Disorders of the Anterior Tibial Tendon: A Comprehensive Surgical Guide
Key Takeaway
Disorders of the anterior tibial tendon, including tenosynovitis and acute rupture, present unique biomechanical challenges. While less common than posterior tibial tendon pathology, missed diagnoses can lead to progressive pes planus and drop foot. This guide details evidence-based diagnostic protocols, conservative management, and step-by-step surgical techniques for synovectomy, primary repair, and delayed tendon transfer reconstructions.
INTRODUCTION TO ANTERIOR TIBIAL TENDON PATHOLOGY
Disorders of the anterior tibial tendon (ATT), primarily encompassing tenosynovitis and acute or chronic rupture, represent a relatively uncommon but functionally debilitating spectrum of foot and ankle pathology. Compared to the high incidence of posterior tibial tendon dysfunction or peroneal tendon disorders, clinical presentations involving the anterior tibial tendon are rare. However, because the anterior tibial muscle is the primary dorsiflexor of the ankle—accounting for approximately 80% of dorsiflexion power—loss of its continuity severely disrupts the normal gait cycle.
The anterior tibial tendon functions critically during two phases of gait: it contracts concentrically during the swing phase to provide ground clearance for the foot, and it contracts eccentrically at heel strike to decelerate plantarflexion, preventing "foot slap." Understanding the biomechanics, precise anatomical constraints, and vascular watershed zones of this tendon is paramount for the orthopedic surgeon when formulating a treatment algorithm for tenosynovitis, acute ruptures, and delayed presentations.
SURGICAL ANATOMY AND BIOMECHANICS
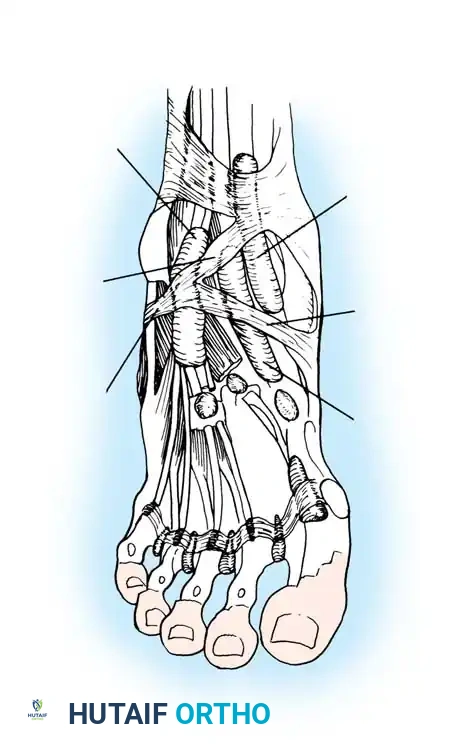
The anterior tibial muscle originates from the lateral condyle and proximal two-thirds of the lateral surface of the tibia, as well as the interosseous membrane. As it transitions into a tendinous structure in the distal third of the leg, it passes through a distinct fibro-osseous tunnel.
The Retinacular System and Insertion
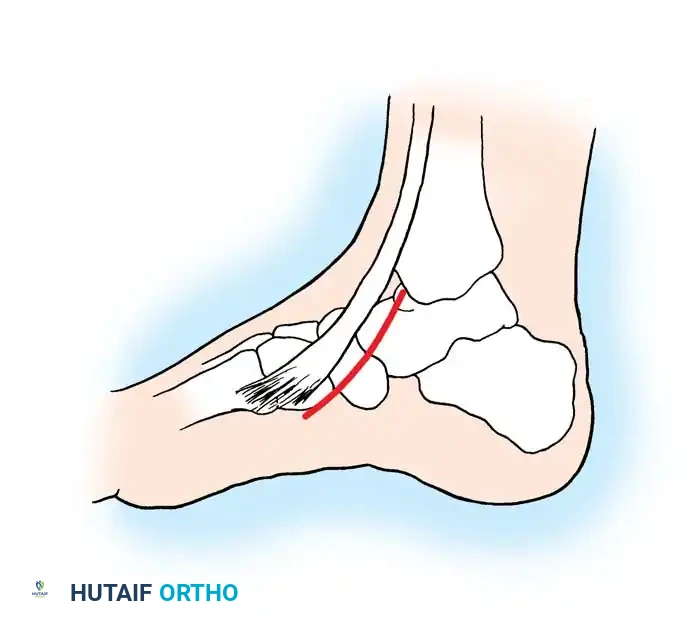
The tendon courses beneath the superior extensor retinaculum and then enters the inferior extensor retinaculum. The anatomical configuration at the inferior extensor retinaculum is of critical clinical significance. As the superomedial limb of the inferior extensor retinaculum reaches the anterior tibial tendon from its lateral side, it divides into an anterior and posterior "glove," completely encircling the tendon as it passes toward its insertion.
