Orthopedic Surgery Board Review MCQs: Arthroplasty, Fracture, Ankle & Hip | Part 79

Key Takeaway
This page features Part 79 of an interactive Orthopedic Surgery Board Review MCQ set, authored by Dr. Mohammed Hutaif. It provides 100 verified, high-yield questions in OITE/AAOS format, designed for orthopedic surgeons and residents preparing for their AAOS/ABOS certification exams. Utilize Study or Exam modes to master topics like Ankle, Arthroplasty, Fracture, and Hip for comprehensive board prep.
About This Board Review Set
This is Part 79 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 79
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Hip.
Sample Questions from This Set
Sample Question 1: A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?...
Sample Question 2: An open biopsy specimen of a radiodense distal clavicle lesion in a 12-year-old girl shows chronic polyclonal inflammatory cells without granuloma formation. Laboratory studies show that bacterial, fungal, and acid-fast bacillus cultures ar...
Sample Question 3: Which of the following findings best describes the acetabular fracture shown in Figure 38?...
Sample Question 4: Porous hydroxyapatite is placed into a bone defect. Incorporation of this bone graft substitute is expected to follow which of the following patterns?...
Sample Question 5: -A patient who had previously undergone a salvage pelvic (Chiari) osteotomy now requires a total hip arthroplasty. The most frequent complication of this procedure is...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 2
An open biopsy specimen of a radiodense distal clavicle lesion in a 12-year-old girl shows chronic polyclonal inflammatory cells without granuloma formation. Laboratory studies show that bacterial, fungal, and acid-fast bacillus cultures are negative. Subsequently, a similar lesion is noted in the fibula. The next most appropriate step in management should consist of
Explanation
REFERENCE: Carr AJ, Cole WG, Roberton DM, Chow CW: Chronic multifocal osteomyelitis. J Bone Joint Surg Br 1993;75:582-591.
Question 3
Which of the following findings best describes the acetabular fracture shown in Figure 38?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.
Question 4
Porous hydroxyapatite is placed into a bone defect. Incorporation of this bone graft substitute is expected to follow which of the following patterns?
Explanation
Question 5
- A patient who had previously undergone a salvage pelvic (Chiari) osteotomy now requires a total hip arthroplasty. The most frequent complication of this procedure is
Explanation
Question 6
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of

Explanation
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
Question 7
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb’s point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?
Explanation
REFERENCES: Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.
Yeh YC, Sun WZ, Lin CP, et al: Prolonged retraction on the normal common carotid artery induced lethal stroke after cervical spine surgery. Spine 2004;29:E431-E434.
Question 8
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, p1550.
Benzel EC (ed): Spine Surgery Techniques, Complication Avoidance and Management. New York, NY, Churchill Livingstone, 1999, p 190.
Question 9
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
REFERENCES: Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Maron BJ, Thompson PD, Puffer JC, McGrew CA: Cardiovascular preparticipation screening of competitive athletes: A statement for health professionals from the Sudden Death Committee (Clinical Cardiology) and Congenital Cardiac Defects Committee (Cardiovascular Disease in the Young), American Heart Association. Circulation 1996;94:850-856.
Question 10
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
REFERENCES: Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
Greis PE, Scuderi MG, Mohr A, et al: Glenohumeral articular contact areas and pressures following labral and osseous injury to the anteroinferior quadrant of the glenoid. J Shoulder Elbow Surg 2002;11:442-451.
Question 11
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must
Explanation
least 1 year.
REFERENCES: Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112.
Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am
1991;73:1561-1566.
Butler MS, Brumback RJ: Interlocking nailing for ipsilateral fractures of the femur, femoral shaft, and distal part of the femur. J Bone Joint Surg Am 1991;73:1492-1502.
Question 12
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in
Explanation
REFERENCES: Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417.
D’Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Pearl ML, Bessos K, Wong K: Strength deficits related to distal biceps tendon rupture and repair: A case report. Am J Sports Med 1998;26:295-296.
Question 13
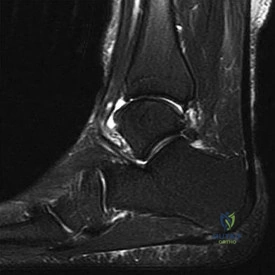
Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has localizable tenderness over the plantar medial tubercle of the calcaneus. The Achilles is intact and nontender, and subtalar joint motion is full and painless. A Tinel test result is negative. What is the most likely diagnosis?
Explanation
Plantar fasciitis is inflammation of the plantar fascia at its insertion onto the medial calcaneus. The T2-weighted sagittal MR image reveals thickening of the plantar fascia with no evidence of a calcaneal stress fracture, coalition, or inflammation of the insertion of the Achilles tendon.
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
Question 14
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?
Explanation
REFERENCE: Gerber C, Myer DC, Schneeberger AG, et al: Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J Bone Joint Surg Am 2004;86:1973-1982.
Question 15
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
REFERENCES: Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119.
Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362.
Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
McKellup HA: Bearing surfaces in total hip replacement: State of the art and future developments. Instr Course Lect 2001;50:165-179.
Question 16
A 70-year-old man with primary osteoarthritis undergoes a primary cementless total hip arthroplasty (THA). His history includes pelvis irradiation for prostate carcinoma (6000 rads). He is at increased risk for which complication?
Explanation
The complication associated with pelvic radiation prior to cementless THA is loosening of the acetabular component or postsurgical noningrowth of the component. Although scarring from radiation may put the hip at increased risk for arterial or nerve damage or infection, this risk has not been associated with pelvic radiation. Cementless acetabular components with porous metal surfaces such as trabecular metal should be considered.
Question 17
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?
Explanation
REFERENCE: Gardner MJ, Brophy RH, Demetrakopoulos D, et al: Interventions to improve osteoporosis treatment following hip fracture: A prospective, randomized trial. J Bone Joint Surg Am 2005;87:3-7.
Question 18
They used three outcome tools, SF-36, WOMAC, and Modified Boston Children's Hospital Grading System to evaluate the the two groups at a minimum of 2 years from injury. The foot injury group, including all types of foot fractures, had a poor outcome when using any of these measures. Turchin concludes that “Foot injuries cause significant disability to multiply injured patients. More attention should be given to these injuries, and more
Explanation
Excessive bleeding into joints and muscles is a common manifestation of hemophilia. The iliacus muscle is a frequent site of hemorrhage in patients with severe or moderate hemophilia. Intramuscular hematoma of the iliacus muscle is likely to occur following play or sporting events that include forceful contraction of the hip flexor muscles. As the hematoma expands, it may
compress the adjacent femoral nerve, potentially resulting in complete femoral nerve palsy. Femoral nerve compression typically includes paresthesias in the distribution of the terminal saphenous nerve branch.
Gilbert et al. review the complex relationship between recurrent bleeding, synovitis, and the development of arthritis in the patient with hemophilia. They discuss both conservative and surgical treatment modalities in these patients and recommend arthroscopic synovectomy for the knee and ankle joints. They conclude that the greatest risk to these procedures is a decreased range of motion.
