Mastering Pediatric Hand Anomalies: Surgical Management of Congenital Trigger Digits and Camptodactyly
Key Takeaway
Congenital trigger digits and camptodactyly present unique challenges in pediatric hand surgery. Successful management requires a deep understanding of flexor tendon biomechanics and precise surgical execution. This guide details the step-by-step operative techniques for A1 pulley release in trigger digits and comprehensive soft tissue reconstruction for camptodactyly, including flexor digitorum superficialis transfer, ensuring optimal functional outcomes for pediatric patients.
Introduction to Pediatric Flexor Tendon Anomalies
The surgical management of pediatric hand deformities requires a profound understanding of evolving biomechanics, meticulous soft-tissue handling, and an appreciation for the longitudinal growth of the child. Among the most frequently encountered conditions in the pediatric hand clinic are congenital trigger digits (thumb and fingers) and camptodactyly. While trigger digits represent a localized mismatch in the flexor tendon sheath volume, camptodactyly represents a complex, multifactorial sagittal plane deformity of the proximal interphalangeal (PIP) joint. This comprehensive guide details the evidence-based surgical techniques, pathoanatomy, and postoperative protocols required to achieve optimal outcomes in these challenging conditions.
Release of a Congenital Trigger Thumb
Congenital trigger thumb is characterized by a fixed flexion deformity at the interphalangeal (IP) joint, secondary to a size mismatch between the flexor pollicis longus (FPL) tendon (often presenting with a palpable "Notta's nodule") and the first annular (A1) pulley. Unlike adult trigger digits, conservative management (splinting, corticosteroid injections) has a significantly lower success rate in the pediatric population, making surgical release the gold standard for persistent deformities.
Preoperative Planning and Positioning
- Anesthesia: General anesthesia is preferred in the pediatric population to ensure absolute immobility.
- Positioning: The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table.
- Tourniquet: A well-padded pediatric pneumatic tourniquet is applied to the upper arm to ensure a bloodless surgical field. Exsanguination is achieved via elevation or an Esmarch bandage prior to inflation.
Surgical Technique: A1 Pulley Release
🔪 Surgical Pearl: Incision Placement
Avoid longitudinal incisions across the flexion crease, as these are prone to hypertrophic scarring and secondary flexion contractures. Always utilize a transverse incision within the natural skin creases.
- Incision: Under tourniquet control, make a precise transverse incision measuring approximately 1.0 to 1.5 cm at the volar crease of the metacarpophalangeal (MCP) joint of the thumb.
- Superficial Dissection: Utilize blunt dissection with tenotomy scissors to spread the subcutaneous fat. The flexor sheath is usually quite prominent just beneath this adipose layer.
- Nerve Protection: Carefully identify and protect the two digital nerves.
🚨 Surgical Warning: The Radial Digital Nerve
The radial digital nerve of the thumb is at exceptional risk during this approach. It crosses obliquely over the flexor sheath from ulnar to radial just proximal to the MCP flexion crease. It must be visualized and gently retracted before any incision is made into the sheath.

- Pulley Identification and Release: Identify the proximal edge of the first annular (A1) pulley. Using a #15 blade or fine tenotomy scissors, completely incise the A1 pulley longitudinally under direct vision. Ensure the release extends distally enough to allow full excursion of the Notta nodule.
- Tendon Assessment: Passively flex and extend the IP joint of the thumb. The FPL tendon should glide smoothly without catching or triggering.
- Note: Shaving the tendinous nodule or excising a segment of the A1 pulley is strictly unnecessary and risks iatrogenic tendon rupture or severe adhesions.
- Closure: Deflate the tourniquet and achieve meticulous hemostasis. Close the skin with interrupted 5-0 or 6-0 absorbable sutures (e.g., fast-absorbing gut or chromic).
- Dressing: Apply a bulky, soft pediatric hand dressing. No rigid immobilization or splinting is required.
This procedure can be performed in a similar fashion for other involved digits, though pediatric trigger fingers often present with more complex pathoanatomy.
Release of a Pediatric Trigger Finger
Triggering of the fingers in children is less common than in the thumb and often involves anatomical variations beyond a simple A1 pulley stenosis. The underlying pathology frequently involves abnormalities of the flexor digitorum superficialis (FDS) tendon, including proximal decussation, thickened slips, or abnormal insertions into the flexor digitorum profundus (FDP).
