Ankle Malunion Reconstruction: Surgical Techniques & Biomechanics
Key Takeaway
Ankle malunion frequently results from inadequate fibular fixation or unrecognized syndesmotic disruption, leading to altered joint biomechanics and posttraumatic arthritis. Even 2 mm of fibular shortening or 5 degrees of external rotation significantly increases talar contact pressures. Successful joint-preserving reconstruction requires anatomical restoration of fibular length, correction of rotation, and a parallel mortise. When advanced arthritis is present, salvage procedures such as arthrodesis or arthroplasty become necessary to restore functional, pain-free weight-bearing.
Introduction to Ankle Malunion
The anatomical integrity of the ankle mortise is paramount for normal lower extremity biomechanics and pain-free weight-bearing. Occasionally, malunion occurs even after the most accurate reduction of closed ankle fractures. More commonly, it develops after seemingly "stable" injuries that subsequently displace, often characterized by widening of the mortise due to unrecognized or inadequately treated syndesmotic disruption.
Malunion frequently develops if the initial internal fixation of the fibula is inadequate, allowing the lateral malleolus to shorten and externally rotate. Because the talus faithfully follows the lateral malleolus, fibular shortening leads to lateral talar shift and profound incongruity of the tibiotalar joint. The disability resulting from a malunited ankle fracture can be so extreme that symptomatic relief and functional restoration can be obtained only through complex reconstructive surgery.
Biomechanics and Pathoanatomy
The ankle is a highly congruent, weight-bearing hinge joint. Even a minor varus or valgus deformity of the joint produces an abnormal weight-bearing alignment, rapidly accelerating the onset of posttraumatic arthritis.
The biomechanical consequences of fibular malreduction have been extensively documented in orthopedic literature. While some early cadaveric studies suggested that factors other than the absolute magnitude of normal contact stresses might play a role in the pathogenesis of posttraumatic arthritis, the prevailing biomechanical consensus is clear regarding spatial displacement.
Biomechanical Pearl:
A landmark cadaver study demonstrated that 2 mm or more of fibular shortening or lateral displacement, or 5 degrees or more of external rotation, increases contact pressures significantly in the posterolateral and midlateral quadrants of the talar dome. Concurrently, a corresponding decrease in contact pressures is noted in the medial quadrants. This asymmetric loading rapidly degrades the articular cartilage.
Anatomical reduction of pronation-lateral rotation fractures of the lateral malleolus is therefore critical. Failure to restore the exact length and rotation of the fibula inevitably leads to altered kinematics, chronic pain, and degenerative joint disease.
Preoperative Evaluation and Imaging
Patients with ankle malunion typically present with chronic pain, swelling, restricted range of motion, and a visible deformity. A thorough clinical examination must assess hindfoot alignment, subtalar motion, and the presence of any compensatory deformities. In patients with poor clinical results, bilateral fractures and concurrent subtalar arthritis frequently contribute to severe gait abnormalities and restricted hindfoot motion.
Standard weight-bearing anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory. However, occult malunions—particularly those involving subtle fibular shortening or rotational malalignment—are best evaluated with computed tomography (CT).
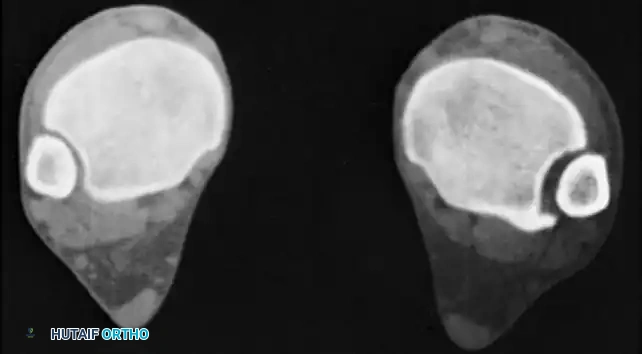
FIGURE 58-9 CT scan of occult malunion. Right ankle (left) is normal; left ankle (right) shows widening of the distal tibiofibular joint, indicating fibular shortening and external rotation of the lateral malleolus. (From Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus, J Bone Joint Surg 71A:521, 1989.)
Criteria for Joint-Preserving Osteotomy
Up to 78% good to excellent results have been reported with fibular osteotomy and lengthening for ankle malunion. The strict criteria for attempting a joint-preserving osteotomy include:
* Radiographic confirmation of malunion (as seen in Fig. 58-9).
* A demonstrable, preserved joint space on AP and mortise views.