Kuo et al. reports on a fourteen-year-old healthy boy with an 11-day history of pain and weakness in the right lower limb following a fall. They report pain in the right lower extremity, numbness of the anterior aspect of the right thigh and medial border of the right leg and foot, inability to ambulate and
weakened quadriceps muscle strength. MRI revealed an iliacus hematoma with a complete femoral nerve palsy. He underwent CT-guided percutaneous drainage for decompression with complete resolution of the palsy.
Illustration A is a diagram of dermatomal distribution. Illustration B shows the lumbar plexus demonstrating the intimate relationship of the femoral nerve to the iliacus muscle.
Incorrect Answers:
A 45-year-old male trauma patient presents with multiple extremity injuries including the foot injury shown in Figure A. The foot fracture is treated surgically, and heals without any initial complications. At a minimum of 12 months, this patient will be expected to have which of the following scores compared to a
Patients with pauciarticular juvenile rheumatoid arthritis (JRA), specifically the subgroup with elevated antinuclear antibody (ANA) titers, are associated with the highest incidence (~75%) of anterior uveitis. As a result, referral for an ophthalmology consultation is recommended.
Pauciarticular JRA is the most common subgroup of JRA and typically presents between the ages of 2 to 4 years with mild swelling of one to four joints. The diagnosis is typically one of exclusion as laboratory studies, including erythrocyte sedimentation rate and rheumatoid factor, are usually within normal limits. In JRA, iridocyclitis, a type of anterior uveitis typically occurs following the onset of synovitis but may precede the joint symptoms. This iridocyclitis is frequently indolent but requires immediate ophthalmologic consultation for a slit-lamp examination because if left untreated, anterior uveitis may progress to loss of vision.
Foeldavri et al. review JRA anterior uveitis. They report an overall incidence of
10%, but this is dependent on the JRA subtype. They noted that a large proportion of children with JRA develop uveitis in the first year of disease and
90% after 4 years. They state that early age of JRA onset, oligoarticular subtype, and ANA reactivity are the main risk factors for the development of uveitis. They conclude that JRA-associated uveitis is important to recognize and treat early to prevent any visual damage.
Hawkins et al. review bilateral chronic anterior uveitis in JRA. They report that female gender, oligoarthritis, and presence of antinuclear antibodies are risk factors.
They report on treatment options, including the use of biologics. They conclude that stepwise immunomodulatory therapy is indicated, with new biologic drugs being used in cases of refractory uveitis.
Incorrect Answers:
Anterior 4: Pompe disease is a glycogen storage disease which may lead to ptosis (drooping of the upper eyelid), not anterior uveitis
A 9-year-old male with hemophilia A presents with severe groin pain, parasthesias over the medial aspect of the distal tibia, and difficulty ambulating several hours after a soccer game. He is believed to have an intramuscular hematoma surrounding the iliacus muscle. Which nerve is MOST likely to be compressed?
Which of the following conditions places the patient at highest risk for anterior uveitis and necessitates referral to an ophthalmologist?
Salmonella is a classic cause of osteomyelitis in patients with sickle cell disease.
Sickle cell disease is a genetic disorder of hemoglobin synthesis. The disease occurs in two phenotypes: sickle cell anemia (most severe) and sickle cell trait (most common). The two most common causes of osteomyelitis in children with sickle cell disease are
Staphylococcus aureus and Salmonella. Although S. aureus is the most common cause of osteomyelitis in the general population, the literature varies on which is the most common in patients with sickle cell disease. The increased risk in these patients may be associated with gastrointestinal microinfarcts, poor circulation of blood in bone, and splenic infarcts that predispose patients to infection by encapsulated bacteria (i.e., Salmonella).
Piehl et al. analyzed records of seven hundred seventeen patients with sickle cell disease treated over a thirteen-year period. They identified and retrospectively reviewed sixteen cases of osteomyelitis in fifteen patients. The authors found Salmonella to be the causative organism in thirteen cases with Proteus mirabilis, Escherichia coli, and Staphylococcus aureus all affecting one patient each. The authors report the annual incidence of osteomyelitis in their series as 0.36%.
Givner et al. reviewed sixty-eight cases of osteomyelitis in children with sickle cell disease and positive cultures over a ten year period. Of the sixty-eight, 50 (75%) yielded Salmonella and Staphylococci was isolated 7 (10%). In
addition, the authors report non-speciated gram-positive cocci were isolated in
11 (16%), non-speciated gram-negative rods in 5 (7%), and non-specified bacteria in 2 (3%). The authors conclude Salmonella is the most common pathogen causing osteomyelitis in patients with major sickle hemoglobinopathies.
Epps et al. reviewed fifteen patients with sickle cell disease and osteomyelitis. Staphylococcus aureus was isolated in eight cases (53%), Salmonella in six (40%), and Proteus mirabilis in one (7%). The authors conclude S. aureus, not Salmonella, may be the most common cause of osteomyelitis associated in patients with sickle-cell disease.
Figure A demonstrates an osteolytic lesion of the distal tibia and Figure F demonstrates sickle-shaped erythrocytes.
Incorrect Answers
Low toughness is a disadvantage of ceramic bearings in total hip arthroplasty.
Ceramic is a non-metal that demonstrates excellent wear characteristics when used with polyethylene in total hip arthroplasty. Although it has a high Young's modulus, it has a low fracture toughness. Subsequently, ceramic is poorly resistant to crack formation. In contrast, UHMWPE has a high fracture toughness because of the presence of very long hydrocarbon chains.
Santavirta et al. review alternative bearing materials to improve wear in total hip arthroplasty. Alumina ceramics are noted to be biostable and bioinert. The best wear properties are noted with ceramic-on-ceramic bearings. For current ceramic constructs, fracture risk is less than 1 per 1000.
Lang et al. review the use of ceramics in total hip replacement. The authors note that ceramic has high compressive strength and high wettability. Low fracture toughness and linear elastic behavior increase the risk of breakage of ceramic components under stress. Processing improvements, enhanced head- neck interfaces and liner modifications have lead to a decrease in the rate of ceramic fracture.
Illustration A shows a compromised ceramic head as a manifestation of the low fracture toughness of the material.
Incorrect Answers:
An 8-year-old African American female presents with lower extremity pain and subjective fever. On exam there is tenderness about the distal tibia. Further workup reveals elevated inflammatory markers and a lytic lesion (Figure A). An aspirate is obtained and cultures grow Salmonella. Additional investigation is most likely to reveal which of the following findings (Figure B-F)?
An ideal fluid film lubrication regime minimizes friction. A larger head size results in a greater development of full-film lubrication due to the increased relative sliding velocity of the larger bearing surfaces. Increased surface roughness inhibits the formation of the film lubrication. The most important factor influencing the predicted lubrication film thickness
has been found to be the radial clearance between the ball and the socket.
Jin et al report that slight clearance, not complete congruence, is optimal for formation of the optimal fluid film lubrication. They note that full fluid film lubrication may be achieved in these hard/hard bearings provided that the surface finish of the bearing surface and the radial clearance are chosen correctly and maintained.
Dumbleton reviewed the literature of metal-on-metal THA and concluded that the current literature does not show any clinical benefit of metal-on-metal compared to metal on poly. Metal-on-metal has been shown to have higher metal ion level in blood, and measurement of these levels is recommended to help identify those at risk of adverse effects from metal on metal prostheses.
