Comprehensive Surgical Management of Congenital Thumb Hypoplasia and Undergrowth Deformities

Key Takeaway
Congenital undergrowth deformities of the hand, particularly thumb hypoplasia, present complex reconstructive challenges. Management is dictated by the Blauth classification, which assesses the stability of the carpometacarpal joint to determine whether reconstruction or pollicization is indicated. Surgical interventions range from first web space deepening via Z-plasty to complex opponensplasties using the ring flexor digitorum superficialis or abductor digiti quinti to restore prehension and opposition.
Introduction to Congenital Undergrowth Deformities
Congenital hand anomalies classified as undergrowth deformities represent a spectrum of conditions in which embryological development is incomplete, rendering the entire upper extremity—or specific anatomical subunits—smaller or deficient. Hypoplasia of digital parts rarely occurs in isolation; it is frequently associated with other complex deformities of the hand and forearm, including radial clubhand (radial longitudinal deficiency), syndactyly, and macrodactyly.
From a taxonomic standpoint, the categorization of "undergrowth" is best reserved for deformities that present a fully formed but globally deficient part, devoid of other confounding anomalies such as failure of differentiation (e.g., complex syndactyly) or duplication.
The Hypoplastic Thumb: Pathoanatomy and Classification
The designation of a hypoplastic thumb applies to any thumb exhibiting a degree of deficiency in its fundamental anatomical components: osseous, musculotendinous, or ectodermal. The clinical presentation is highly variable. The thumb may be entirely functional but simply shorter than normal, or, in its most severe manifestation, completely absent.
Epidemiologically, the hypoplastic thumb constitutes approximately 3.6% of all congenital hand anomalies according to Flatt’s extensive series, and 1.3% in the Yokohama series. Global hypoplasia of the entire hand represented 0.8% in Flatt’s series, while total absence of the thumb accounted for 1.4%.
Clinical presentation of a severe congenital thumb hypoplasia in an infant, demonstrating a deficient first web space and absent thenar musculature.
Etiology and Syndromic Associations
Because of the wide phenotypic variety of deformities produced by thumb hypoplasia, the etiological factors are equally diverse. While many occurrences are sporadic, a significant proportion are genetically transmitted or associated with specific systemic syndromes.
Historically, hypoplastic thumbs were divided into six descriptive types based on visual appearance and deficient structures: short thumb, adducted thumb, abducted thumb, floating thumb (pouce flottant), absent thumb, and clasped thumb. However, modern orthopedic practice relies heavily on the Blauth Classification System, which dictates surgical decision-making.
The Blauth Classification System
The Blauth system categorizes the hypoplastic thumb into five distinct types based on the degree of anatomical deficiency:
* Type 1: Minor generalized hypoplasia (short thumb). All structures are present but smaller.
* Type 2: Adduction contracture with deficient intrinsic thenar muscles and an unstable metacarpophalangeal (MCP) joint (adducted or abducted thumb).
* Type 3: Deficient extrinsic muscles and skeletal hypoplasia. This is subdivided into 3A (stable carpometacarpal [CMC] joint) and 3B (unstable/absent CMC joint).
* Type 4: Deficient osseous structures, specifically an absent or rudimentary thumb metacarpal (floating thumb).
* Type 5: Total absence of the thumb.
Clinical Pearl: In the Blauth classification scheme, the presence of a stable carpometacarpal (CMC) joint is the absolute critical determinant of surgical strategy. A stable CMC joint (Types 1, 2, and 3A) indicates that the thumb should be reconstructed. An unstable or absent CMC joint (Types 3B, 4, and 5) mandates amputation of the rudimentary digit and index finger pollicization.

Radiographic evaluation is mandatory to assess the presence and stability of the first metacarpal and the carpometacarpal joint, which dictates the choice between reconstruction and pollicization.
The Short Thumb (Blauth Type 1)
A normal thumb extends approximately to the level of the proximal interphalangeal (PIP) joint of the index finger. A thumb is clinically considered "short" if its distal tip falls significantly proximal to this landmark. Hypoplasia of any or all osseous components (metacarpal, proximal phalanx, distal phalanx) produces this shortening.
Syndromic Correlations of the Short Thumb
The specific osseous segment that is shortened often provides a diagnostic clue to an underlying syndrome:
* Short and Slender Metacarpal: Fanconi anemia, Holt-Oram syndrome, or Juberg-Hayward syndrome. These require urgent workup for associated spinal, cardiovascular, and gastrointestinal malformations.