* Sufficient remaining articular cartilage covering the tibial plafond and the talar dome.
Contraindications to joint-preserving osteotomies include:
* Ankylosis of the tibiotalar joint.
* Severe loss of bone stock.
* Advanced, severe degenerative arthritis (bone-on-bone articulation).
Principles of Anatomical Restoration
To achieve a successful joint-preserving reconstruction, the surgeon must adhere to three non-negotiable requirements for the anatomical restoration of the ankle joint:
- A Perfectly Equidistant and Parallel Joint Space: The clear space between the talus and the tibial plafond must be uniform across the entire articulation.
- Restoration of Fibular Length: The "fibular spike" must be in its normal position, pointing exactly to the level of the distal tibial subchondral bone. This radiographic landmark confirms that the length of the fibula has been accurately restored.
- Normal Talofibular Contour: There must be a normal contour at the lateral part of the articular surface of the talus, continuing as an unbroken curve into the recess of the distal fibula where the peroneal tendons lie (the Shenton line of the ankle).
Surgical Options for Ankle Malunion
Operations to correct malunited ankle fractures generally fall into three categories:
1. Osteotomy of the fractured fibula and/or medial malleolus with restoration of fibular length and rigid internal fixation.
2. Supramalleolar osteotomy when only realignment of the lower extremity mechanical axis is required (extra-articular deformity).
3. Arthrodesis of the ankle (with or without supramalleolar osteotomy) for end-stage arthritis.
Although a wide variety of malunions can occur, the procedures described below can be modified to treat the vast majority of clinical presentations.
Surgical Technique: Fibular Lengthening and Derotation Osteotomy
When the primary pathology is a shortened, externally rotated fibula, a lengthening osteotomy is the procedure of choice.
Approach and Osteotomy
- Incision: Make a longitudinal lateral incision over the previous surgical scar or directly over the fibula, extending distally to the tip of the lateral malleolus.
- Exposure: Elevate full-thickness flaps. Carefully identify and protect the superficial peroneal nerve proximally and the sural nerve distally.
- Syndesmotic Takedown: Expose the distal tibiofibular syndesmosis. In chronic malunions, the syndesmosis is often filled with dense scar tissue. This must be meticulously excised to allow the fibula to mobilize and the talus to medialize.
- Osteotomy: Perform an oblique or step-cut osteotomy through the previous fracture site. A transverse osteotomy may be used if a structural bone graft is planned.
- Distraction: Apply a laminar spreader or a specialized articulated distractor between the proximal and distal fibular segments. Distract the osteotomy until the lateral malleolus is pushed distally.
- Assessment: Verify the restoration of the fibular length (the fibular spike pointing to the tibial subchondral line) and the correction of external rotation using fluoroscopy. The talus should passively follow the fibula, restoring the medial clear space.
Fixation and Grafting
- Graft Placement: Once anatomical length and rotation are achieved, measure the resulting gap. Harvest a structural tricortical bone graft from the ipsilateral iliac crest and impact it into the defect.
- Plating: Secure the construct with a robust, pre-contoured anatomical locking plate. Ensure at least three bicortical screws are placed in both the proximal and distal segments.
- Syndesmotic Fixation: If the syndesmosis remains unstable after fibular length is restored, place one or two syndesmotic screws or flexible fixation devices to maintain the reduction of the distal tibiofibular joint.
Surgical Technique: Adjunctive Calcaneal Osteotomy
In cases where ankle malunion has led to a secondary, rigid hindfoot deformity, or when offloading a specific compartment of the ankle is desired, an adjunctive calcaneal osteotomy may be required. The following technique describes an opening wedge calcaneal osteotomy utilizing a structural graft.
🔪 Surgical Technique: Calcaneal Osteotomy for Hindfoot Realignment
Step 1: Surgical Approach
* Approach the calcaneus through an oblique lateral incision.
* Surgical Warning: Meticulously protect and retract the superficial branches of the peroneal nerve and the sural nerve, which are at high risk during the lateral exposure of the hindfoot.
Step 2: Anatomical Identification
* Identify the sustentaculum tali by carefully probing over the dorsum of the exposed calcaneus. This serves as a critical medial landmark to ensure the osteotomy does not violate the medial neurovascular bundle.
Step 3: Preparation of the Osteotomy Site
* Shave the lateral border of the widened calcaneus if exostoses are present.
* Incise the periosteum directly in line with the planned osteotomy. Start laterally, approximately 2.5 cm proximal to the calcaneocuboid joint, specifically in the interval between the middle and posterior facets of the subtalar joint.