Low toughness is a disadvantage of which of the following bearing surfaces used in total hip arthroplasty?
This attending did not fully disclose that the resident would be performing the cementing portions of the case unsupervised. This represents an ethically unsound scenario as the patient was misled regarding involvement of the resident in their surgery.
The informed consent process is grounded in the ethical principle of autonomy. Informed consent represents a shared decision making process where a
patient understands all the risks and benefits of a surgery fully and makes an informed decision. However, the patient's choice of surgeon is felt to be critical
to the informed consent process and any variation from that surgeon performing the surgery should be discussed explicitly. A surgeon who performs surgery or part of surgery on the patient without prior consent may be held liable for battery.
Kocher presents three cases demonstrating the spectrum of "ghost surgery". They state the substitution of an authorized surgeon with an unauthorized surgeon or allowing surgical trainees to operate without appropriate guidance constitutes "ghost surgery".
Deviation from what is explicitly discussed has been justified in an emergency scenario or if the treatment is aimed at an overall condition.
Bhattacharyya et al reviewed malpractice claims for factors that positively correlated with successful defense. They found that those who performed informed consent in the office had lower risk of malpractice payment. They conclude surgeons can decrease their risk of malpractice claims by performing informed consent in the office and documenting the discussion.
Incorrect Answers:
Which of the following features of metal-on-metal total hip arthroplasty does not allow for improved fluid film lubrication between the components?
The patient sustained a fragility fracture with lab work consistent with primary hyperparathyroidism.
Hyperparathyroidism is commonly caused by increased activity of the parathyroid glands resulting in high levels of PTH. Increased circulating levels of PTH leads to calcium being "sucked" out of bone and into the serum. This
alteration in calcium hemostasis leads to low-density bone and a predisposition to fragility type fractures. When present, lab values are much different from standard age-related osteoporosis. Furthermore, referral to medical and surgical endocrinology specialists for directed treatments may improve overall bone quality and prevent further fragility fractures.
Fraser summarizes primary and secondary hyperparathyroidism. He describes the normal physiologic response to low calcium of an increase in PTH. Increased PTH has three downstream effects of increased tubular resorption of calcium by the kidneys, increased osteoclast activity to harvest calcium from bone, and increased active vitamin D levels leading to increased bowel absorption of calcium.
Singhal et al. reviewed hyperparathyroidism and what the orthopedic surgeon should know. They state when a patient presents with a pathologic fracture and elevated serum calcium levels, an appropriate lab workup for hyperparathyroidism should be done. They stated when surgery is needed for hyperparathyroidism and fracture, surgery can safely be performed simultaneously as demonstrated by 3 case examples.
Figure A exhibits a left femoral neck fracture, which is a fragility fracture associated with poor bone density. Illustration A is a figure from Fraser's article exhibiting the
feedback loop from the hypothalamus, pituitary, adrenal/glandular axis.
Incorrect answers:
Prior to undergoing a total knee arthroplasty at an academic medical center a patient is told during informed consent by the attending surgeon that resident involvement in the case will be limited to retracting. During the case the attending is present up to trialing of the selected components. The surgeon leaves prior to cementing to start trialing components in another case while the chief resident remains alone in the room for the completion of the case. Which of the following is true regarding the ethics of this practice?
Patients in factorial randomized control trials (RCT) are assigned to groups that receive a specific combination of interventions and non-interventions.
In factorial RCTs, patients are randomized to groups receiving treatment A and B, treatment A or control, treatment B or control, or no treatment. This study design is useful because two interventions can be assessed with the same
study population and any interaction between the treatments can be determined (for example, does treatment A work differentially when combined with treatment B). Other randomized control trial designs include parallel, cluster, and crossover. Parallel studies are performed by having two or more groups that exclusively have one intervention without group overlap.
Crossover studies have each group receive each intervention in a random sequence. Cluster design studies have pre-existing groups of participants
(such as schools, or cities) that are randomly selected to receive or not receive an intervention.
Karlsson and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine published an exhaustive guide to research for evidence-based medicine in a step-wise fashion. They cover levels of evidence, design for randomized control trials and the CONSORT checklist. They also describe proper study design of cohort, case- control, case series, systematic review, meta-analysis studies. The second half of the guide discusses appropriate outcome measures, statistical analyses, and data interpretation, reporting complications, and concludes with steps to writing a scientific article.
Incorrect Answers:
A 66-year-old woman falls from standing and sustains the injury shown in Figure A. Her most recent T score was -1.9, 3 months prior to presentation. Preoperative lab work reveals elevated serum calcium, elevated alkaline phosphatase, decreased serum phosphorus, and elevated parathyroid hormone (PTH). Which of the following correctly describes the underlying etiology of her osteopenia?
The most recent update of the CDC guidelines for the prevention of SSI issues a category IA strong recommendation stating that "in clean and clean- contaminated procedures, do not administer additional antimicrobial prophylaxis doses after the surgical incision is closed in the operating room, even in the presence of a drain."
The previous 2002 CDC guidelines for the prevention of SSI focused on three performance parameters: (1) initiation of parenteral antibiotics within 1 hour of the surgical incision, (2) selection of an appropriate antibiotic, and (3) discontinuation of antibiotics within 24 hours. The most recent updated 2017
CDC guidelines for the prevention of SSI has several notable changes with an emphasis that additional doses of antibiotics after initial prophylaxis are no longer recommended.
Berrios-Torres et al. review the 2017 updates to the CDC guidelines for prophylaxis against SSI. Strong recommendations include that in clean and clean-contaminated cases, additional antimicrobial prophylaxis should not be administered after the surgical incision is closed in the operating room, even in the presence of a drain. Furthermore, the authors discuss that there is no evidence that re-dosing intraoperative antibiotics or continuation of antibiotics until surgical drains have been removed provides any additional protection against surgical site infection.
O'Hara et al. highlights the key updates in the most recent CDC guidelines for prevention of SSI. The authors present specific suggestions for translating these recommendations into evidence-based policies and practices. They conclude that the implementation of new and existing guidelines in SSI prevention requires thoughtful and careful collaboration with several inter- professional and interdisciplinary teams.
Incorrect Answers:
Which of the following study designs describes a randomized controlled trial in which two interventions are applied separately or in combination to study groups?
The patient has an allergy to cephalosporins and a history of an MRSA infection. Of the choices listed, vancomycin is the best preoperative antibiotic for this patient.
The choice of preoperative antibiotics is of great interest given the large
medical and economic cost of periprosthetic infections. Standard preoperative prophylaxis in patients undergoing total joint arthroplasty consists of cefazolin or cefuroxime. In patients with beta-lactam allergies, the treatment options include clindamycin or vancomycin. Vancomycin is often the antibiotic of choice given it's higher efficacy with regard to MRSA prevention. In those patients who are considered at risk for MRSA infection and a beta-lactam allergy, vancomycin can be supplemented with an aminoglycoside (gentamicin) or aztreonam.