* Short and Broad Metacarpus: Cornelia de Lange syndrome, hand-foot-uterus syndrome, diastrophic dwarfism, or myositis ossificans progressiva.
* Short Proximal Phalanx: Often associated with isolated brachydactyly.
* Broad and Short Distal Phalanx: Rubinstein-Taybi, Apert, Carpenter, or hand-foot-uterus syndrome.
* Slender Distal Phalanx: Fanconi or Holt-Oram syndrome.
Morphologically, the thumb may be radially deviated ("hitchhiker’s thumb") or very short and stubby ("potter’s thumb" or "murderer’s thumb").
Treatment of the Short Thumb
If a hypoplastic thumb is only short (Blauth Type 1) and possesses normal intrinsic and extrinsic function, surgical correction is rarely indicated. However, if prehension (grasp) is significantly limited due to the shortened lever arm, deepening of the first web space is highly effective. This creates a relative lengthening of the thumb in relation to objects being grasped. This relative lengthening is typically achieved with a two-limb or four-limb Z-plasty.
The Adducted Thumb (Blauth Type 2)
An adducted thumb is primarily caused by the absence or partial absence of the thenar musculature (abductor pollicis brevis, opponens pollicis, and superficial head of the flexor pollicis brevis), resulting in severely deficient opposition.
Pathoanatomy
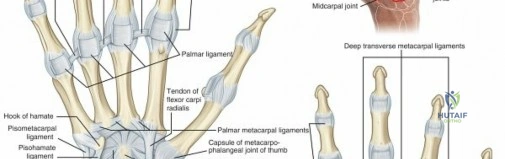
Strauch and Spinner noted that these thumbs frequently lack a functional flexor pollicis longus (FPL) muscle, or the FPL may be aberrantly connected. Furthermore, the radial collateral ligament (RCL) or ulnar collateral ligament (UCL) of the thumb MCP joint is often deficient, leading to profound instability during pinch maneuvers.
Clinically, the thumb is shortened and tapered, presenting with a flattened thenar eminence and a severely deficient, contracted first web space. This deformity is usually transmitted as an autosomal dominant trait and is predominantly unilateral.
Treatment Principles for the Adducted Thumb
The goals of surgical reconstruction are twofold:
1. Correction of the adduction contracture: Deepening the first web space.