Step 4: Executing the Osteotomy
* Make a lateral-to-medial oblique osteotomy using an oscillating saw.
* The osteotomy line should be directed slightly oblique from proximal-lateral to distal-medial.
* Clinical Pearl: The required depth and trajectory of the osteotomy must be meticulously estimated from preoperative calcaneal axial radiographs or CT scans to avoid medial cortical blowout.
Step 5: Distraction and Grafting
* Open the osteotomy gently with a large osteotome or lamina spreader.
* Crucial Step: Preserve the periosteum of the medial calcaneus. An intact medial periosteal hinge is essential to prevent uncontrolled medial displacement or translation of the posterior tuberosity fragment.
* Take a suitably sized tricortical bone graft from the posterior iliac crest. Place it securely into the lateral osteotomy site to maintain the correction. Add local bone shavings or cancellous allograft to fill any remaining voids.
Step 6: Internal Fixation
* Through a separate, small posterior stab approach, place one or two large-diameter (e.g., 6.5 mm or 7.3 mm) cannulated screws through the long axis of the calcaneus, compressing the posterior tuberosity against the anterior segment and securing the graft.
Postoperative Care for Calcaneal Osteotomy
Postoperatively, the patient is placed in a well-padded short leg splint. Once swelling subsides, they are transitioned to a rigid cast. The patient is kept strictly non-weight-bearing for 6 weeks. Following radiographic evidence of early consolidation, the patient is placed in a walking cast or controlled ankle motion (CAM) boot for an additional 6 weeks. Thereafter, the patient may transition to normal shoes with supportive orthotics.
Salvage Procedures: Arthrodesis and Arthroplasty
Osteotomies have proven significantly less successful in treating bimalleolar malunions associated with moderate-to-severe arthritis. While an osteotomy can successfully restore the weight-bearing alignment of the ankle, pain and swelling frequently persist due to irreversible arthritic deterioration of the cartilage.
Some authors have historically recommended realignment osteotomies as the initial treatment for all symptomatic ankle malunions, regardless of the patient's age, time elapsed from the initial injury, severity of the malunion, or the presence of early arthritic changes. However, modern evidence dictates that while mild arthritis is not an absolute contraindication to osteotomy, significant chondral damage is highly indicative of a poor functional result.
Ankle Arthrodesis
Ankle arthrodesis (fusion) or total ankle arthroplasty (replacement) should be strongly considered in patients with severe arthritic changes and severely impaired function, or in patients who remain significantly symptomatic after a failed joint-preserving osteotomy.
When counseling patients for arthrodesis, it is important to remember—and to inform the patient—that walking on uneven or rough ground will be permanently difficult after a fusion. This difficulty is exponentially magnified if the subtalar joint is secondarily fibrosed, arthritic, or ankylosed.
Surgical Pitfall:
Complication rates as high as 30% have been reported following ankle arthrodesis for posttraumatic malunion. The most frequent major complications include nonunion, delayed union, and secondary malunion, often necessitating revision surgery.
Ilizarov Reconstruction for Complex Malunions
In cases of severe, complex malunions—particularly those complicated by infection, poor soft tissue envelopes, or previous failed arthrodesis—circular external fixation offers a powerful salvage tool.
Paley et al. extensively documented the treatment of malunion after ankle arthrodesis utilizing Ilizarov reconstruction. They concluded that the Ilizarov apparatus can simultaneously treat complex foot deformities, correct limb length discrepancies, and eradicate deep bone infections, ultimately achieving a solid union and a plantigrade foot.
However, the use of circular frames is highly demanding for both the surgeon and the patient. In Paley's series, 20 major complications requiring additional surgery occurred during the active treatment phase, and seven occurred after frame removal (four of which required further surgical intervention). Therefore, Ilizarov reconstruction should be reserved for highly selected patients managed in specialized limb reconstruction centers.
Conclusion
The management of ankle malunion requires a profound understanding of lower extremity biomechanics and meticulous preoperative planning. Anatomical restoration of the fibula is the cornerstone of joint-preserving surgery, requiring exact correction of length, rotation, and syndesmotic alignment. When adjunctive procedures like calcaneal osteotomies are required, strict adherence to surgical technique ensures optimal realignment of the hindfoot axis. In the presence of advanced posttraumatic arthritis, salvage procedures such as arthrodesis remain the gold standard for providing a stable, plantigrade, and pain-free limb, despite their inherent risks and biomechanical trade-offs.
You Might Also Like