Surgical Technique: Comprehensive Flexor Sheath Exploration
- Incision: Make a volar zigzag (Bruner) incision centered over the A1 pulley. This extensile approach allows for both proximal and distal exposure of the flexor tendon sheath and its contents, which is critical if FDS abnormalities are discovered.
- Neurovascular Protection: Identify and meticulously retract the radial and ulnar digital neurovascular bundles.
- A1 Pulley Release: Incise the A1 pulley completely along its longitudinal axis.
- Dynamic Assessment: Passively flex and extend the digit. Inspect the motion of the flexor tendons. Assess the finger for any residual triggering.
- Tendon Inspection: Inspect the flexor tendons for nodules. If there is no triggering and normal gliding of the FDS and FDP is present, routine closure is carried out.
- Managing Persistent Triggering: If further triggering or abnormal motion is observed after A1 release:
- Inspect the FDS tendon for a more proximal-than-normal decussation (chiasm of Camper) or an abnormal insertion into the FDP tendon.
- FDS Slip Excision: Excise one slip of the FDS tendon if it is the source of the mechanical impingement.
- A3 Pulley Assessment: Inspect the A3 pulley area. Release the A3 pulley if there is triggering at this level.
- Final Verification: Place the finger through a full passive range of motion. Apply proximal traction to both flexor tendons together and individually, and passively extend the finger to verify that all triggering has resolved.
- Closure: Close the skin with absorbable sutures and apply a soft hand dressing.
Camptodactyly: Comprehensive Management
Camptodactyly is a non-traumatic, progressive flexion deformity of the proximal interphalangeal (PIP) joint. It most frequently involves only the little finger but can affect multiple digits.
💡 Clinical Pearl: Camptodactyly vs. Clinodactyly
Camptodactyly must be strictly distinguished from clinodactyly. Camptodactyly is a sagittal plane deformity (bent into flexion), whereas clinodactyly is a coronal plane deformity (bent radialward or ulnarward, typically due to a delta phalanx).
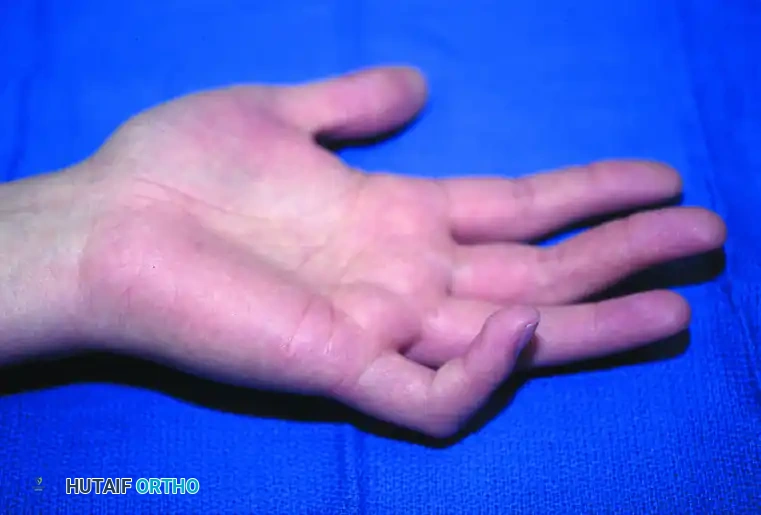
Figure: Camptodactyly demonstrating the classic isolated flexion deformity of the proximal interphalangeal joint involving the little finger.
Epidemiology and Etiology
Camptodactyly occurs in less than 1% of the general population but represents a significant portion of congenital hand anomalies (found in 6.9% of anomalies in Flatt’s series). There is a strong hereditary predisposition in many patients, transmitted as an autosomal dominant trait with variable penetrance, though sporadic cases are common.
The etiology is multifactorial, generally representing a relative imbalance between the flexor and extensor mechanisms. Implicated anatomical structures include:
* A stout, aberrant band of tissue associated with the Landsmeer (retinacular) ligament.
* Abnormal insertion of the lumbrical tendon into the FDS tendon, the MCP joint capsule, or the extensor expansion.
* Relative shortening of the FDS muscle-tendon unit.
* Contractures of the collateral ligaments or volar plate.
* Insufficient palmar skin (often a secondary contracture).
* Congenital fibrous substrata in the subcutaneous tissues.
Classification and Syndromic Associations
Camptodactyly is broadly categorized into two primary types based on the age of onset:
1. Type I (Infantile): Occurs in infancy, affects both sexes equally, and is the most common type (approximately 80% of patients).