2. Restoration of opposition: Tendon transfer (opponensplasty).
The adduction contracture may be corrected by a two-limb Z-plasty, a four-limb Z-plasty, or a sliding dorsal flap raised from the radial side of the index finger. While a simple two-limb Z-plasty is occasionally sufficient for mild cases, it rarely attains adequate correction for severe contractures.
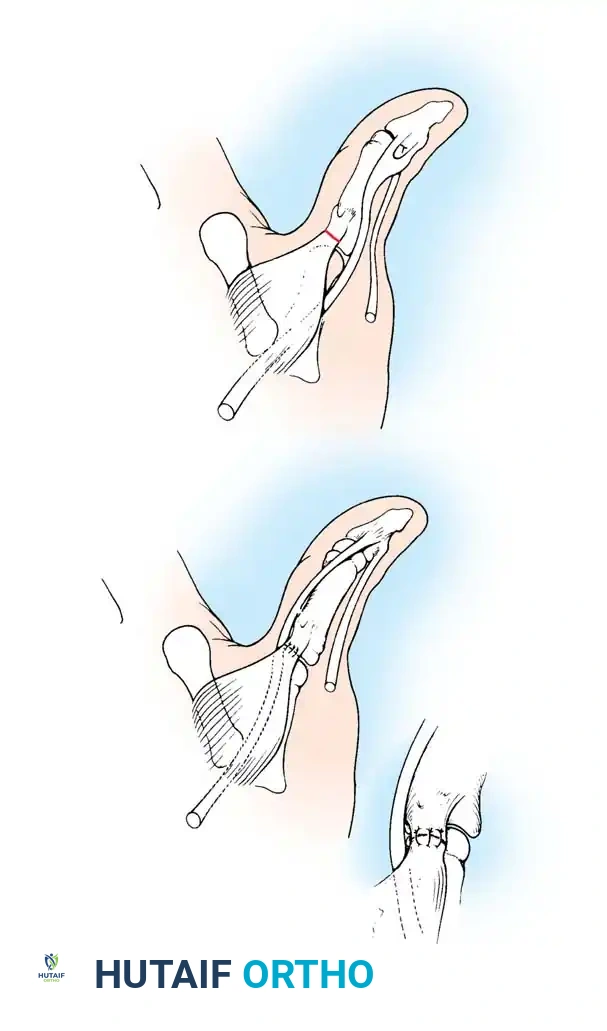
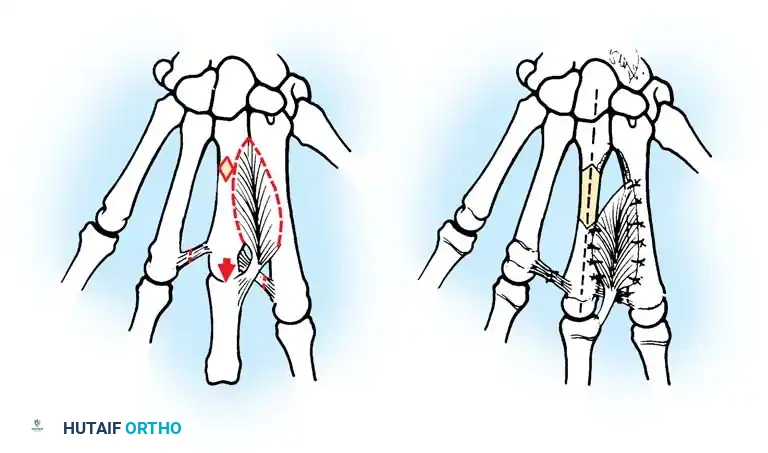
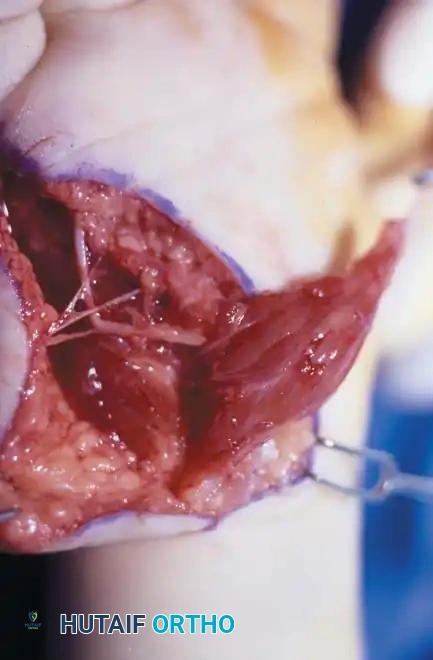
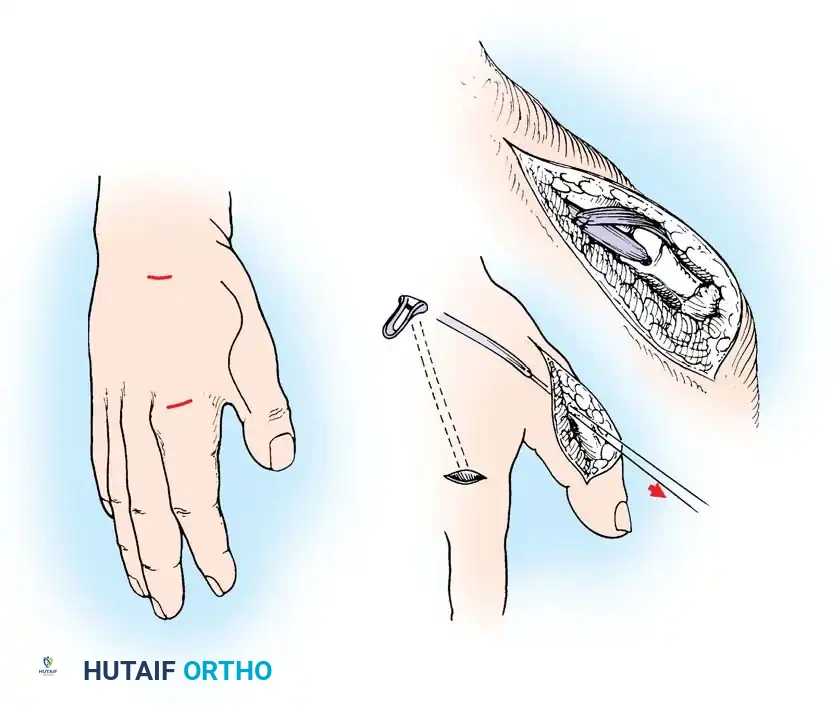
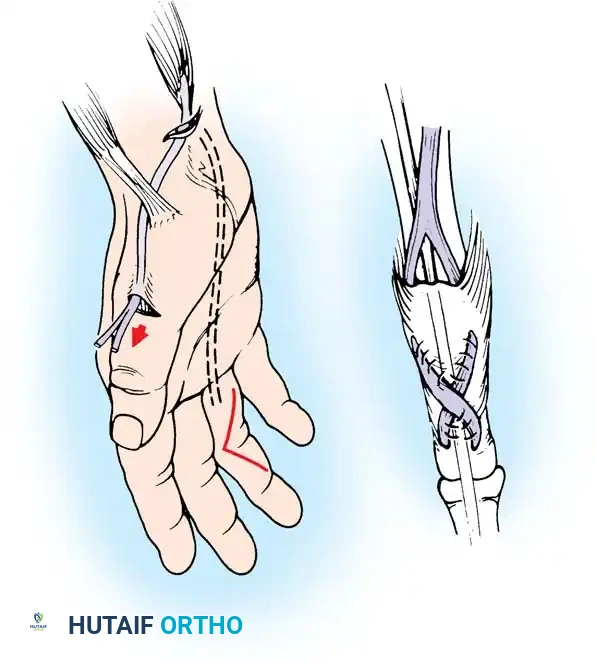
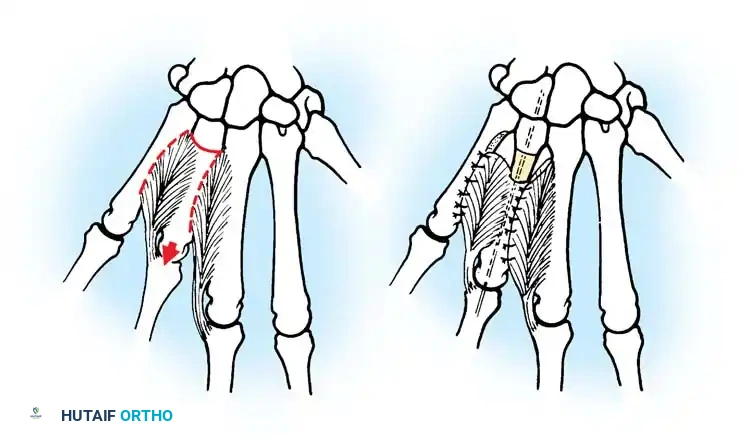
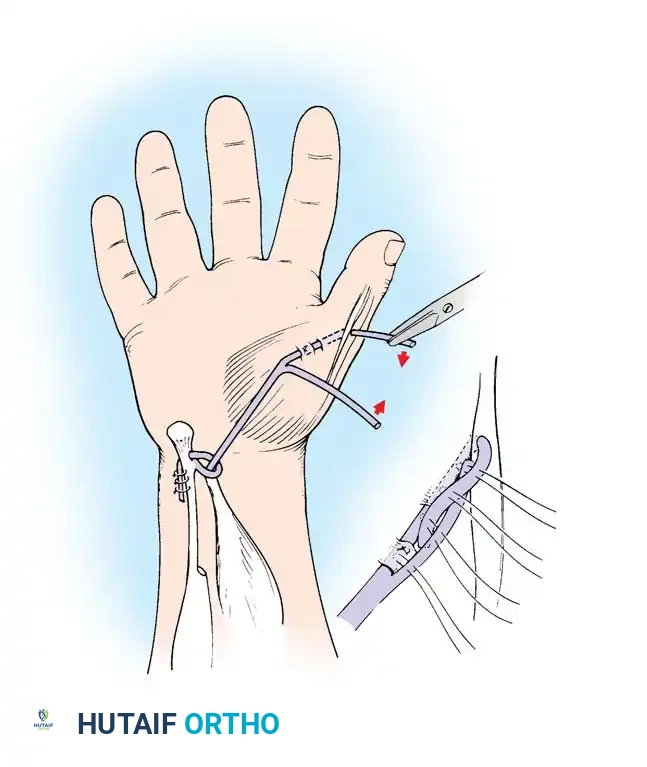
For the restoration of opposition, the two most popular techniques are the ring flexor digitorum superficialis (FDS) tendon opponensplasty (Riordan technique) and the abductor digiti quinti (ADQ) opponensplasty (Huber procedure, popularized by Littler and Cooley). The Huber procedure has the distinct advantage of creating a more normal-appearing thenar eminence by transferring a muscle belly into the deficient thenar space.