Bratzler et al. review antimicrobial prophylaxis for surgery and state for orthopedic joint replacement procedures cefazolin or cefuroxime is the recommended antibiotic. For patients with a confirmed beta-lactam allergy, they recommend vancomycin or clindamycin. They also state antibiotics should be stopped within 24hrs after surgery.
Dellinger et al. review antibiotics for surgical prophylaxis. They state the standard antibiotics for orthopedic procedures are cefazolin or cefuroxime. They state if there is also a concern for MRSA infection vancomycin can be added in addition to the above antibiotics.
Incorrect Answers:
Which of the following is STRONGLY recommended by the most recent (2017) Centers for Disease Control and Prevention (CDC) Guidelines with regard to antimicrobial prophylaxis for the prevention of surgical site infection (SSI)?
Clindamycin is a bacterial protein synthesis inhibitor by inhibiting ribosomal translocation at the 50S subunit.
Clindamycin is primarily bacteriostatic but may be bactericidal at higher concentrations.
Side effects of clindamycin may include a hypersensitivity reaction and pseudomembranous colitis. Resistance to clindamycin is conferred by a plasmid that alters the 50s ribosome binding site for clindamycin. The D- zone test is used to determine whether an organism has inducible resistance
to clindamycin.
Marcotte and Trzeciak published a review on community-acquired methicillin- resistant Staphylococcus aureus (CA-MRSA). They reported that CA-MRSA
does not have predictable susceptibility to clindamycin. They conclude that clindamycin also presents a risk for the development of Clostridium difficile colitis and inducible clindamycin resistance for which a D-zone test should be performed when culture results reveal erythromycin resistance.
Steward et al. performed a lab study to determine the efficacy of testing for induced clindamycin resistance in erythromycin-resistant Staphylococcus aureus. They reported that resistance to erythromycin and clindamycin can occur through methylation of their ribosomal target site (50s), which is mediated by erm genes. They conclude that disk diffusion is the preferred method for testing S. aureus isolates for inducible clindamycin resistance.
Incorrect Answers:
A 68-year-old man is scheduled to undergo total hip arthroplasty. He states he had an anaphylactic reaction after taking cefazolin for an MRSA hand infection 10 years ago. Which of the following best describes the preoperative antibiotic that should be administered for this patient?
Advanced glycation end-products (AGEs) cause excessive cross-linking of collagen in aging articular cartilage. As a result, the stiffness is increased.
AGEs are produced by spontaneous nonenzymatic glycation of proteins when sugars (glucose, fructose, ribose) react with lysine or arginine residues. The most abundant matrix protein in cartilage is Type II collagen. AGEs cause changes to the aging cartilage matrix and the aging chondrocyte. The increased cross-linking of Type II collagen results in an increase in cartilage stiffness (i.e. increase in the modulus of elasticity) and an increase in brittleness (i.e. less strain needed to go from the yield point to the fracture point on the stress-strain curve). As a result of the change in the aging cartilage’s biomechanical properties, it's susceptible to fatigue failure. Additionally, AGEs decrease the anabolic response of chondrocytes from autocrine signaling via TGF-beta, IGF-1, BMP-7, and OP-1. These two initial mechanisms contribute to aging cartilage to eventually lead to the development of osteoarthritis.
Li et al. reviewed age-related changes in cartilage and seek to define the different
mechanisms between aging cartilage and osteoarthritis. They state that with AGEs, there is excessive collagen cross-linking increases cartilage stiffness, while shortening/degradation of aggrecan leads to loss of sugar side chains and water-binding ability. Additionally, increased levels of AGEs are associated with a decline in anabolic activity. They state that these changes to cartilage make it more vulnerable to damage and therefore the onset of osteoarthritis. This is contrast to the initial steps in the mechanism of osteoarthritis which is characterized by cell proliferation, formation of chondrocyte clusters, increased synthesis of irregular cartilage matrix, and eventually a pro-catabolic and pro-inflammatory state that results in an imbalance in cartilage homeostasis and cartilage matrix breakdown.
Anderson et al. reviewed the relationship between osteoarthritis and aging.
They state that knee cartilage thins with aging, especially on the femoral and patellar sides, suggesting a gradual loss of cartilage matrix. AGEs formation leads to modification of type II collagen by cross-linking of collagen molecules, increasing stiffness and brittleness and increasing susceptibility to fatigue failure. Furthermore, describe the senescent phenotype of the chondrocyte
and its similarities with osteoarthritic chondrocyte phenotype.
Incorrect Answers:
Which of the following antibiotics works by binding to the 50S ribosomal subunit?
The patient has clinical signs and symptoms of gout. Figure D would correspond to this diagnosis as it shows negatively birefringent needle-shaped monosodium urate crystals.
Gout is an idiopathic disorder of nucleic acid metabolism that leads to hyperuricemia and deposition of monosodium urate crystals, most commonly in the joints of the lower limb (knee, ankle, and classically the 1st metatarsophalangeal joint). Diagnosis can be confirmed with joint arthrocentesis revealing negatively birefringent needle-shaped crystals. Treatment of acute gout flares is generally comprised of NSAIDs and colchicine, and chronic gout is treated with allopurinol to prevent the build-up
of uric acid.
Shmerling et al. prospectively analyzed the synovial fluid test results of 100 consecutive patients undergoing diagnostic arthrocentesis. They noted that synovial fluid white blood cell count (WBC) and the percentage of polymorphonuclear cells performed well as discriminators between inflammatory and noninflammatory diseases. Given the diagnostic value of synovial WBCs, the authors concluded that ordering of chemistry studies of synovial fluid should be discouraged because they are likely to provide misleading or redundant information.
Chiodo et al. review the use of intra-articular aspiration and injections for both diagnosis and treatment of disorders of the lower extremity such as infectious arthritis, gout, pigmented villonodular synovitis (PVNS), rheumatoid arthritis, and hemophilia. The authors discuss the importance of knowledge of regional anatomy, procedural indications, and appropriate techniques for successful aspiration/injection. The authors review safe and effective aspiration and injection techniques for the lower extremity, including the hip, knee, foot, and ankle.
Figure A reveals hemosiderin stained multinucleated giant cells consistent with PVNS. Figure B is a gram stain revealing gram-positive cocci in clusters consistent with Staphylococcus aureus. Figure C reveals rhomboid-shaped, positively birefrigerant crystal consistent with calcium pyrophosphate/pseudogout. Figure D reveals negatively birefringent needle- shaped crystals of monosodium urate/gout. Figure E reveals a collection of histiocytes and inflammatory cells around prominent intimal hyperplasia.
Incorrect Answers
An increase in advanced glycation end-products (AGEs) is characteristic of which of the following clinical conditions and results in which pathologic process?
Regardless of the number of level I studies included in a systematic review, having one study with <80% follow-up decreases the level of evidence for this review from level I to level II.
After classifying the type of study (e.g. therapeutic study, prognostic study, diagnostic study, economic analysis, or decision analysis) the “level of evidence” is then determined. The level of evidence (on a scale of I through V) for medical research is determined. It is important to consider the characteristics of a study’s design. This would include the percent follow-up, utilization of a control group, presence of blinding, heterogeneity of results, and process of randomization. Specific to meta-analyses and systematic reviews, it is important to know that the lowest quality study used in the review determines the level of evidence. In evidence-based medicine, higher levels of evidence have a larger impact on clinical recommendations.
