

About This Board Review Set
This is Part 18 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 18
This module focuses heavily on: Arthroplasty, Fracture, Hip.
Sample Questions from This Set
Sample Question 1: Heat transfer from the skin to the environment when the ambient temperature exceeds 35°C primarily is attributable to...
Sample Question 2: Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?...
Sample Question 3: Figures 38a and 38b...
Sample Question 4: Assuming that the fracture shown in this radiograph (Figure 1) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active...
Sample Question 5: With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the followin...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Heat transfer from the skin to the environment when the ambient temperature exceeds 35°C primarily is attributable to
Explanation
Heat transfer from the skin to the environment occurs through conduction, convection, evaporation, and radiation. Evaporation of sweat is the primary mechanism by which core body temperature is regulated when the ambient temperature exceeds 35°C. High humidity can inhibit the evaporation of sweat, placing athletes at increased risk for heat-related illness, which is defined as a core temperature above 40°C. Symptoms include dizziness, confusion, irritability, hyperventilation, nausea, vomiting, fatigue, and collapse. Initial treatment involves rapid cooling through immersion in cold or ice water to prevent end-stage organ failure.
Question 2
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?

Explanation
Question 3
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 4
Assuming that the fracture shown in this radiograph (Figure 1) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active

Explanation
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints.
Question 5
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 6
Etanercept modifies the natural history of inflammatory arthropathies through what mechanism?
Explanation
Question 7
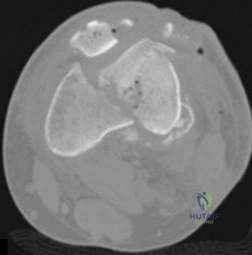
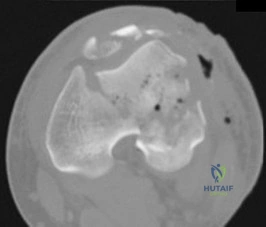
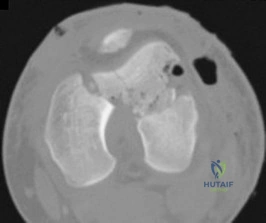
Figures below depict the radiographs obtained from a 53-year-old man who has had swelling in his right knee for 2 years, with minimal pain. He did not note an injury to the knee but has been unable to ambulate without crutches during this period. His past history is unremarkable, and he denies a history of diabetes or back problems. The social history reveals that he emigrated from China, and he works at a desk job. Physical examination shows a healthy man in no acute distress. Range of motion of the right knee is 5° to 120° actively and 0° to 120° passively, without pain. Sensation is decreased on the bottom of both feet, but otherwise the neurologic examination is unremarkable. Laboratory testing reveals a positive rapid plasma reagin (RPR) test. What is the best next step?
Explanation
This patient has a neuropathic knee caused by neurosyphilis, as shown by the joint destruction on the radiographs, with a lack of pain and a positive RPR test. He has a low-demand job and would be best treated with a hinged knee arthroplasty to provide stability for his knee.
Question 8
-Where is the physis with the highest growth rate (in mm per year) located?
Explanation

Question 9
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 10
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 11
Which of the following is considered a physiologic effect of anemia?
Explanation
REFERENCE: Carson JL, Duff A, Poses RM, et al: Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996;348:1055-1060.
Question 12
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 13
The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using
Explanation
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow, and an abnormality would be a late finding. MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
Question 14
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
Toe is fused too straight (plantar flexed)
Toe is fused in too much valgus
Toe is fused in too much dorsiflexion
There is a nonunion of the fusion
Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 15
01 (left). What is the most appropriate next step?

Explanation
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours. Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
Question 16
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results? Review Topic

Explanation
Question 17
A 64-year-old female sustains a nondisplaced distal radius fracture and undergoes closed treatment using a cast. Three months after the fracture she reports an acute loss of her ability to extend her thumb. What is the most likely etiology of her new loss of function?

Explanation
Question 18
Of the following, what is the most reliable method of assessing spinal fusion? Review Topic
Explanation
Question 19
A 25-year-old patient presents with a posterior wall/ posterior column acetabular fracture. She is scheduled for open reduction internal fixation through a posterior approach. What position of the leg exerts the least amount of intraneural pressure on the sciatic nerve?

Explanation
Question 20
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies? Review Topic
Explanation
Question 21
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Explanation
Question 22
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mmP3P (normal to 10,500/mmP3P) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of Review Topic

Explanation
Question 23
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.