Littler and Cooley described the use of an abdominal flap for soft-tissue coverage in severe adduction contractures of the thumb, though modern practice often favors local or regional fasciocutaneous flaps.
Upton et al. have also reported excellent results utilizing pedicled, distally based radial and dorsal interosseous forearm fasciocutaneous island flaps in young children with severe congenital malformations requiring massive web space reconstruction.
Surgical Techniques: First Web Space Deepening
Simple Z-Plasty of the Thumb Web (Technique 76-35)
Surgical Warning: The fundamental principle of all Z-plasty procedures must be strictly adhered to: all flap sides must be of exactly equal lengths to prevent tip necrosis and ensure tension-free transposition.
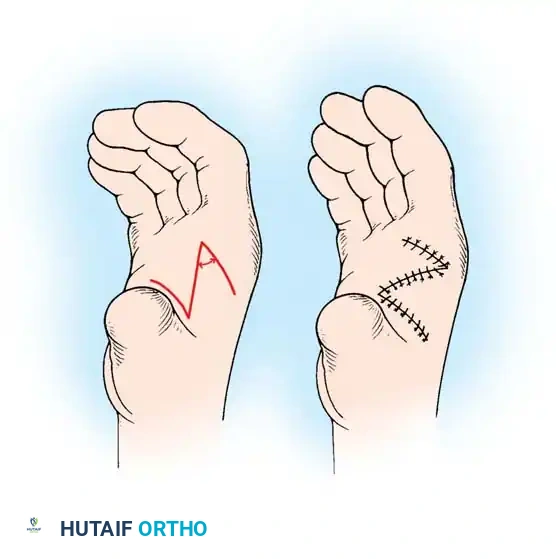
Fig. 76-59: Simple Z-plasty of the thumb web. (A) Incision design along the distal ridge. (B) Closure after reversal and interdigitation of the flaps.
Step-by-Step Procedure:
1. Marking: Before inflating the tourniquet, diagram the skin incision. Design the flap with its longitudinal axis along the distal ridge of the first web space, extending from the proximal thumb crease to approximately 1 cm proximal to the proximal digital crease of the index finger (corresponding to the radial confluence of the proximal and middle palmar creases).
2. Flap Design: Draw an oblique proximal palmar limb and a distal dorsal limb at approximately 60-degree angles to the central axis. Ensure the lengths of both limbs correspond exactly to the longitudinal incision.
3. Incision and Elevation: Inflate the tourniquet. Make the incisions as outlined. Elevate the flaps sharply, undermining carefully just superficial to the fascia to avoid vascular compromise to the subdermal plexus.
4. Deep Dissection: If additional depth is required, sharply dissect the distal edge of the web space musculature (adductor pollicis fascia) to obtain a partial recession.
5. Transposition: Reverse the flaps and carefully interdigitate them.
6. Closure: Suture the flaps with interrupted 6-0 nylon or absorbable skin sutures. Use vertical mattress sutures at the tips to help prevent tip necrosis.
7. Postoperative Care: Deflate the tourniquet, confirm adequate capillary refill in the flaps, and apply a sterile bulky dressing with the thumb splinted in an abducted, opposed position. Remove sutures and splint at 2 weeks.
Alternative simple Z-plasty variant demonstrating the geometric transposition required to lengthen the contracted web space.
Four-Flap Z-Plasty (Broadbent and Woolf, Modified) (Technique 76-36)
The four-flap Z-plasty provides superior deepening and lengthening of the web space compared to the simple Z-plasty and is preferred for moderate to severe contractures.