Bhandari et al. analyzed the interobserver agreement among reviewers in categorizing the type of study, level of evidence, and subclassification for different clinical studies. The authors had 6 different surgeons with different levels of training in epidemiology analyzed 51 separate papers published in JBJS. The results demonstrated that the interobserver absolute agreement for the type of study and the level evidence was 82% and 67%, respectively. The epidemiology-trained reviewers had nearly perfect agreement in categorizing the type of study, level of evidence, and subclassification.
Wright et al. published an editorial introducing the different types of study designs and defined the different levels of evidence. Illustration A is a figure from this editorial.
Incorrect Answers:
A 55-year-old male, alcoholic, presents to the ER with acute right knee swelling and pain x 3 days. He admits to prior episodes of this pain that resolve after a few days. Serum labs reveal an ESR of 40 mm/hr and CRP of 5 mg/dl. He undergoes right knee aspiration and based on the results, he is discharged home on colchicine with the presumed diagnosis of gout. Which of the following images of the aspiration results are consistent with this diagnosis?
conclude that the patient populations and outcomes measure are homogenous and you do not have any concerns with randomization. You notice one of
the studies included had 70% follow-up, yet the remaining studies had
>80% follow-up. Knowing this, you appropriately assign what level of evidence to the systematic review?
The correct sequence of events should be the surgeon reads the surgical information on the consent to the patient, then the surgeon marks the surgical site with the patient’s assistance, then allows the anesthesia team to perform their procedure, and then performs a final Time-Out with the surgical team immediately prior to the surgical incision.
Orthopedic surgical patients are at risk of surgical errors due the number of procedures that can be performed on the bilateral extremities. The responsibility to identify the correct surgical procedure at the correct location has expanded beyond only the surgeon. The entire surgical team is
responsible for confirming the patient, surgical site, and surgical procedure. All members on the surgical team should be valued and emboldened to “speak up’ and actively participate. To help improve communication and reduce complications, surgical safety checklists have become common. In a statement
published by the AAOS is 2015, they support the use of standardized surgical systems, including the use checklists, as it is critically important to keep patients safe. In 1998, the AAOS introduced the “Sign Your Site” safety program to reduce wrong-site surgeries through improved site identification. Permanent ink should be used to mark the site(s) with the patient's assistance prior to surgery, and the site(s) should be confirmed by the surgical team during the Time-Out immediately before the start of the surgical procedure.
Singer et al. performed a study to evaluate the association between surgical teamwork and surgery safety checklist performance. Their results emphasized the importance of surgeon buy-in and clinical leadership to initiating and maintaining surgical safety checklists. In addition to surgeon buy-in and clinical leadership, factors that help maintain high-quality and consistent surgical teamwork were communication, coordination, respect, and assertiveness.
Incorrect Answers:
You are reviewing a systematic review on the 90-day complication rate and outcome for same day total joint arthroplasty for publication. After you analyze the methodology of the 6 randomized controlled trials included in the review, you
preoperative paperwork outside the room. The patient is taken to surgery and receives an interscalene block on the left shoulder after sedation. At the final Time- Out, the surgeon realizes a discrepancy with the laterality when the consent is read aloud. The surgeon aborts the case and wakes the patient. What is the correct sequence of events that should have happened to prevent this error? A: The surgeon begins
the surgery B: The surgical team performs a Time-Out C: The surgeon marks the surgical site D: The surgeon reads the surgical information on the consent to the patient E: The anesthesia team administers a local extremity block
Enchondral ossification occurs with relative stability constructs, which is represented by the bridge plate in figure C.
Fracture healing is a complex process that occurs in several key steps. The type of healing that occurs is dependent on the stability and strain of the fracture environment. In constructs with very little strain, also referred to as absolute stability, there is primary bone healing through Haversian remodeling. This produces very little callus and does not rely on a cartilage precursor. Relative stability constructs with higher strains produce a cartilage precursor, which subsequently ossifies in later stages of healing, also referred to as enchondral ossification.
Perren reviewed the biological mechanisms of fracture healing. The author discussed the importance of skeletal stiffness for limb function in addition to the healing process that utilizes soft tissue compensatory mechanisms to aid
in fracture healing. The author concluded that the goal of fracture healing is to obtain a functional limb to allow for daily mobility and activity.
Gerstenfeld et al. investigated the effect of non-selective and COX-2 selective NSAIDs effects on bone healing in a rat model. They reported a significantly higher nonunion rate in valdecoxib treated rats compared to the ketorolac group. They also noted that withdrawal of either drug at six days resulted in prostaglandin E2 levels returning to normal levels after 14 days. The authors concluded that COX-2 specific NSAIDs inhibited bone healing greater than nonspecific NSAIDs with the magnitude of the effect dependent on the duration of treatment, but the effects on prostaglandin E2 levels appear reversible with discontinuation of the drug.
Figure A is the AP radiograph of the left distal tibia with three lag screws through a spiral fracture. Figure B is the lateral radiograph of the right elbow with an olecranon plate.
Figure C is the AP radiograph of the right distal femur with a lateral bridge plate. Figure D is an AP radiograph of the left ankle with a lag screw and neutralization plate on the distal fibula. Figure E is the lateral radiograph of the forearm with a compression plate on the radius.
Incorrect Answers:
A 31-year-old man is scheduled to undergo a right shoulder arthroscopic labral repair. The surgeon is running behind and hurries to the preoperative holding area. The surgeon greets the patient and verbally confirms the operative site with the patient. The surgeon leaves the patient’s room and completes the appropriate
The yield point is the transition point between elastic and plastic deformation. The yield strength is defined as the amount of stress necessary to produce a specific amount of permanent deformation.
Stress is the amount of force applied to a material and strain is the deformation resulting
from that stress. This is graphically depicted as a stress- strain curve, where the X-axis represents strain and the Y-axis represents stress. The elastic modulus of a material is the linear region of the graph (rise over run/stress on strain). Remember, an elastic material is one that resists a change in shape (less strain or deformation under increasing stress). Non- linear regions include the toe region for some materials (tendons/ligaments) and the plastic zone, which occurs after the yield point.
Mantripragada et al. provide a review of recent advances in designing orthopaedic implants. Of note, they discuss modifications to metallic implants to reduce unwanted effects, such as nickel-free stainless steel. They also go over newer alloys with desirable mechanical and biological properties, such as tantalum, niobium, zirconium, and magnesium.
Kennedy et al. provide a classic in-vitro tension study of the human knee ligaments. They used an Instron Tension Analyzer to test the ultimate failure of the medial collateral, lateral collateral, anterior cruciate, and posterior cruciate ligaments at different loading rates. They found that the posterior cruciate ligament was the strongest (the other ligaments were all of
comparable strength) and that microscopic failure occurred before macroscopic failure. Illustration A represents a stress-strain curve.
Incorrect Answers:
is a phenomenon especially associated with a ductile material; the diameter of the material is diminished prior to fracture.
material can absorb before fracture and is the area under the stress-strain curve. Answer 5: The toe region is seen in materials such as ligaments and tendons and represents the straightening of the crimped ligament fibers.