2. Type II (Adolescent): Presents during the adolescent growth spurt and predominantly affects females.
Syndromic Associations: Camptodactyly is frequently associated with systemic syndromes, including Trisomy 13, Oculodentodigital syndrome, Orofaciodigital syndrome, Aarskog syndrome, and Cerebrohepatorenal syndromes.
Severe Congenital Subgroup: A distinct subgroup exists where severe PIP flexion deformities are present at birth, often affecting several digits of the same hand without a predilection for the small finger. Pathological findings in this subtype primarily involve the extensor mechanism, including attenuation of the central slip, palmar subluxation of the lateral bands, and hypoplasia of the radial extensor structure.
Clinical Evaluation
Most patients present with a PIP joint flexion deformity during the first year of life. Approximately two-thirds have bilateral deformities, though they are rarely symmetrical in severity. The MCP joint is usually held in compensatory hyperextension. Rotational deformities can cause mild overlapping of the fingers.
The Wrist Flexion Test:
In young children, the PIP deformity often disappears or significantly improves when the wrist is passively flexed. This indicates that a relatively short FDS muscle-tendon unit is the primary deforming force. In older children, secondary contractures of the volar plate and collateral ligaments develop, rendering the deformity fixed regardless of wrist position.

Figure A: Camptodactyly with a severe flexion deformity of 80 degrees while the wrist is held in extension.

Figure B: With the wrist in flexion, the deformity improves to 40 degrees, indicating a tight flexor digitorum superficialis unit.
Natural History and Nonoperative Treatment
If left untreated, 80% of cases worsen, particularly during periods of rapid growth acceleration. The deformity typically stabilizes after skeletal maturity (age 18 to 20 years). Pain and swelling are exceedingly rare and should prompt investigation for alternative diagnoses (e.g., inflammatory arthropathy).
Neither nonoperative nor operative treatments have been universally predictable. Historically, only 20% of patients improve with nonoperative treatment, and 35% with operative treatment.
Baek's Passive Stretching Protocol:
Baek reported promising results using a rigorous passive stretching protocol in children younger than 3 years. The protocol is time-intensive: 5-minute stretches performed 20 times daily (1 hour and 40 minutes total per day). Results demonstrated significant improvement:
* Mild camptodactyly: Improved from 20° to 1°.
* Moderate camptodactyly: Improved from 39° to 12°.
* Severe camptodactyly: Improved from 75° to 28°.
Dynamic splinting can yield good initial results, but rebound flexion deformity frequently occurs when splinting is discontinued. For patients with mild, non-progressive deformities, observation and acceptance of the deformity is a reasonable clinical recommendation.
Operative Management of Camptodactyly
Surgical intervention is indicated for progressive deformities, severe contractures interfering with hand function, or when parents desire correction in a young child whose deformity remains flexible.
Surgical Strategy Based on Age and Flexibility:
1. Young Children (< 4 years): If the deformity disappears with wrist flexion, isolated release (tenotomy) of the FDS tendon may correct the deformity and prevent worsening during growth.
2. Older Children and Young Adults: If the deformity can be passively corrected with splinting but the patient exhibits weak active extension at the PIP joint, release of the FDS and transfer into the extensor apparatus is advised to augment extension power.
3. Fixed Deformities: A comprehensive volar release is required. This includes local skin flaps (Z-plasties), volar plate release, and accessory collateral ligament release, performed prior to any tendon transfer to allow passive correction.
Smith's Unifying Approach:
Smith emphasized the necessity of exploring and treating all abnormal structures contributing to the deformity. Table 79-6 outlines the relative frequency of involved structures encountered during surgical exploration.
Table 79-6: Structures Involved in Patients with Camptodactyly
| Structure Involved | % of Cases |
|---|---|
| Skin | 100% |
| Flexor digitorum superficialis and tendon sheaths | 66.6% |
| Retinaculum cutis | 55.5% |
| Lumbricals | 22.0% |
| Bone (abnormal PIP joint surfaces/neck of proximal phalanx) | 16.6% |
| Volar plate | 16.6% |
| Central slip | 11.0% |
| Adherence of lateral bands to proximal phalanx | 11.0% |
| Accessory collateral ligaments | 5.6% |
Data derived from Smith PJ, Grobbelaar AO: Camptodactyly: a unifying theory and approach to surgical treatment, J Hand Surg 23A:14, 1998. Using this comprehensive approach, the postoperative arc of motion averaged 85 degrees.