The tendon ultimately inserts into the medial and plantar surfaces of the medial cuneiform and the base of the first metatarsal. A highly constant bursa lies deep to the tendon at its insertion site, which can become a nidus for localized inflammation.
Pathoanatomy of Rupture
The anterior tibial tendon generally loses continuity in one of two distinct clinical scenarios:
1. The Attritional Rupture (Elderly Demographic): Typically seen in physically active men over the age of 60. The rupture is often spontaneous and occurs during routine sports or activities. This is rarely a true acute traumatic event; rather, it is the culmination of attritional loss of continuity. Synovitis around the ankle joint can cause the retinacular "envelope" to constrict the tendon. This extrinsic pressure induces localized ischemic changes within the tendon's watershed zone, leading to degenerative tearing.
2. The Acute Traumatic Rupture (Young Adult Demographic): Occurs when a young athlete forcefully dorsiflexes an acutely plantarflexed foot against extreme resistance (e.g., during a tackle in American football or a blocked kick in soccer). This eccentric overload exceeds the ultimate tensile strength of the healthy tendon.
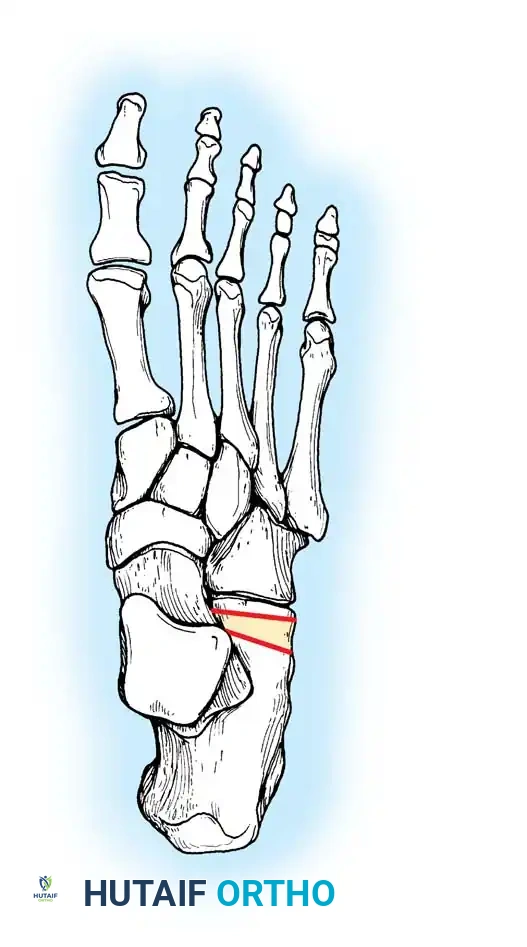
Ruptures typically occur at one of two locations: directly at the insertion into the medial cuneiform/first metatarsal base, or proximally beneath the superomedial limb of the inferior extensor retinaculum.
CLINICAL EVALUATION AND DIAGNOSIS
Patient History and Physical Examination
The hallmark presenting complaint is weakness in ankle dorsiflexion accompanied by a variable degree of pain over the anterior aspect of the ankle. Distance runners frequently present with chronic, activity-limiting pain indicative of tenosynovitis rather than rupture.