Question 24
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?
Explanation
REFERENCES: Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258.
Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Greenfield MA, Insall JN, Case GC, Kelly MA: Instrumentation of the patellar osteotomy in total knee arthroplasty: The relationship of patellar thickness and lateral retinacular release. Am J Knee Surg 1996;9:129-131.
Question 25
A 69-year-old woman has rigid painful left pes planus that has become less symptomatic with casting. She has multiple comorbidities and is not a good surgical candidate. She has failed a trial of activity without any supports.
Explanation
Treatment for pes planus revolves around 2 clinical parameters: pain and rigidity. In the absence of pain, no intervention is warranted because there are no other symptoms that can reasonably be linked to the foot shape. Flexible pes planus (that corrects with heel rise) is usually normal and does not cause symptoms, but it can be associated with a symptomatic accessory navicular, in which case the patient may have pain over the medial navicular from either traction by the tibialis posterior or the act of rubbing against the medial shoe counter. Rigid pes planus is most frequently associated with a tarsal coalition, which classically presents in late adolescence but can become symptomatic for the first time in adults. The initial treatment for painful pes planus, whether flexible or rigid, is immobilization, usually in a walking cast. This often is sufficient to relieve symptoms on a permanent basis. Surgery should be contemplated only when this treatment fails. Adult-acquired flatfoot is most commonly attributable to tibialis posterior tendon dysfunction. In stage 3, the pes planus is rigid. If it is painful, surgical treatment, which consists of a triple arthrodesis, may be considered. However, if medical constraints or patient preference preclude surgery, an Arizona brace can provide sufficient support to reduce symptoms to an acceptable level to perform activities of daily living.
RECOMMENDED READINGS
Varner KE, Michelson JD. Tarsal coalition in adults. Foot Ankle Int. 2000 Aug;21(8):669-72. PubMed PMID: 10966365. View Abstract at PubMed
Lin JL, Balbas J, Richardson EG. Results of non-surgical treatment of stage II posterior tibial tendon dysfunction: a 7- to 10-year followup. Foot Ankle Int. 2008 Aug;29(8):781-6. doi: 10.3113/FAI.2008.0781. PubMed PMID: 18752775. View Abstract at PubMed
Chao W, Wapner KL, Lee TH, Adams J, Hecht PJ. Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int. 1996 Dec;17(12):736-41. PubMed PMID: 8973895. View Abstract at PubMed
Cha SM, Shin HD, Kim KC, Lee JK. Simple excision vs the Kidner procedure for type 2 accessory navicular associated with flatfoot in pediatric population. Foot Ankle Int. 2013 Feb;34(2):167-72. doi: 10.1177/1071100712467616. Epub 2013 Jan 15. PubMed PMID:
Question 26
Examination of a 41-year-old man who was thrown from a motorcycle reveals that both legs appear externally rotated and there is bruising in the perineal area. He has a blood pressure of 80/40 mm Hg, a pulse rate of 140/min, a respiratory rate of 25/min, and he appears confused. Following administration of 4 L of saline solution and 2 units of packed red blood cells, he has a blood pressure of 80/40 mm Hg, a pulse rate of 160/min, and a respiratory rate of 25/min. The abdominal assessment for intraperitoneal blood is negative. An AP radiograph shows an anteroposterior compression injury with 7 cm of symphysis diastasis but no posterior displacement in the sacroiliac joints. What is the next most appropriate step in management?
Explanation
REFERENCES: Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS: A protocol for the initial management for unstable pelvic fractures. Am Surg 1998;64:862-867.
Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 217-226.
Mucha P Jr, Welch TJ: Hemorrhage in major pelvic fractures. Surg Clin North Am 1988;68:757-773.
Question 27
A 66-year-old woman reports chronic mild low back pain. Over the last 3 years, she has noticed worsening buttock and posterior leg pain with standing and walking. Sitting seems to improve the pain. She also reports numbness in both legs with walking. An MRI scan and standing radiographs of the lumbar spine are shown in Figures 53a through 53c. She has undergone two epidural injections with good, but short-term relief. Further treatment to alleviate this patient's symptoms should consist of which of the following? Review Topic

