Partial Nail Fold and Nail Matrix Removal: Advanced Surgical Techniques

Key Takeaway
Partial nail fold and nail matrix removal aims to eradicate pathological tissue causing onychocryptosis or dystrophy while preserving normal perionychial structures. The critical step in preventing recurrence, particularly nail spicules, is the complete excision of the germinal matrix. This comprehensive surgical guide details the biomechanics, wedge resection principles, and the Quenu technique for total germinal matrix excision, ensuring optimal outcomes for complex nail pathologies.
INTRODUCTION TO PERIONYCHIAL SURGERY
The rationale for partial nail fold and nail matrix removal, along with its various surgical modifications, is to definitively eliminate all pathological components causing clinical symptoms while meticulously preserving the normal nail plate and surrounding soft tissue architecture. Conditions such as chronic onychocryptosis (ingrown toenails), severe onychomycosis, and post-traumatic nail dystrophies frequently require surgical intervention when conservative measures fail.
The cornerstone of successful perionychial surgery lies in a profound understanding of the nail unit's anatomy. The procedure typically involves a precise wedge resection of the nail plate, the underlying nail bed, and the hypertrophic nail fold. However, the most notorious and frequent complication of wedge resection is the postoperative recurrence of nail spicules.
Clinical Pearl: The crucial factor in preventing the formation of recurrent nail spicules is the absolute and complete removal of the germinal matrix at the lateral horns. Because the apex of the surgical wedge—and consequently the narrowest area of resection—is located at the most critical tissue requiring excision, meticulous surgical technique is paramount.
ANATOMY AND BIOMECHANICS OF THE NAIL UNIT
To master nail matrix removal, the orthopedic surgeon must first master the microanatomy of the perionychium. The nail unit is a complex appendage composed of several distinct structures:
- The Nail Plate: The hard, keratinized structure produced primarily by the germinal matrix.
- The Germinal Matrix: Located proximally beneath the eponychium, extending to the distal margin of the lunula. It is responsible for approximately 90% of nail plate generation.
- The Sterile Matrix: Extends from the lunula to the hyponychium. It provides strong adherence to the nail plate and contributes slightly to its thickness.
- The Eponychium (Cuticle): The proximal skin fold that overlies the germinal matrix and protects the proximal nail fold from environmental pathogens.
- The Paronychium: The lateral soft tissue folds that guide the directional growth of the nail plate.
- The Hyponychium: The distal specialized epidermis beneath the free edge of the nail, serving as a waterproof seal.
Pathophysiology of Recurrence
When performing a partial nail fold removal, the surgeon creates a wedge excision. The base of this wedge is distal, and the apex is proximal, extending deep beneath the eponychium. The anatomical lateral horns of the germinal matrix curve proximally and laterally, often extending further than visually apparent. If the apex of the surgical wedge fails to capture the entirety of this lateral horn, the retained germinal matrix cells will continue to produce keratinized tissue, resulting in a sharp, highly symptomatic nail spicule that pierces the healing paronychium.
INDICATIONS FOR SURGICAL INTERVENTION
Surgical management of the nail unit is indicated in several clinical scenarios, ranging from acute infections to chronic dystrophies.
Partial Nail Fold and Matrix Removal (Wedge Resection)
- Recurrent Onychocryptosis: Ingrown toenails that have failed conservative management (e.g., taping, orthonyxia, oral antibiotics).
- Hypertrophic Granulation Tissue: Chronic irritation leading to exuberant, bleeding granulation tissue at the lateral nail fold.
- Focal Nail Dystrophy: Localized trauma or benign tumors (e.g., glomus tumor, subungual exostosis) requiring partial resection for access or excision.
Total Germinal Matrix Excision (Quenu / Zadik / Fowler Technique)
- Chronic Symptomatic Onychomycosis: Severe fungal infections resistant to prolonged systemic and topical antifungal therapies, particularly when accompanied by painful onychogryphosis (ram's horn nail).
- Severe Global Nail Dystrophy: Psoriatic nail disease or post-traumatic dystrophy causing intractable pain or functional impairment.
- Recurrent Global Onychocryptosis: Cases where bilateral partial resections have repeatedly failed.
PREOPERATIVE PREPARATION AND POSITIONING
Anesthesia
Perionychial surgery is exquisitely painful; therefore, profound local anesthesia is required. A standard digital ring block or a Mayo block utilizing 1% to 2% Lidocaine without epinephrine, often combined with 0.5% Bupivacaine for prolonged postoperative analgesia, is recommended.
Surgical Warning: Never use epinephrine in digital blocks for patients with known peripheral vascular disease, Raynaud's phenomenon, or severe microvascular compromise, as it may precipitate digital ischemia.
Hemostasis
A bloodless surgical field is mandatory to accurately identify and excise the translucent germinal matrix. Exsanguinate the digit using an Esmarch bandage or a sterile glove finger cut at the tip, rolling it proximally to the base of the digit. Secure it as a digital tourniquet. Ensure the tourniquet time does not exceed 30 to 45 minutes.
SURGICAL TECHNIQUE: TOTAL GERMINAL MATRIX EXCISION (QUENU TECHNIQUE)
The Quenu technique (also modified by Fowler and Zadik) is the gold standard for total germinal matrix excision in cases of chronic, symptomatic onychomycosis or severe dystrophy. The objective is to remove the entire nail plate and the germinal matrix while preserving the sterile matrix and the eponychial fold.
Step 1: Skin Incisions
Following adequate anesthesia and exsanguination, the surgical approach begins with precise incisions to mobilize the proximal nail fold. Two oblique incisions are made extending proximally and slightly laterally from the corners of the proximal nail fold.

These incisions must be deep enough to release the eponychium but careful to avoid damaging the underlying extensor hallucis longus tendon insertion.