Which of the following fixation constructs would achieve fracture healing through enchondral ossification?
The preosteoclast (precursor to the osteoclast) is the only cell of myeloid origin. The remainder of the cells involved in bone formation, remodeling, and metabolism are of mesenchymal origin.
Osteoclast signaling, function, and biology have grown increasingly well understood over the past few decades. Osteoclast activity is regulated by
osteoblasts, thereby coupling bone formation and resorption. Osteoclast differentiation from myeloid precursor cells is stimulated by key molecules including RANK, PU-1, and CSF-1. An understanding of these molecular pathways is essential to developing effective directed anti-resorptive therapies.
Zaidi et al. present a comprehensive review of proliferation, differentiation, and hormonal regulation of cells of the bone. The authors specifically discuss the unique origin of the osteoclast from the myeloid lineage and conversely the mesenchymal origin of the osteoblast. Furthermore, they highlight the
most recent understanding of the molecular mechanisms involved in osteoclast formation
and signaling, including M-CSF and RANKL.
Caterson et al. discusses mesenchymal differentiation in the context of musculoskeletal regeneration. The authors review the growth factors and bioactive signaling molecules involved in directed differentiation itno the various mesodermal lineages including bone, cartilage, muscle, tendon, marrow, and adipose. They emphasize the importance of understanding these pathways to regenerative medicine.
Illustration A is a diagram illustrating the difference between mesenchymal and myeloid lineages.
Incorrect answers:
The point on a stress-strain curve that separates the plastic and elastic regions is defined as which of the following:
Due to the risk of inducible clindamycin resistance in erythromycin-resistant MRSA, a D-test should be performed.
Isolates of MRSA that are resistant to erythromycin have been shown to become resistant to clindamycin through a process called inducible resistance, which is conferred by a plasmid that alters the 50S ribosome binding site for both clindamycin and erythromycin. Thus, when culture results reveal erythromycin-resistant MRSA, a D-zone test should be performed to check for inducible clindamycin resistance. The D-zone test is performed by
placing an erythromycin disk in proximity to a clindamycin disk on an agar plate inoculated with methicillin-resistant S aureus (MRSA). A zone of inhibition in the shape of the letter "D" is seen with an inducible strain and is considered a positive test. If the D- zone test is positive, then clindamycin should not be used because the strain of MRSA can become resistant to the treatment.
Marcotte et al. published a review on community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA). They reported that clindamycin has activity against Streptococcus species, but it is not as predictable against CA- MRSA. Clindamycin also presents a risk for the development of Clostridium difficile colitis and inducible clindamycin resistance. for which a D-zone test should be performed when culture results reveal erythromycin resistance.
Steward et al. performed a study to determine the efficacy of testing for induced clindamycin resistance in erythromycin-resistant Staphylococcus aureus. They reported that resistance to erythromycin and clindamycin can occur through methylation of their ribosomal target site (25), which is typically mediated by erm genes. They found that disk diffusion is the preferred method for testing S. aureus isolates for inducible clindamycin resistance.
Illustration A is an image of a positive D-zone test, which indicates inducible clindamycin resistance.
Incorrect Answers:
Which of the following cells involved in bone metabolism derives from a myeloid origin?
Enoxaparin primarily exerts its effects by inhibiting Factor Xa, which is labeled C in Figure A.
Enoxaparin is a low molecular weight heparin (LMWH) that primarily exerts its effects by inhibiting Factor Xa. It achieves this by binding to antithrombin to form a complex that irreversibly inactivates clotting factor Xa. Enoxaparin has the advantage of not requiring laboratory monitoring and can be reversed with protamine sulfate. However, it is important to note that protamine sulfate is less effective in reversing enoxaparin compared to unfractionated heparin (UFH).
Hyers published a review on the past, present, and future management of venous thromboembolism. He found that, for the most part, LMWH and other newer anticoagulants have been shown to be superior to UFH in terms of the venographic endpoint. He also reports that several meta-analyses have demonstrated that LMWH offers superior benefit to UFH for VTE prevention in hip and knee surgery patients.
Tørholm et al. performed a study to determine outcomes of thromboprophylaxis using LMWH compared to placebo in elective hip surgery. They found that 9 (16%) patients in the treatment group and 19 (35%) in the placebo group developed deep venous thrombosis. The risk of thrombosis in the placebo group was increased with prolonged surgery and occurred more frequently during the first 4 postoperative days. They concluded that LMWH offers safe and easily administered thromboprophylaxis in total hip replacement.
Figure A is an image of the coagulation cascade. Illustration A is an image of the
coagulation cascade with the sites of action of the various anticoagulants labeled.
Incorrect Answers:
A 42-year-old IV drug user presents to the emergency department with a large abscess on his forearm. A bedside I&D is performed and he is started on broad-spectrum IV antibiotics. Initial results from his cultures demonstrate methicillin-resistant Staphlycoccus aureus (MRSA) that is also resistant to erythromycin. The team would like to transition him to oral clindamycin. Prior to transitioning him to clindamycin, which additional laboratory test should be performed?
Teriparatide promotes bone formation in patients at high risk of fractures due to severe osteoporosis that is refractory to multiple treatments, including bisphosphonates and cement augmentation. Teriparatide is a human recombinant N-terminal parathyroid hormone.
Teriparatide administered in daily injections results in bony formation, whereas continuous infusion results in bony resorption. In rat models, teriparatide caused an increase in the incidence of osteosarcoma, and thus should only be prescribed for patients for whom the potential benefits outweigh the potential risk. It can be administered in isolation or as an adjunct treatment during bisphosphonate therapy. However, in patients on long-term bisphosphonate therapy, discontinuation of bisphosphonates are advised to reduce potential complications of atypical femur fractures and jaw osteonecrosis.
Watts et al. published a review article on postmenopausal osteoporosis. They reported that bisphosphonates can accumulate in bone, thus after a period of treatment, lower- risk patients should be offered a drug holiday. Denosumab, on the other hand, is not sustained when treatment is discontinued, so no drug holiday is warranted. They concluded that, although there are safety
concerns regarding atypical femoral fracture and osteonecrosis of the jaw with long term use, the benefit of hip fracture risk reduction far outweighs the risk of these relatively uncommon side effects.
Song et al. performed a meta-analysis to investigate the effect of teriparatide monotherapy and the additive effect of teriparatide on antiresorptive agents in postmenopausal women with osteoporosis. They reported that teriparatide monotherapy significantly improved bone mineral density (BMD) in the lumbar spine, total hip, and femoral neck compared with placebo; the additive effect
of teriparatide over hormone replacement therapy (HRT) and denosumab agents was evident in all 3 skeletal sites; however, teriparatide plus alendronate did not demonstrate additive effect in total hip and femoral neck. They concluded that, for patients with osteoporosis who were at high risk for fracture, BMD increased more in patients receiving teriparatide than in those receiving alendronate.