Explanation
Question 28
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?
Explanation
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Naudie DD, Rorabeck CH: Managing instability in total knee arthroplasty with constrained and linked implants. Instr Course Lect 2004;53:207-215.
Question 29
Figure 88 is the radiograph of a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
Explanation
Based on the fact that the fracture is occurring around the stem (type B) and the stem is clearly loose (type B2), the appropriate treatment is removal of the in situ stem (which is loose), ORIF of the femur (cerclage wires, cables, or a plate would be acceptable), and insertion of a longer revision stem (a tapered fluted modular titanium or fully porous coated cylindrical stem) to bypass the fracture. All other responses are incorrect because they provide inappropriate treatment options for a Vancouver B2 fracture.
Question 30
What gene is implicated in spinal muscular atrophy? Review Topic
Explanation
Question 31
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
REFERENCES: Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20.
Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Solomonow M, Baratta R, Zhou BH, et al: The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 1987;15:207-213.
Question 32
A 13-year-old boy has had a painless mass in the arm for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 46a through 46c. What is the most likely diagnosis?
Explanation
REFERENCE: Bernstein KE, Lattes R: Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: Clinicopathologic study of 134 cases. Cancer 1982;49:1668-1678.
Question 33
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
REFERENCES: O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 34
Two weeks after undergoing total knee arthroplasty, a 68-year-old woman experiences moderate, yet worsening, knee pain. Upon examination, she can walk with a cane but she has swelling with mild reactive erythema. She has a well-healed incision with no drainage. A review of her medications reveals the she has been taking warfarin and has an international normalized ratio (INR) of 4.0. Her erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are slightly elevated, and radiographs are unremarkable other than for effusion. What is the most likely diagnosis?
Explanation
This patient likely has a hemarthrosis related to INR elevation. The slight elevations in ESR and CRP are likely attributable to the nature of the surgery itself rather than an infection, and the mild reactive erythema is likely attributable to the hemarthrosis.
Question 35
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?

Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
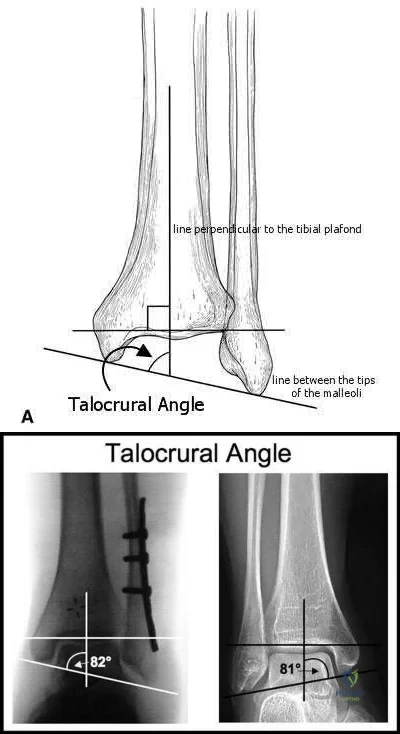
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
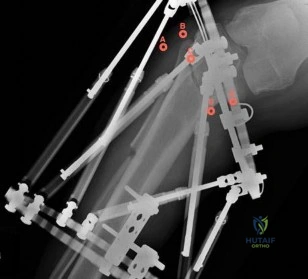
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