On physical examination, patients with a complete rupture will demonstrate a "steppage gait" to avoid tripping, or a noticeable "foot slap" at heel strike. A critical observational finding is the recruitment of secondary dorsiflexors: the patient will actively hyperextend the toes using the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) to clear the foot during the swing phase.
Depending on the chronicity of the injury, a palpable defect may be present over the anterior ankle. However, in delayed presentations, the tendon may have healed in an elongated, non-functional position via a bridge of scar tissue in continuity, masking the palpable gap. In cases of florid tenosynovitis, marked crepitance and swelling are palpable along the tendon sheath.
Clinical Pearl: Always test dorsiflexion strength with the toes actively plantarflexed. This eliminates the substitution effect of the EHL and EDL, isolating the anterior tibial tendon and unmasking subtle weakness.
Imaging and Concomitant Deformities
While the physical examination is frequently definitive, advanced imaging is highly recommended. Magnetic Resonance Imaging (MRI) is the gold standard, confirming the diagnosis, localizing the level of the tear, and quantifying the degree of tendon retraction and muscle atrophy.
Furthermore, chronic anterior tibial tendon dysfunction can lead to secondary biomechanical collapse of the foot. Mann has reported progressive pes planus deformities in elderly patients following unrecognized ruptures of this tendon. In severe, chronic cases of secondary flatfoot, reconstructive procedures such as an Evans anterior calcaneal osteotomy may eventually be required to restore the longitudinal arch by elongating the lateral column.
MANAGEMENT OF TENOSYNOVITIS
Conservative Treatment
Distance runners and athletes suffering from isolated tenosynovitis should first undergo a rigorous non-operative protocol. The cornerstone of treatment is immobilization in a removable or nonremovable short-leg walking cast or controlled ankle motion (CAM) boot.
The immobilization device must be worn continuously for 3 weeks (removed only for bathing if a prefabricated boot is used), followed by an additional 3 weeks of use during ambulation. Oral nonsteroidal anti-inflammatory drugs (NSAIDs) are utilized adjunctively.
Surgical Warning: If a corticosteroid injection is deemed necessary for resistant cases, it must be placed judiciously within the tendon sheath under ultrasound guidance. Intratendinous injection is strictly contraindicated as it significantly increases the risk of iatrogenic rupture.
Operative Treatment: Synovectomy
Synovectomy of the anterior tibial tendon is seldom required, except in cases refractory to prolonged conservative care or in patients with inflammatory arthritides (e.g., rheumatoid arthritis).
When planning the surgical approach, the surgeon must be acutely aware that any incision across the anteromedial aspect of the ankle is prone to hypertrophic scarring.

Surgical Technique 85-6: Synovectomy of the Anterior Tibial Tendon
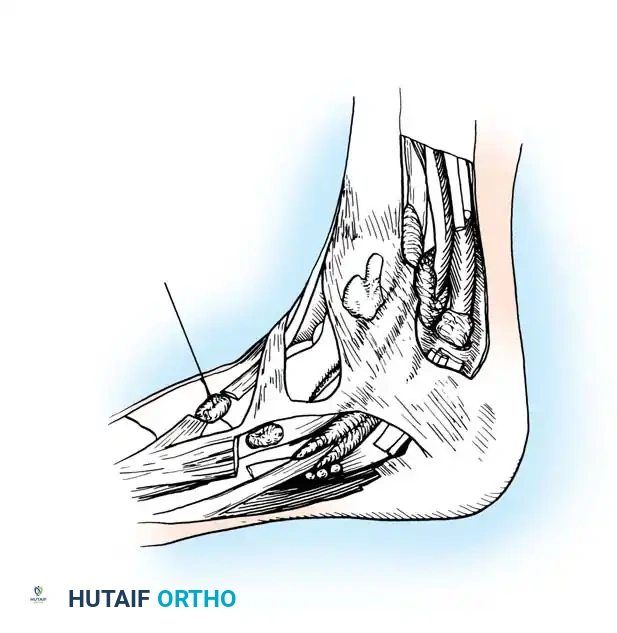
- Incision and Exposure: Begin the incision just distal to the ankle joint. Carry the incision medially and posteriorly to the anterior tibial tendon, extending 5 to 6 cm distally. It is critical to stay 2 to 3 mm medial to the tendon, continuing almost to its insertion. Do not cross the ankle joint crease perpendicularly.