Saag et al. compared the use of teriparatide or alendronate in the management of glucocorticoid-induced osteoporosis. They reported that BMD had increased more in the teriparatide group than in the alendronate group in the lumbar spine and total hip at 6 and 12 months, respectively. They also reported significantly fewer new vertebral fractures in the teriparatide group compared to the alendronate group. They concluded that in severely osteoporotic patients at high risk for fracture, BMD increased more in patients receiving teriparatide than in those receiving alendronate.
Figure A depicts multiple vertebral insufficiency fractures in the setting of a prior cement augmentation procedure.
Incorrect Answers:
Where in the coagulation cascade shown in Figure A does enoxaparin primarily exert its effects?
This patient is presenting with signs of a septic nonunion after open reduction and internal fixation (ORIF) of a radial shaft fracture. Of the choices listed, C- reactive protein (CRP) is the best predictor of infection in the setting of nonunion.
Nonunions after fracture fixation may occur from infection. The most sensitive and readily-available laboratory marker to detect infection is the CRP. CRP is an acute phase reactant that significantly rises within 6 hours after tissue damage or onset of clinical infection. CRP then peaks 2-3 days later and returns to normal levels 5-21 days after the inciting event if it is treated (e.g. antibiotics for cellulitis). In septic nonunions, the chance of fracture healing is low if the infection is not properly treated, and chronic infection can lead to substantially elevated CRP values.
Wang et al. evaluated the effectiveness of laboratory tests in the diagnosis of
infected nonunion. They reported that the sensitivity and specificity of CRP for detection of infected nonunions are both higher than those of IL-6. They concluded that the diagnostic utility of CRP was superior to IL-6, which is contrary to similar studies comparing these markers in prosthetic joint infection patients.
Stucken et al. performed a study to investigate the utility of a standardized protocol to rule out infection in high-risk patients and to evaluate the efficacy of each component of the protocol. They reported that the ESR and the CRP levels were both independently accurate predictors of infection. They
concluded that their protocol can help surgeons to risk-stratify patients prior to the surgical treatment of a nonunion, allowing them to counsel patients more appropriately.
Figure A depicts a nonunion of a radial shaft fracture after ORIF. Incorrect Answers:
An 85-year-old woman presents with severe back pain and the CT shown in Figure A. Her history is notable for prior vertebral compression fractures for which she underwent a cement augmentation procedure. She has been on bisphosphonates for the last 5 years, without improvement of her osteoporosis. She has no history of malignancy. What is the mechanism of action of the medication that should be prescribed for her refractory osteoporosis?
A receiver operating characteristic (ROC) curve is used to determine responsiveness.
Responsiveness is a measure of the diagnostic ability of different tests. It can be determined by calculating the C-statistic, which represents the area under a
Receiver Operating Characteristic (ROC) curve. On a ROC curve, the false positive rate (1 - specificity) is plotted on the x-axis, while the true positive rate (sensitivity) is plotted on the y-axis. The higher the area under the curve, the more responsive the outcome measure. A value of 0.5 indicates a random chance and a therefore useless test, while values above 0.75 usually are considered to be adequately responsive.
Kocher et al. published a review on clinical epidemiology and biostatistics for orthopaedic surgeons. They reported that the relationship between the sensitivity and specificity of a diagnostic test can be portrayed with use of a receiver operating characteristic (ROC) curve. A ROC graph shows the relationship between the true- positive rate (sensitivity) on the y-axis and the false-positive rate (1 − specificity) on the x-axis plotted at each possible cutoff. Overall diagnostic performance can be evaluated on the basis of the area under the ROC curve.
Hanley et al. published a review on the meaning and use of the area under a receiver operating characteristic (ROC) curve. They reported that it represents the probability that a randomly chosen diseased subject is (correctly) rated or ranked with greater suspicion than a randomly chosen non-diseased subject.
Illustration A is an example of a ROC curve. Illustration B is an example of a funnel plot. Illustration C is an example of a Kaplan-Meier curve. Illustration D is a table outlining the interpretation of the Cronbach alpha coefficient. Illustration E is an example of a forest plot.
Incorrect Answers:
A 32-year-old man underwent open reduction and internal fixation for an open radial shaft fracture 6 months ago. He is now experiencing fevers and chills at night and pain and swelling over the surgical site. A current radiograph is depicted in Figure A. What is the most accurate laboratory test for assessing his most likely diagnosis?
The Patient-Reported Outcomes Measurement Information System (PROMIS) has been shown to have reduced floor and ceiling effects compared to other assessment tools.
The PROMIS system was developed to produce a highly reliable, precise, and versatile assessment of outcomes. When administered in a computerized adaptive mode, each question that is answered is followed with a customized follow-up question based on the previous response, which allows for reduced testing items and time. Further, the results of the assessment are reported in T-scores with 50 being the population norm and with a standard deviation of
Question 19
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?

Explanation
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 20
What is the most common presentation of a benign bone tumor in childhood?
Explanation
REFERENCES: Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 21
5 mm of change in the atlanto-dens interval (ADI) between flexion and extension views
Explanation
With the introductions of disease-modifying antirheumatic agents (DMARDs), the incidence of RA patients undergoing cervical spine surgery has decreased significantly. Basilar invagination, atlantoaxial instability, and subaxial subluxation are the three most common manifestations of cervical disease. Multiple studies in RA patients with untreated or poorly controlled disease have led to the development of a set of measurements that identify patients who require surgical intervention and predict outcome after surgery. Additionally, progressive neurological compromise and
refractory
pain
are
indications
for
intervention.
Kim and Hilibrand reviewed management of the rheumatoid cervical spine and outline parameters for surgical intervention. These include a PADI < 14 mm, cervicomedullary angle <135 degrees, progressive neurological deficit, refractory pain, atlantoaxial impaction as determined by migration >5 mm rostral to McGregor's line, and subaxial canal diameter < 14 mm.
Boden et al. analyzed 73 patients followed for rheumatoid cervical spine disease with an average follow up of 7 years. They found that the PADI correlated with paralysis. Patients with PADI less than 10 mm had no recovery, and all patients with PADI greater than 14 mm had full recovery.
Illustration A demonstrates the measurement of the ADI and PADI. Illustration B demonstrates how to measure the cervicomedullary angle (as marked by A), which is typically determined on MRI
Incorrect
Question 22
What are the four most common soft-tissue sarcomas to spread via the lymph node system?
Explanation
REFERENCES: Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Blazer DG III, Sabel MS, Sondak VK: Is there a role for sentinel lymph node biopsy in the management of sarcoma? Surg Oncol 2003;12:201-206.
Question 23
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts? Review Topic
Explanation
Question 24
A 35-year-old active woman with rheumatoid arthritis experiences right shoulder pain following an extended course of corticosteroids (Figures 96a and 96b).

Explanation
The indication for anatomic TSA is end-stage glenohumeral arthritis with an intact rotator cuff. For the 62-year-old man, his radiographs reveal osteoarthritis, and his MR image shows an intact rotator cuff. Although humeral head replacement has historically been employed for this disorder, pain relief is not as reliable as with TSA, and the revision rate is higher. rTSA is generally reserved for patients with a nonfunctional rotator cuff.