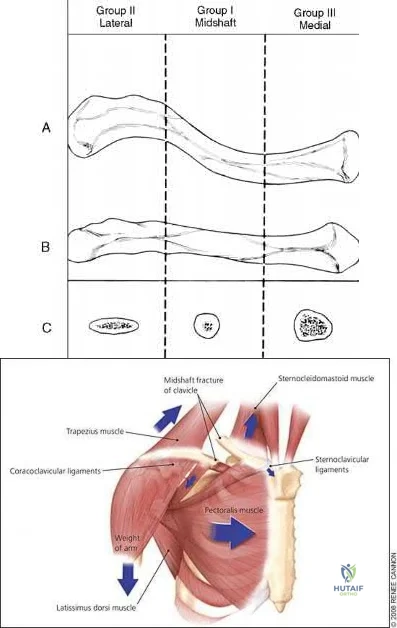
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 36
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Explanation
500 µm.
REFERENCES: Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Question 37
A B Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
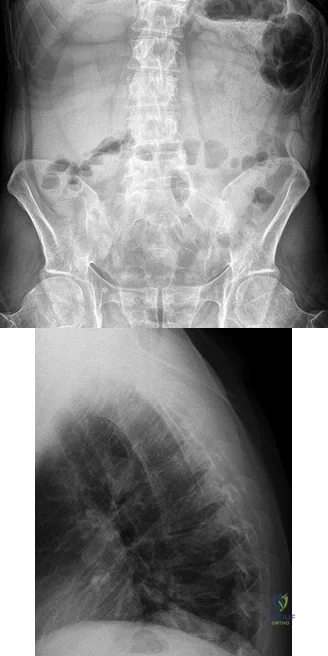
Explanation
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. View Abstract at PubMed
Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. View Abstract at PubMed
Question 38
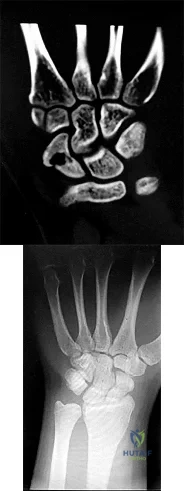
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?
Explanation
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
Question 39
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 40
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 41
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?
Explanation
REFERENCES: Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget’s disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 187-196.
Question 42
Which of the following classes of antibiotics works by binding to the 30S-ribosomal subunit?
Explanation
Aminoglycosides are among the oldest classes of antibiotics. They are act by binding to the 30S ribosomal subunit and are considered bactericidal. Due to their effectiveness on Gram-negative bacteria they are often used in conjunction with cephalosporins for treatment of open fractures. Care must be taken when using aminoglycosides due to their potential nephrotoxicity and ototoxicity.
Mader et al. present an instructional course lecture reviewing common antibiotics and their mechanisms of action. For aminoglycosides, they comment that their primary use is for aerobic Gram-negative organisms, particularly enterobacter species and P. aeruginosa. Aminoglycosides have realtively poor activity against Gram-positive organisms and should not be used for staph or strep species.
Illustration A is a diagram showing the mechanism of action of different antibiotics. Incorrect Answers:
Question 43
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?
Explanation
REFERENCES: Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Garfin SR, Vaccaro AR(eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 235-256.
Question 44
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Explanation
Question 45
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
Explanation
REFERENCES: Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Timins ME: MR imaging of the foot and ankle. Foot Ankle Clin 2000;5:83-101.
Question 46
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
REFERENCES: Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997;5:67-78.
Schwend RM, Hennrikus W, Hall JE, et al: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Question 47
A patient undergoes the procedure shown in Figure A. This patient is most likely to be Review Topic
Explanation
In the pediatric population, arthroereisis is one option to restore the alignment of the hindfoot after talocalcaneal coalition. Hindfoot deformity correction is required because resection of the coalition alone will often increase the hindfoot valgus
deformity. The arthroereisis implant prevents this valgus collapse. Another alternative to correct the hindfoot valgus deformity is a calcaneal lateral column lengthening osteotomy.
Khoshbin et al. reviewed the long-term outcomes of coalition resection in 24 patients (32 coalitions). Resected talocalcaneal (TC) coalitions had less inversion/eversion postoperatively than resected calcaneonavicular (CN) coalitions but there was no difference in outcome scores. They obtained favorable results when even resecting talocalcaneal coalition with >50% involvement of the middle facet and hindfoot valgus angles >16 °, which were considered historical contraindications to resection.
Zaw et al. reviewed tarsal coalitions. Radiographic signs of CN coalition include the anteater sign (elongated anterior calcaneal process), decreased CN gap, reverse anteater sign (elongated lateral navicular) and hypoplastic lateral talar head. Radiographic signs of TC coalition include obliterated middle facet on a Harris view (osseous coalition), irregular cortices/dysplastic sustentaculum tali on a Harris view (nonosseous), C-sign on a lateral view, talar beaking, short talar neck with concave inferior surface, narrow posterior facet, and non-visibility of the middle facet.
Giannini et al. reviewed subtalar arthroereisis with coalition resection in 14 feet in patients aged 9-18 years. They achieved 57% excellent, 21% good and 21% fair results. Regarding pain, 86% had improvement and 14% had no change. Regarding ROM, 93% had improvement, and 7% had no change. Better scores were seen in patients <14 years.
Figure A shows the implantation of an arthroereisis implant in the sinus tarsi. Illustration A comprises coronal CT images of talocalcaneal coalition.
Incorrect Answers:
Question 48
82 • American Academy of Orthopaedic Surgeons A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 49
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of