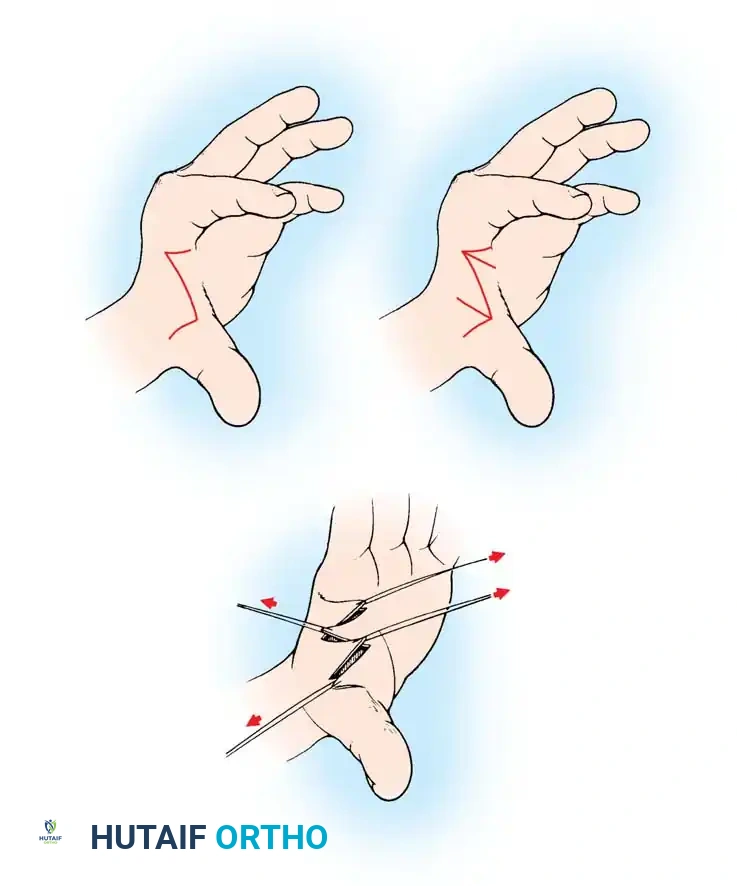
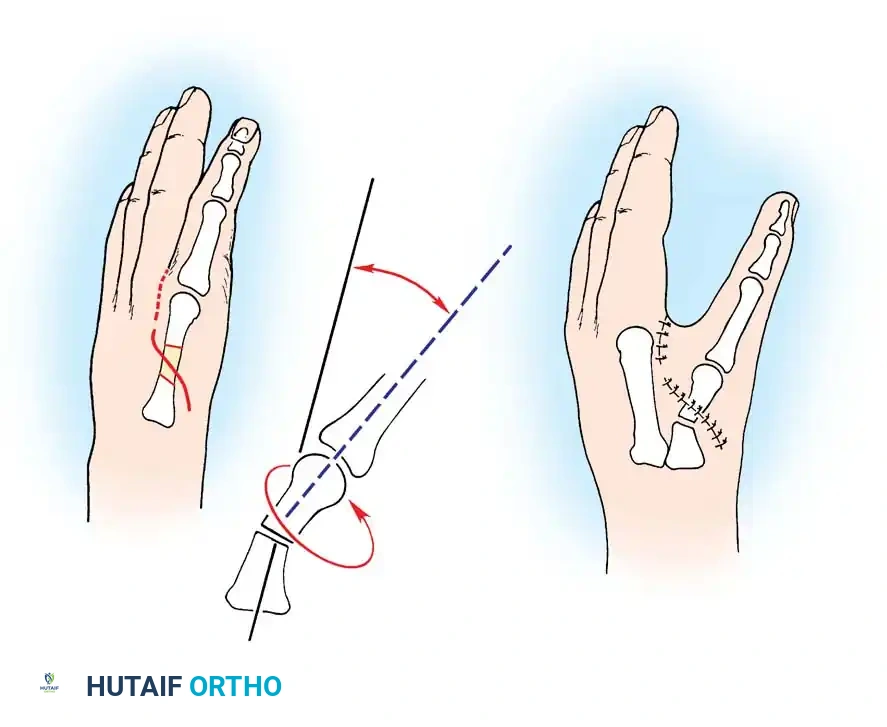
Fig. 76-60: Four-flap Z-plasty for lengthening the first web in an adducted thumb. (A) 90-degree dorsal and volar flaps are marked. (B) Flaps are bisected to create four distinct flaps. (C) Flaps are elevated, transposed, and interdigitated (sequence 3, 1, 4, 2).
Step-by-Step Procedure:
1. Marking the Axis: Make the longitudinal axis of the Z-plasty along the distal edge of the thumb web ridge, extending from the ulnar margin of the proximal thumb crease to 1 cm proximal to the proximal digital crease of the index finger.