Surgical Technique: FDS Release and Transfer

Figure C: Following superficialis tenotomy, the flexion deformity measures 40 degrees and is now completely unrelated to wrist position, confirming the release of the dynamic deforming force.
When augmenting the extensor mechanism is necessary, the FDS tendon is transferred to the extensor apparatus.
- Exposure: Utilize a volar zigzag incision over the affected digit to expose the flexor sheath, and a dorsal longitudinal or curved incision over the proximal phalanx to expose the extensor mechanism.
- FDS Harvest: Identify the FDS tendon. Divide it at its insertion points on the middle phalanx.
- Tendon Routing: Withdraw the FDS tendon proximally into the palm. Reroute the tendon dorsally through the lumbrical canal to reach the extensor apparatus.
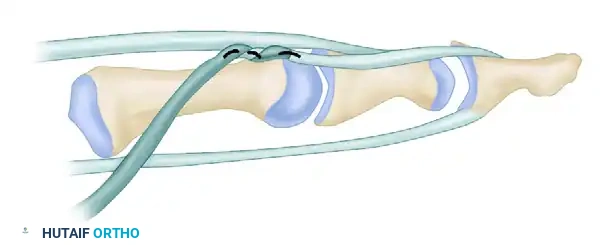
Figure: Technique for correction of camptodactyly. The flexor sublimis (superficialis) tendon is prepared for transfer to the extensor apparatus.
- Tendon Insertion: Weave the transferred FDS tendon into the lateral band of the extensor mechanism. Tension the transfer with the PIP joint held in full extension and the wrist in neutral.
- Fixation: Secure the transfer using non-absorbable horizontal mattress sutures (e.g., 4-0 braided polyester).
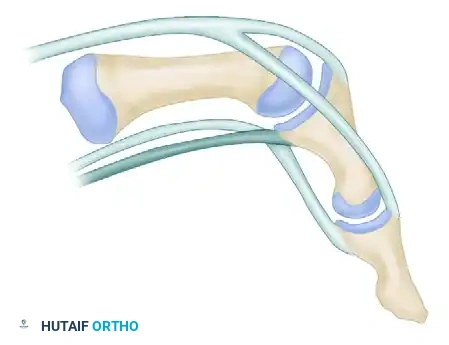
Figure: The flexor sublimis tendon has been routed through the lumbrical canal and securely sutured to the extensor lateral band, augmenting PIP joint extension.
🚨 Surgical Warning: Postoperative Impingement
Postoperative impingement has been noted primarily in patients whose extensor mechanism was realigned and augmented by release or transfer of the FDS. Meticulous tensioning and ensuring smooth gliding through the lumbrical canal are critical to prevent this complication.
Postoperative Rehabilitation
Following comprehensive release and tendon transfer, the digit is immobilized in a static extension splint for 3 to 4 weeks to protect the tendon transfer and soft tissue healing. Following this period, a rigorous, therapist-guided rehabilitation program is initiated.
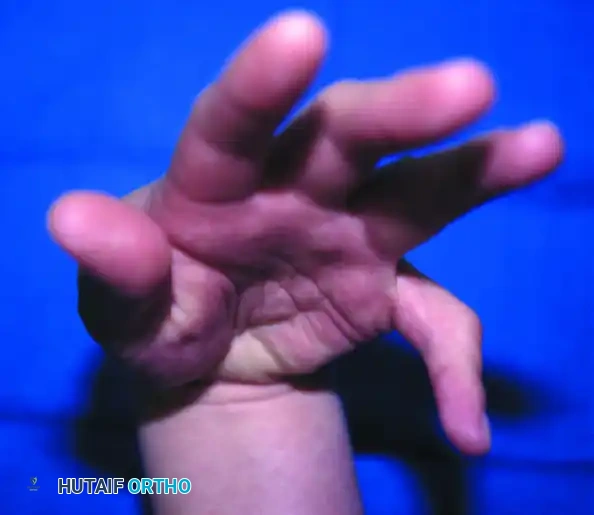
Figure D and E: Following meticulous postoperative rehabilitation, the patient demonstrates an excellent active proximal interphalangeal joint arc of motion from 20 degrees of extension to 90 degrees of flexion.
Night splinting in extension is often continued for 3 to 6 months postoperatively to prevent recurrence of the flexion contracture during the remodeling phase of healing. Regular follow-up through skeletal maturity is advised to monitor for recurrent deformity during growth spurts.
You Might Also Like