Explanation
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an infection, and revascularization is not indicated.
Question 50
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
REFERENCES: Jessing P: Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-609.
Stein F, Grabias SL, Deffer PA: Nerve injuries complicating Monteggia lesions. J Bone Joint Surg Am 1971;53:1432-1436.
Question 51
The CT scan reveals a nondisplaced greater trochanteric fracture. The patient is now experiencing severe pain. What is the most appropriate treatment at this time?
Explanation
This patient presents with significant polyethylene wear, which can lead to both osteolysis and synovitis. However, synovitis usually manifests as a mild to moderate chronic ache, which should explain the discomfort. Although infection should always be ruled out with new-onset pain, no clinical parameters suggest acute hematogenous infection. Similarly, without any mention of back pain or neuropathy, radicular pain from the spine is unlikely. If this patient has a nondisplaced greater trochanteric fracture noted on MR imaging, the optimal immediate mode of treatment is to not rush into surgery despite the mild osteolysis. The patient’s severe pain is likely attributable to the nondisplaced greater trochanteric fracture rather than wear-induced synovitis, which typically presents as a mild to moderate ache. It is recommended to
allow the fracture to heal to avoid fracture displacement. Once the fracture is healed, a revision surgery with liner exchange can be recommended. Based on this clinical scenario, the acetabular component is within what is largely considered the “safe-zone” in THA. Despite this patient’s dislocations, the preferred treatment modality is to revise to a constrained liner. This patient had a well-functioning hip for longer than 15 years. Therefore, conversion to a constrained liner is the best treatment.
Question 52
The patient undergoes hip arthroscopy and the image of the right hip is shown in Figure 39. Repair of the injured structure would be expected to improve
Explanation
The radiographic studies reveal both acetabular dysplasia and cam-type femoroacetabular impingement. The MR image shows an acetabular labral tear. Structural abnormalities of the hip, including femoroacetabular impingement, have commonly been identified in association with labral tears. Disruption of the ligamentum teres is not associated with impingement conditions in the absence of trauma.
The patient has acetabular dysplasia with a decreased lateral center-edge angle and also has visible cam-type femoroacetabular impingement. The common pathway for joint degeneration in hips with cam-type femoral head anatomy includes the development of cartilage damage in the anterior or superolateral aspects of the acetabular cartilage. Paralabral cysts may be seen more commonly in association with acetabular dysplasia, although the patient’s radiographs did not demonstrate substantial cystic changes. Osteochondral loose bodies and ligamentum teres ruptures can be seen at arthroscopy in a small number of cases.
There are several proposed roles of the acetabular labrum. It can increase the depth of the acetabular socket by as much as 21% to 28%. Roles of the acetabular labrum include joint lubrication, shock absorption, and pressure distribution. Recent studies assessing the effects of loading on joint stability for both normal and dysplastic hips did not demonstrate a substantial role of the labrum in differences in loading. Although joint stability might be improved following surgical repair, acetabular dysplasia is not likely to be resolved with acetabular labral repair alone.
RECOMMENDED READINGS
Tibor LM, Leunig M. The pathoanatomy and arthroscopic management of femoroacetabular impingement. Bone Joint Res. 2012 Oct 1;1(10):245-57. doi: 10.1302/2046-3758.110.2000105.PubMed: 23610655. View Abstract at PubMed
Peelle MW, Della Rocca GJ, Maloney WJ, Curry MC, Clohisy JC. Acetabular and femoral radiographic abnormalities associated with labral tears. Clin Orthop Relat Res. 2005 Dec;441:327-33. PubMed PMID: 16331022. View Abstract at PubMed
Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011 Jul;39 Suppl:72S-8S. doi: 10.1177/0363546511412320.
PubMed PMID: 21709035. View Abstract at PubMed
James SL, Ali K, Malara F, Young D, O'Donnell J, Connell DA. MRI findings of 37
femoroacetabular impingement. AJR Am J Roentgenol. 2006 Dec;187(6):1412-9. PubMed PMID: 17114529. View Abstract at PubMed
Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17. doi: 10.1007/s12178-009-9052-9. Epub 2009 Apr 7. PubMed PMID: 19468871. View Abstract at PubMed
Henak CR, Ellis BJ, Harris MD, Anderson AE, Peters CL, Weiss JA. Role of the acetabular labrum in load support across the hip joint. J Biomech. 2011 Aug 11;44(12):2201-6. doi: 10.1016/j.jbiomech.2011.06.011. Epub 2011 Jul 14. PubMed PMID: 21757198. View Abstract at PubMed
Question 53
A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck fracture. Along with surgical fixation of the fracture, what is the next step in management? Review Topic
Explanation
Question 54
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
REFERENCES: Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Katlic MR, Derkac WM, Coleman WS: Clostridium septicum infection and malignancy. Ann Surg 1981;193:361-364.
Question 55
Figures 37a and 37b show the clinical photographs of a 43-year-old patient with type I diabetes mellitus who has a stump ulcer after undergoing successful transtibial amputation 1 year ago. Which of the following is considered the most predictable method of healing the ulcer and preventing recurrent ulceration?
Explanation
REFERENCE: Hadden W, Marks R, Murdoch G, et al: Wedge resection of amputation stumps: A valuable salvage procedure. J Bone Joint Surg Br 1987;69:306-308.
Question 56
A 13-year-old pitcher is hit in the left intercostal space by a line drive ball. He collapses, is apneic and unresponsive, and his radial pulse is absent. What is the next step in management? Review Topic
Explanation
Question 57
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?

Explanation
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Which treatment option listed is best for each patient described?
71A

B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Question 58
As a baseball player dives to catch a line drive in the outfield, the ball strikes the tip of the player’s finger when extended, causing forcible flexion to avulse the extensor tendon from the distal phalanx. Following evaluation and normal radiographic findings, initial management should include
Explanation
6 weeks, followed by nighttime splinting for an additional 6 weeks. It must be emphasized to the patient that at no time during the initial 6 weeks of treatment should the DIP joint be allowed to fall into flexion or an additional 6 weeks of continuous splinting is required.
REFERENCES: Miller MD, Cooper DE, Warner JP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 255.
Rettig AC: Closed tendon injuries of the hand and wrist in the athlete. Clin Sports Med 1992;11:77-99.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 229-230.
Question 59
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
REFERENCE: Ditunno JF, Little JW, Tessler A, et al: Spinal shock revisited: A four-phase model. Spinal Cord 2004;42:383-395.
Question 60
Figures 1 through 3 show the radiographs obtained from a 40-year-old woman who injured her right index finger in a bicycle collision. Failure to restore sagittal plane alignment would likely result in