2. Creating the Flaps: Draw proximal palmar and distal dorsal limbs at 90-degree angles to the longitudinal axis. The lengths of these limbs must equal the longitudinal incision.
3. Bisection: Bisect each 90-degree angle with an additional oblique limb, ensuring the length corresponds to the other flap margins. This creates four distinct flaps.
4. Elevation: Inflate the tourniquet. Sharply elevate the flaps, taking skin and a small amount of subcutaneous tissue.
5. Muscle Recession: For further deepening, perform a small recession of the thumb web musculature (adductor pollicis) in its midsubstance. Do not perform a complete myotomy, as this will severely weaken pinch strength.
6. Transposition: Label the flaps 1, 2, 3, and 4 (from radial to ulnar). Interdigitate them so the final sequence is 3, 1, 4, 2. Suture with 6-0 monofilament nylon.
7. Postoperative Care: Splint in abduction for 2 weeks. A web-spacer orthosis may be used for an additional 2 to 4 weeks to prevent recurrent contracture.
Complex flap transposition requires meticulous handling of the skin edges to prevent vascular compromise at the apices.
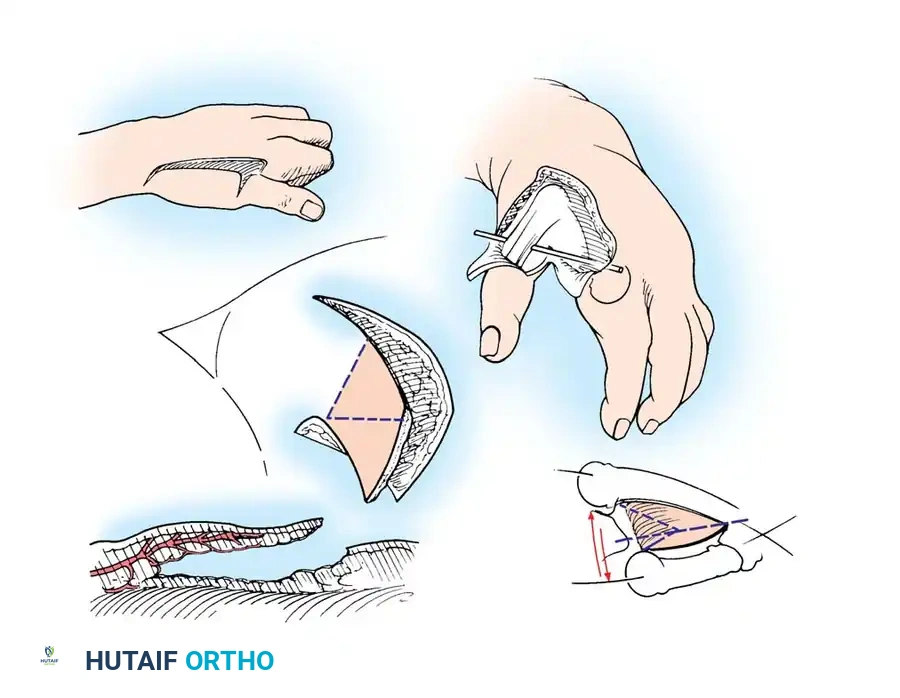
Web Deepening with a Sliding Flap (Brand et al.) (Technique 76-37)
For severe adduction contractures where local tissue rearrangement is insufficient, a dorsal sliding flap provides excellent coverage of the deepened web.
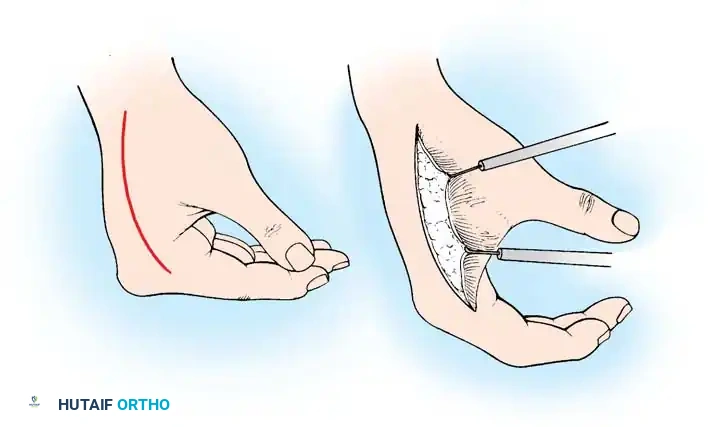
Fig. 76-61: Dorsal sliding flap for correction of adduction deformity. (A) Incision design. (B) The radial flap is undermined and advanced into the web space; the resulting dorsal defect is covered with a split-thickness skin graft.