- Neurovascular Protection: Meticulously isolate the communicating branches of the saphenous vein as they course plantarward; preserve as many as possible to prevent postoperative venous congestion. The terminal branches of the saphenous nerve frequently lie just deep to the saphenous vein and must be protected to avoid painful neuromas.
- Sheath Debridement: Raise the anterior skin flap only as much as necessary to expose the tendon. Open the tendon sheath longitudinally. Perform a thorough debridement of the hypertrophic synovium. By passively dorsiflexing the ankle and applying distal traction on the tendon, the surgeon can deliver and excise most of the synovium, even tissue located proximal to the ankle joint line.
- Retinacular Release: If the tendon is severely constricted, incise the superomedial band of the inferior extensor retinaculum. Resuturing this band is unnecessary, technically difficult, and risks re-constriction.
- Closure: Obtain meticulous hemostasis. Close the skin only, avoiding deep dermal sutures that may tether the tendon. Apply a bulky compressive dressing and a short-leg walking cast.
Postoperative Protocol for Synovectomy:
* Days 1-7: Crutches are used. Weight-bearing to tolerance is permitted in the cast.
* Days 12-16: The cast is removed for suture removal. A new short-leg cast is applied.
* Weeks 2-6: The patient remains in the cast.
* Weeks 6-12: Transition to a compressive ankle corset or sleeve for an additional 4 to 6 weeks while initiating physical therapy for range of motion.
MANAGEMENT OF ACUTE TENDON RUPTURE
The decision to proceed with operative treatment for a complete rupture is dictated by the patient's physiological age, functional demands, and degree of impairment. Unlike posterior tibial tendon ruptures, which almost universally lead to progressive deformity, an anterior tibial tendon rupture can sometimes be tolerated in low-demand elderly patients. Non-operative management consists of a short-leg brace (AFO) with a 90-degree plantarflexion stop for 3 to 6 months, which may allow the tendon to heal in continuity via scar tissue, providing acceptable function.
For active patients, primary surgical repair is indicated to restore dorsiflexion power and prevent gait dysfunction.
Surgical Technique 85-7: Primary Repair of Complete Rupture
- Incision: Utilize the same anteromedial incision described for synovectomy.
- Tendon Retrieval: If the tendon has ruptured beneath the inferomedial limb of the inferior extensor retinaculum, incise this band. Grasp the proximal stump and advance it as far distally as possible.
- Retrieval Pearl: If the tendon has retracted proximal to the superomedial limb, incise this limb. Slowly pass a hemostat or tendon passer proximally through the sheath to retrieve it. If unsuccessful, make a separate small (2-3 cm) anteromedial incision above the ankle, identify the tendon at the tibial border, and pass it distally using a curved clamp or by suturing it to a rubber urinary catheter and pulling it through the sheath.
- Preparation of the Insertion Site: Expose the medial cuneiform. Drill a hole from dorsal to plantar. Elevate the inferior flap and the abductor hallucis muscle plantarward just enough to visualize the drill bit emerging. Enlarge the hole incrementally to 1/4 inch or 5/16 inch to accommodate the tendon stump.
- Tendon Weave and Fixation: Place a Bunnell or Krackow weave using #0 or #2 nonabsorbable suture on free straight needles into the distal end of the proximal tendon stump. Pass the suture ends through the osseous tunnel in the medial cuneiform.
- Tensioning: Pull the tendon firmly into the hole. While holding the ankle in 20 to 30 degrees of dorsiflexion, tie the sutures over the plantar bony bridge or secure them to the adjacent plantar periosteum and deep fascia.
- Alternative Navicular Insertion: If the tendon is severely retracted and cannot reach the medial cuneiform despite mobilization, the navicular may be used as an alternative bony insertion.