Explanation
The radiographs reveal an extra-articular proximal phalanx fracture of the index finger. The fracture is comminuted with dorsal angulation of the distal fragment. The question specifically asks about the restoration of sagittal alignment. The fracture is comminuted with dorsal angulation of the distal fragment. The other options are incorrect, because overlapping of the digits occurs with rotational malalignment, the development of arthritis may occur with intra-articular fractures, and hyperextension would not occur with this type of deformity.
Question 61
A surgeon performs a minimally invasive total knee arthroplasty through a quadriceps-sparing approach using medial-to-lateral cutting jigs. When beginning therapy that afternoon, the patient can passively but not actively extend her knee, although she has minimal knee pain. All regional blocks have been discontinued. What is the most likely reason for this finding?
Explanation
This patient lacks active knee extension. It is not attributable to the regional block because that block is no longer acting. The most likely cause is laceration of the patella tendon, which has been described during both large-incision surgery and minimally invasive surgery. However, this is reported with increased frequency during minimally invasive surgery. Quadriceps inhibition, avulsion of the quadriceps tendon, and femoral nerve palsy can cause lack of active extension, but these problems are less likely because the patient has minimal pain.
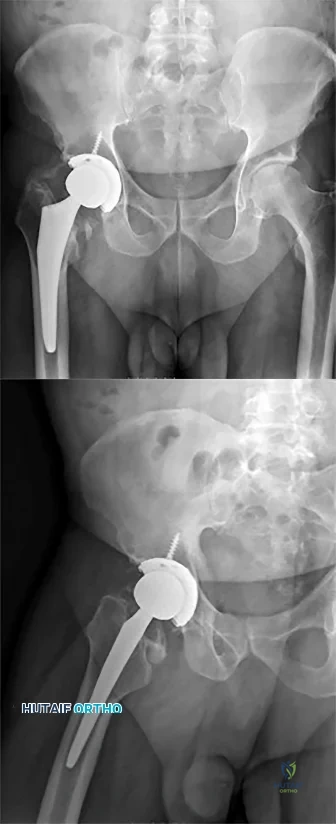
Question 62
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
Question 63
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
REFERENCE: Leffert RD: Anatomy of the Brachial Plexus in Brachial Plexus Injuries. Churchill Livingstone, New York, NY, 1985.
Question 64
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity. Postoperative radiographs are shown in Figures 3 and 4. How does the plate function?

