta P III: Percutaneous management of MorelLavallee lesions, J Bone Joint Surg 88A:92, 2006.
- Open Fractures Altemeier WA, Furste WL:
You Might Also Like