Step-by-Step Procedure:
1. Flap Design: Draw a line dorsally from the apex of the first and second metacarpals, extending distally to the radial side of the proximal phalanx of the index finger. Curve the line back across the web space into the palm, proximally to the apex of the first and second metacarpals.
2. Elevation: Exsanguinate the arm and inflate the tourniquet. Sharply elevate the skin flaps with a small amount of subcutaneous tissue.
3. Fascial Release: Release any thickened dorsal and volar fascia. Exercise extreme caution to avoid injury to the radial artery and digital nerves.
4. Capsulotomy: If severe osseous contracture is present, incise the capsule of the carpometacarpal joint of the thumb.
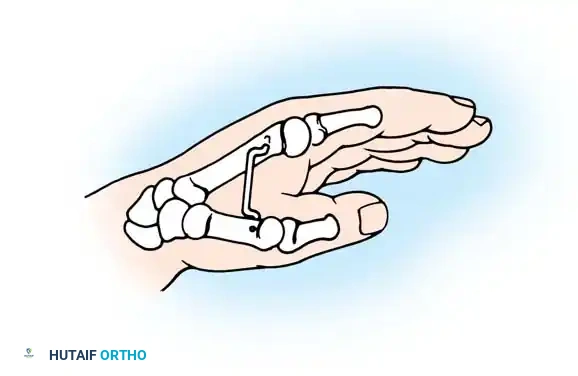
5. Fixation: Pull the thumb away from the palm into maximal abduction and hold it with a transfixing Kirschner wire (K-wire) between the first and second metacarpals.
6. Flap Advancement: Allow the dorsal flap to slide radially with the thumb, utilizing it to cover the thumb and the newly created palmar web space.
7. Grafting: The advancement of the flap will leave a secondary defect on the dorsum of the hand. Cover this dorsal defect with a split-thickness skin graft.
8. Closure: Suture the flaps with interrupted 6-0 nylon. Secure and bolster the skin graft with a tie-over dressing.
9. Postoperative Care: Remove sutures at 2 weeks. The K-wire is removed at 4 weeks, followed by unrestricted active motion.
Diagrammatic representation of web space deepening, illustrating the vector of release required to restore the functional span of the first web.
Intraoperative marking and design of a local transposition flap for web space reconstruction.
*Mobilization of the flap, demonstrating the critical need to
Associated Surgical & Radiographic Imaging


📚 Medical References
- thumb hypoplasia, J Bone Joint Surg 86A:2196, 2004.
- James MA, McCarroll R, Manske PR: The spectrum of radial longitudinal defi ciency: a modifi ed classifi cation, J Hand Surg 24A:1145, 1999.
- Kato K: Congenital absence of the radius, with review of the literature and report of three cases, J Bone Joint Surg 6:589, 1924.
- Kawabata H, Masatomi T, Yasui N: Residual deformity in congenital radial club hands after previous centralization of the wrist: ulnar lengthening and correction by the Ilizarov method, J Bone Joint Surg 18A:316, 1998.
- Kessler I: Centralization of the radial club hand by gradual distraction, J Hand Surg 14B:37, 1989.
- Kummel W: Die Missbildungen der Extremitäten durch Defekt, Verwachsung und Ueberzahl, heft 3, Kassel, Germany, 1895, Bibliotheca Medica. Lamb DW: The treatment of radial club hand: absent radius, aplasia of the radius, hypoplasia of the radius, radial paraxial hemimelia, Hand 4:22, 1972.
- Lamb DW: Radial club hand, a continuing study of sixty-eight patients with one hundred and seventeen club hands, J Bone Joint Surg 59A:1, 1977.
- Lamb DW, Wynne-Davies R, Soto L: An estimate of the population frequency of congenital malformations of the upper limb, J Hand Surg 7A:557, 1982.
- Lidge RT: Congenital radial defi cient club hand, J Bone Joint Surg 51A:1041, 1969.
- Manske PR, McCarroll HR Jr: Abductor digiti minimi
You Might Also Like