Explanation
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 65
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
REFERENCES: Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Sharrard J, Drennan JC: Osteotomy excision of the spine for lumbar kyphosis in older children with myelomeningocele. J Bone Joint Surg Br 1972;54:50-60.
Question 66
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
REFERENCES: Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Keaveny TM: Strength of trabecular bone, in Cowin SC (ed): Bone Mechanics Handbook. Boca Raton, FL, CRC Press, 2001, pp 16-1-16-8.
Question 67
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?
Explanation
REFERENCES: Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Hettrich CM, Weldon E III, Boorman RS, et al: Preoperative factors associated with improvements in shoulder function after humeral hemiarthroplasty. J Bone Joint Surg Am 2004;86:1446-1451.
Question 68
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 69
Sex-linked recessive Pseudohypoparathyroidism (AHO) - end-organ insensitivity; in AHO, germline mutation that leads to loss of function of Galpha S (GNAS1); causes end-organ resistance to PTH
Explanation
Question 70
..A 75-year-old woman sustained a 4-part fracture dislocation of the proximal humerus with a comminuted humeral head. You decide to perform a reverse total shoulder replacement because of her age and activity level. This will be your first reverse total shoulder replacement. It is common practice in your hospital for an industry representative to be present when new implants are brought into the operating room. What information are you required to disclose?
Explanation
Arthroscopic or open debridement and capsular release
Interposition arthroplasty
Ulnohumeral arthrodesis
Linked total elbow arthroplasty (TEA)
Unlinked TEA
What surgical procedure listed above is most associated with the conditions defined below?
Question 71
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 72
Chemotherapy is routinely included in the treatment of which of the following soft-tissue sarcomas?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Rhabdomyosarcoma, in Soft Tissue Tumors, ed 3. St Louis, MO, CV Mosby, 1995, p 539.
Hays DM: Rhabdomyosarcoma. Clin Orthop 1993;289:36-49.
Question 73
What is the average version of the humeral head (with respect to the transepicondylar axis)? Review Topic
Explanation
One of the goals of primary anatomic total shoulder arthroplasty (TSA) is recreation and reconstruction of proximal humeral anatomy. Modular prostheses have evolved to provide surgeons with better capability to recreate proximal humeral morphology based on humeral head inclination, retroversion, offset, height and size. In terms of size, humeral head thickness has been found in cadaver studies to be 70% of its radius of curvature. This can be helpful to avoid 'over-stuffing' the joint or leaving it too loose.
Boileau and Walch took digitized measurements of 65 humeri in order to create a computer model for proximal humeral morphology. They found that retroversion varied from -6.7 to 47.5 degrees, with a mean of 17.9. They advocate for prosthetic adaptability to recreate proximal humeral anatomy in a way that earlier generations of more geometrically constrained TSA implants could not.
Robertson et al. made 3D computed tomographic models of 60 humeri (30 pairs) to study proximal humeral morphology. They found mean retroversion to be 19 degrees, with a range of 9 to 31 degrees. They found that proximal canal version was similar to head version but that canal version in the middle and distal sections of the canal was variable.
Illustration A shows key proximal humeral morphologic parameters found by Robertson et al. in comparison with earlier studies (including Boileau's).
Incorrect Answers:
Question 74
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 75
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
REFERENCES: Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Gertzbein SD: Metastatic spine tumors, in Herkowitz HN, Dvorak J, Bell G, et al (eds): The Lumbar Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 792-802.
Question 76
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability.
REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.
Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 77
Posttraumatic physeal arrest is most common at which of the following locations?
Explanation
REFERENCES: Ecklund K, Jaramillo D: Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol 2002; 178:967-972.
YAtotoartanadQpyiQter GN: Physeal bridge resection. J Am Acad Orthop Surg 2005; 13:4
Figure 64a Figure 64b
Question 78
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 79
The ability of compressed cortical bone to resist greater applied force in the longitudinal plane than in the transverse plane is an illustration of what material property?
Explanation
Question 80
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?
Explanation
L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root.
REFERENCES: Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Aeschbach A, Mekhail NA: Common nerve blocks in chronic pain management. Anesthesiol Clin North Am 2000;18:429-459.
Question 81
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
REFERENCES: Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
Guskiewicz KM, McCrea, Marshall SW, et al: Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA
2003;290:2549-2555.
Question 82
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
is best reserved for low-demand or infirm patients.
Question 83
The function of which of the following structures is to resist internal tibial rotation with the knee in full extension? Review Topic
Explanation
The posterior oblique ligament is a structure within the posteromedial corner of the knee, with attachments proximally to the adductor tubercle of the femur and distally to the tibia/posterior knee capsule. The posterior oblique ligament and posteromedial capsule play a significant role in the prevention of additional posterior tibial translation in the knee in the setting of posterior cruciate ligament injury. They also act to resist internal tibial rotation with the knee in full extension.
Griffith et al. reports that the posterior oblique ligament provides significant resistance to valgus and internal rotation forces with knee extension. They used a cadaver model and demonstrated that the superficial MCL resists valgus and external rotation forces more than the posterior oblique ligament, while the posterior oblique ligament is more involved in resisting internal rotation.
Tibor et al. reviews the anatomy of the posteromedial corner of the knee. They report that failing to recognize injury to these structures may cause failure of cruciate ligament reconstruction surgery, and that reconstruction or repair of the posteromedial corner may be indicated in the face of multiple ligament injuries.
Illustration A shows the posteromedial corner of the knee, including the posterior oblique ligament.
Incorrect answers:
1-4: These structures are not primary restraints to internal tibial rotation in full extension.
Question 84
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 85
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
Explanation
REFERENCES: Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Kelly JP, Rosenberg JH: Diagnosis and management of concussion in sports. Neurology 1997;48:575-580.
Question 86
A 32-year-old female sustained the injury seen in Figure A after a motor vehicle accident. On physical exam there was obvious deformity about the arm with a laceration that probed to bone over the lateral aspect of the arm. The patient was neurovascularly intact. She was treated with an intramedullary nail. Which of the following is true?