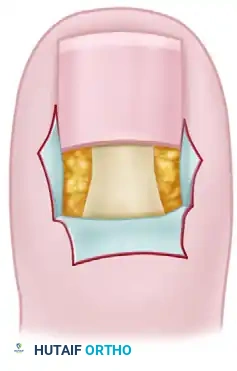
Step 2: Nail Plate Removal
A Freer elevator or a specialized nail elevator is introduced beneath the free edge of the nail plate, gently separating it from the underlying sterile matrix. The elevator is advanced proximally until the entire nail plate is freed from the germinal matrix and the eponychial fold. The nail plate is then grasped with a sturdy hemostat and removed with a rolling motion.

Step 3: Elevation of the Eponychial Flap
Using fine skin hooks or delicate forceps, the eponychial flap is reflected proximally. This maneuver exposes the entire germinal matrix.
It is critical to differentiate the germinal matrix from the sterile (dormant) matrix. The germinal matrix typically appears as a thicker, slightly more opaque, and often protruding tissue layer beneath the eponychium, whereas the sterile matrix is thinner and firmly adherent to the periosteum of the distal phalanx. In cases of chronic onychomycosis, the dormant matrix may appear abnormal or damaged by the mycotic process.

Step 4: Excision of the Germinal Matrix
This is the most critical step of the procedure. A transverse incision is made at the junction of the germinal and sterile matrices (the distal border of the lunula). The germinal matrix is then sharply dissected off the underlying periosteum of the distal phalanx, working proximally.
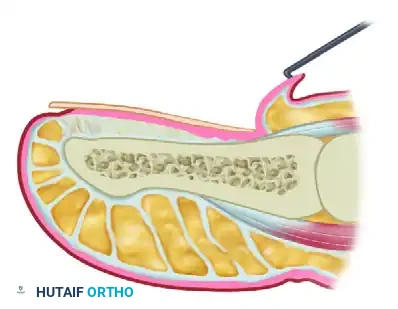
Surgical Pitfall: The lateral horns of the germinal matrix curve deeply into the proximal-lateral corners of the distal phalanx. Failure to aggressively curette or sharply excise these hidden recesses will guarantee the formation of postoperative spicules.
All germinal matrix tissue must be meticulously removed. Some surgeons advocate for the adjunctive use of chemical cautery (e.g., 89% phenol or 10% sodium hydroxide) applied strictly to the proximal cul-de-sac to ensure the destruction of any microscopic remnants, though sharp excision alone is sufficient if performed perfectly.


Step 5: Closure and Eponychial Replacement
Once hemostasis is verified (by temporarily releasing the tourniquet if necessary), the eponychial flap is repositioned distally. The eponychium is replaced adjacent to the remaining dormant (sterile) matrix.

The oblique skin incisions are closed using fine non-absorbable sutures (e.g., 4-0 or 5-0 nylon). The sutures should approximate the skin edges without excessive tension to prevent necrosis of the eponychial flap.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management following nail matrix removal is as critical as the surgical execution to ensure optimal healing and patient satisfaction.
Immediate Postoperative Care
- Dressing: A non-adherent dressing (e.g., Adaptic or Xeroform) is applied directly over the exposed sterile matrix and surgical incisions. This is followed by sterile gauze and a mildly compressive cohesive bandage.
- Elevation: The patient must keep the foot strictly elevated above heart level for the first 48 to 72 hours to minimize edema, throbbing pain, and the risk of postoperative hematoma.
- Analgesia: Oral NSAIDs and acetaminophen are usually sufficient, though a short course of stronger analgesics may be required for the first 24 hours.
Footwear Restrictions and Return to Activity
Patient education regarding footwear is paramount. The patient must be explicitly instructed not to wear a closed-toe shoe, even if the toe box is exceptionally wide, for a minimum of 10 to 14 days. Premature use of closed footwear causes micro-trauma to the healing eponychial flap and increases the risk of surgical site infection.
Clinical Pearl: The patient should be informed before surgery that it may take 3 to 4 weeks before a standard shoe can be worn comfortably for an 8-hour workday. Managing patient expectations regarding the recovery timeline prevents postoperative dissatisfaction.
Long-Term Outcomes and Complications
Following a total germinal matrix excision, the patient will be left with anonychia (absence of the nail plate). The exposed sterile matrix will eventually epithelialize and toughen, taking on the appearance of normal skin.
However, patients must be warned that after germinal matrix removal, the remaining sterile matrix may continue to produce flaky cornifications or a thin, pseudo-nail structure. This is a normal physiological response of the sterile matrix attempting to keratinize and should not be mistaken for a recurrence of the true nail plate.

Management of Complications
- Nail Spicules: If a spicule forms due to retained lateral horn matrix, a revision surgery is required. The spicule must be traced proximally, and the offending matrix remnant must be surgically excised or chemically ablated.
- Infection: Superficial surgical site infections are managed with oral antibiotics targeting skin flora (e.g., Cephalexin) and warm saline soaks. Deep infections may require partial suture removal for drainage.
- Epidermal Inclusion Cysts: Rarely, epithelial cells can be driven deep during the surgical approach, leading to cyst formation. These present as painful, slow-growing nodules beneath the eponychium and require surgical enucleation.
CONCLUSION
Partial nail fold and nail matrix removal, particularly the comprehensive Quenu technique, are highly effective procedures for eradicating chronic, debilitating perionychial pathology. The success of these interventions hinges entirely on the surgeon's anatomical knowledge and meticulous execution—specifically, the complete eradication of the germinal matrix to prevent spicule recurrence. By adhering to strict surgical principles and guiding patients through a structured postoperative footwear protocol, orthopedic surgeons can achieve excellent, long-lasting functional and cosmetic outcomes.
You Might Also Like