- Technical Pitfall: Dissection plantar to the navicular is tedious due to the intervening posterior tibial tendon. The surgeon must stay plantar to the posterior tibial tendon, dissecting the abductor hallucis plantarward while protecting the crossing long toe flexor tendons.
- Pass the tendon through a drill hole in the middle of the navicular. Suturing in this deep plantar location is challenging; the use of a small, free, curved cutting needle (e.g., a No. 7 Murphy needle) is highly recommended. Suture the tendon under tension to the inferior surface of the navicular with the ankle dorsiflexed.
Postoperative Protocol for Primary Repair:
The aftertreatment mirrors that of the synovectomy, but strict non-weight-bearing is enforced for the first 4 weeks, followed by progressive weight-bearing in a CAM boot locked in neutral to slight dorsiflexion.
MANAGEMENT OF DELAYED DIAGNOSIS AND CHRONIC RUPTURE
Anterior tibial tendon ruptures frequently present as delayed diagnoses. This occurs either because the initial functional deficit was mild (due to EHL/EDL substitution) or because the injury was misdiagnosed as a simple ankle sprain.
In chronic settings, the proximal muscle belly retracts and undergoes fatty infiltration, and the tendon gap fills with incompetent fibrous scar tissue. Primary end-to-end repair is usually impossible. Markarian et al. defined several reconstructive options:
* Primary repair after aggressive debridement of interposed fibrous tissue (rarely feasible).
* Tendon debridement with a sliding anterior tibial tendon lengthening graft (V-Y advancement).
* Adjacent tendon transfer utilizing either the Extensor Hallucis Longus (EHL) or Extensor Digitorum Longus (EDL).
Surgical Technique 85-8: Adjacent Tendon Transfer (EHL/EDL)
- Incision and Debridement: Make a longitudinal incision between the saphenous and superficial peroneal nerves on the anterior aspect of the ankle. Carefully preserve the superior extensor retinaculum to prevent postoperative bowstringing. Identify the anterior tibial tendon. Excise all interposed fibrous tissue until healthy, organized tendon fibers are reached proximally.
- Graft Harvest: Choose either the EHL or EDL tendon for transfer. The EHL is most commonly selected due to its robust size and synergistic vector. Detach the chosen tendon distally at the level of the metatarsophalangeal joint.
- Distal Stump Management: To prevent a drop-toe deformity, suture the distal stump of the harvested EHL to the adjacent extensor digitorum brevis (EDB) or extensor hallucis brevis (EHB) tendon.
- Tendon Transfer and Weave: Bring the proximal portion of the harvested EHL/EDL into the primary wound. If the distal stump of the anterior tibial tendon is viable and of sufficient length, perform a side-to-side transfer or a formal Pulvertaft weave to definitively repair the distal segment.
- Bony Fixation (If Avulsed): If the distal ATT stump is avulsed or incompetent, create a dorsal-to-plantar drill hole in the medial cuneiform. Pass the transferred tendon through the hole and secure it. Modern techniques highly favor the use of an interference tenodesis screw or a robust bone anchor for rigid fixation, allowing for earlier rehabilitation.
- Tensioning: The ankle must be positioned in neutral (0 degrees) during final tensioning and fixation.
- Closure: Leave the inferior extensor retinaculum open over the repair site to prevent restrictive adhesions that would limit the excursion of the new tendon graft. Close the subcutaneous tissue and skin meticulously.
Postoperative Protocol for Tendon Transfer:
* Weeks 0-2: A well-padded posterior splint is applied in neutral dorsiflexion. Strict non-weight-bearing. Sutures are removed at 10 to 14 days.
* Weeks 2-4: Transition to a non-weight-bearing short leg cast.
* Weeks 4-6: Transition to a weight-bearing cast or CAM boot.
* Weeks 6+: A removable ankle-foot orthosis (AFO) is applied. Formal physical therapy is instituted, focusing on restoring ankle range of motion, retraining the transferred tendon (biofeedback), and aggressive calf strengthening to restore the gait cycle. Return to high-impact activity is generally restricted for 6 to 9 months.
You Might Also Like