Explanation
Options for operative management of humeral shaft fractures mainly consist of intramedullary nail or plate and screw constructs. The main advantage to intramedullary nailing is when the soft tissue envelope makes a large incision undesireable or the fracture pattern dictates a relative stability construct - such as segmental or massively comminuted injuries. The disadvantages include trauma to the rotator cuff, post operative shoulder pain, indirect reduction leading to increased risk of malrotation, and increased reoperation for implant removal.
Li et al. performed a randomized controlled trial with 45 patients that investigated the difference in post operative malrotation and functional outcomes when comparing intramedullary nails versus open reduction and internal fixation. They concluded that
when comparing the two operative options, patients who underwent intramedullary nailing had a greater degree of malrotation, which was associated with decreased range of motion. Additionally, they found lower functional scores with patients who underwent intramedullary nailing.
Kurup et al. performed a systematic review comparing outcomes between compression plating and intrameduallary nailing for operative treatment of humeral shaft fractures. With a total of 260 patients, they found no difference with blood loss, fracture union, iatrogenic radial nerve palsy, iatrogenic fracture comminution, elbow impingement, return to pre-injury occupation, and functional shoulder scores. They did show a statistically significant increase in shoulder impingement and reduction of range of motion when using an intramedullary nail.
Figure A is a AP radiograph of a comminuted humeral shaft fracture. Illustration A is a radiograph of a humerus fixed with an intramedullary nail. Illustration B is a radiograph of a humerus fixed with a compression plate.
Incorrect Answers:
Question 87
- A 20-year-old college football player sustains a forceful hyperextension injury to his shoulder 4 months after undergoing an anterior capsular shift. Examination 2 weeks later reveals anterior tenderness. He is unable to lift the dorsum of his hand away from his back. What is the most likely diagnosis?
Explanation
Question 88
- The Injury Severity Score (ISS), using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by
Explanation
Question 89
5 degrees medial and 10 degrees cephalad
Explanation
Question 90
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?
Explanation
REFERENCE: Norris TR: Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, p 342.
Question 91
- Which of the following rehabilitation methods should be used for the first 24 hours following a blunt injury to the quadriceps musculature to avoid short-term stiffness?
Explanation
In the past immobilization in full extension was recommended, but it was noticed that the lack of flexion prolonged disability. Flexion of the knee during the first 24 hours also aids in limiting the extent of intramuscular hematoma.
Myositis ossificans is higher in any patient presenting after a quad contusion and has active knee ROM of less than 120 degrees and delay in treatment greater than 3 days.
Question 92
The flexor hallucis longus tendon is at greatest risk of injury with a lateral-to-medial drill or screw during fixation of what structure?

Explanation
Question 93
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
REFERENCES: Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 94
A funnel plot is used in meta-analyses to perform which of the following functions:
Explanation
Publication bias occurs because studies with a non-significant result, so-called
negative studies, have a higher likelihood of being rejected than positive studies, and are oftentimes not even submitted for publication. Funnel plots, which plot the effect size of a study against a measure of the study’s size are used to detect this bias. This method is based on the fact that larger studies have smaller variability, whereas small studies, which are more numerous, have larger variability. Thus the plot of a sample of studies without publication bias will produce a symmetrical, inverted-funnel shaped scatter, whereas a biased sample will result in a skewed plot.
Vavken et al. reviewed orthopaedic meta-analyses in order to determine whether publication bias was assessed and to evaluate its effect on the outcomes of these meta-analyses. They found that only 35% of all orthopaedic meta-analyses published between 1992 and 2008 in English and German assessed publication bias. Adjustment for publication bias did not produce significantly different results, but the magnitude of the pooled estimates in the affected meta-analyses changed by 29% on average.
Illustration A depicts a symmetrical funnel plot with no evidence for publication bias. Illustration B shows a skewed funnel plot suggesting publication bias, as it is missing studies in the lower left corner, i.e. ‘‘negative studies’’. Illustration C depicts a forest plot comparing the incidence of squeaking between ceramic-on-ceramic (COC) and ceramic-on-polyethylene (COP). Illustration D is an example of a ROC curve examining the probability of DVT.
Incorrect Answers:
Question 95
-Figures 56a and 56b are the MRI scans of a 2-year-old girl who has a fever of 39°C and inability to move her left arm. She has not had any recent injury and is otherwise healthy. Radiograph findings of her left upper extremity are normal. What is the most appropriate treatment?
Explanation

Question 96
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?
Explanation
REFERENCES: Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Seeger LL, Gold RH, Bassett LW, Ellman H: Shoulder impingement syndrome: MR findings in 53 shoulders. Am J Roentgenol 1988;150:343-347.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 97
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 98
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Beaule PE, Dorey FJ, Matta JM: Letournel classification of acetabular fractures: Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-1709.
Question 99
A 45-year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to 85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well- fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
Question 100
The lower extremity motor dysfunction in Charcot-Marie-Tooth disease most commonly involves which of the following muscles?
Explanation
REFERENCES: Mann RA, Missirian J: Pathophysiology of Charcot-Marie-Tooth disease. Clin Orthop 1988;234:221-228.
Tynan MC, Klenerman L, Helliwell TR, Edwards RH, Hayward M: Investigation of muscle imbalance in the leg in symptomatic forefoot pes cavus: A multidisciplinary study. Foot Ankle 1992;13:489-501.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-board-review-oite-abos-part-18