For this 58-year-old patient with a full-thickness rotator cuff tear, preserved motion, and weakness in forward elevation, a rotator cuff repair is the most appropriate treatment. In the absence of degenerative changes, shoulder hemiarthroplasty or anatomic TSA is not indicated. Although indications for rTSA continue to evolve, well-compensated range of motion and a medium-sized rotator cuff tear in a younger patient are not among them.
rTSA is an emerging treatment for comminuted proximal humerus fractures in elderly patients. Although hemiarthroplasty has been a traditional treatment, current evidence suggests rTSA more reliably restores range of motion, and this 78-year-old patient's CT scan shows a small and comminuted greater tuberosity fragment that is unlikely to heal. ORIF is another option, but the CT scan also shows a small humeral head fragment that suggests osteopenia, making fixation more tenuous and likely less reliable.
A common problem associated with hemiarthroplasty for glenohumeral osteoarthritis is symptomatic glenoid degeneration that necessitates revision. This 55-year-old patient’s images reveal this is the case, although his infection workup is negative. His examination findings suggest an intact subscapularis repair. With a functioning rotator cuff and symptomatic glenoid arthritis, a conversion to anatomic TSA is indicated. In the absence of a functioning rotator cuff in an older patient, an rTSA is a better option.
This 72-year-old patient has classic symptoms and radiographs of cuff tear arthropathy. For patients with massive rotator cuff tear and glenohumeral arthritis, neither anatomic TSA nor rotator cuff repair is indicated. Hemiarthroplasty has historically been indicated for cuff tear arthropathy, but rTSA outcomes for this disorder have been superior and are now the preferred option.
Comminuted proximal humerus fractures in young, active patients are treated primarily with ORIF. The absence of glenohumeral arthritis removes anatomic TSA as a possibility, and concerns about implant longevity in younger, active patients such as this 40-year-old laborer contraindicate rTSA. Hemiarthroplasty is still employed in 3- and 4-part fractures but is generally reserved for subacute presentations or dislocations in which the humeral head is dysvascular and unlikely to survive. In this acute setting, a fixation procedure is preferred.
The 71-year-old patient who has had 2 failed rotator cuff repairs has an MR image that reveals another recurrent tear that is retracted to the glenoid. Her examination findings reveal classic signs
of a decompensated rotator cuff tear with pseudoparalysis and weakness in forward elevation. Although infection is a concern in the setting of multiply failed rotator cuff repair, the workup is negative in this scenario. Because this patient has a dysfunctional rotator cuff and has failed previous attempts at repair, a conversion to rTSA is the better option. In the absence of degenerative changes, hemiarthroplasty and anatomic TSA are not indicated.
The indications for hemiarthroplasty continue to narrow, but it is still a consideration for young patients with unipolar shoulder degeneration. In this 35-year-old patient, her MR image shows avascular necrosis in the humeral head, and her arthroscopy suggests arthritic change only on the humeral side with an uncompromised glenoid. To best treat young and active patients, a hemiarthroplasty that articulates with healthy glenoid cartilage can provide good pain relief and functional outcomes. Anatomic TSA is also reasonable but not an optimal option considering the normal glenoid condition. rTSA is not a consideration when a young patient’s MR images reveal an intact rotator cuff.
RECOMMENDED READINGS
Torchia ME, Cofield RH, Settergren CR. Total shoulder arthroplasty with the Neer prosthesis: longterm results. J Shoulder Elbow Surg. 1997 Nov-Dec;6(6):495-505. PubMed PMID: 9437598. View Abstract at PubMed
Chalmers PN, Slikker W 3rd, Mall NA, Gupta AK, Rahman Z, Enriquez D, Nicholson GP. Reverse total shoulder arthroplasty for acute proximal humeral fracture: comparison to open reduction-internal fixation and hemiarthroplasty. J Shoulder Elbow Surg. 2014 Feb;23(2):197-204. doi: 10.1016/j.jse.2013.07.044. Epub 2013 Sep 27. PubMed PMID: 24076000. View Abstract at PubMed
Groh GI, Wirth MA. Results of revision from hemiarthroplasty to total shoulder arthroplasty utilizing modular component systems. J Shoulder Elbow Surg. 2011 Jul;20(5):778-82. doi: 10.1016/j.jse.2010.09.014. Epub 2011 Jan 13. PubMed PMID: 21232989. View Abstract at PubMed
Orfaly RM, Rockwood CA Jr, Esenyel CZ, Wirth MA. Shoulder arthroplasty in cases with avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2007 May-Jun;16(3 Suppl):S27-32. Epub 2006 Nov 16. PubMed PMID: 17113317. View Abstract at PubMed
Sershon RA, Van Thiel GS, Lin EC, McGill KC, Cole BJ, Verma NN, Romeo AA, Nicholson GP. Clinical outcomes of reverse total shoulder arthroplasty in patients aged younger than 60 years. J Shoulder Elbow Surg. 2014 Mar;23(3):395-400. doi: 10.1016/j.jse.2013.07.047. Epub 2013 Oct 12. PubMed PMID: 24129052. View Abstract at PubMed
Question 25
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?
Explanation
REFERENCES: Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Lowell TD, Errico TJ, Eskenazi MS: Use of steroids after discectomy may predispose to infection. Spine 2000;25:516-519.
Question 26
Intrinsic muscles of the foot act on the toes by
Explanation
REFERENCES: Myerson MS, Shereff MJ: The pathologic anatomy of claw and hammertoes.
J Bone Joint Surg Am 1989;71:45-49.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 71-80.
Question 27
2010 Pediatric Orthopaedic Examination Answer Book • 9 A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis?
Explanation
There is an asymmetry of the deformities that makes diastrophic dysplasia less likely.
REFERENCES: Goldberg MJ, Yassir W, Sadeghi-Nejad A: Clinical analysis of short stature. J Pediatr Orthop 2002;22:690-696.
Parmar VS, Stanitski DF, Stanitski CL: Interpretation of radiographs in a pediatric limb deformity practice: Do
radiologists contribute? J Pediatr Orthop 1999;19:732-734. Question 4
Patients with slipped capital femoral epiphysis are more likely to experience a delay in definitive diagnosis if they initially present to a physician reporting which of the following problems?
L Limp
Hip pain
Knee pain
Proximal thigh pain
Buttock pain
DISCUSSION: A delay in diagnosis of slipped capital femoral epiphysis (SCFE) can lead to significant worsening of the deformity or even progression from a stable to an unstable SCFE. Those patients that report knee pain as their primary complaint are most likely to experience significant delay. Other variables associated with this delay include Medicaid insurance and stable SCFE.
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis.
AL-Madena Copy
10 • American Academy of Orthopaedic Surgeons
Pediatrics 2004;113:e322-e325.
Rahme D, Comley A, Foster B, et al: Consequences of diagnostic delays in slipped capital femoral epiphysis. J Pediatr Orthop B 2006;15:93-97.
Question 28
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
Explanation
REFERENCES: Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 29
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?

Explanation
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 30
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Howard FM: Fracture of the basal joint of the thumb. Clin Orthop 1987;220:46-51.
Question 31
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?
Explanation
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory

drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Question 32
In the most common condition causing a winged scapula, which of the following nerves is affected?
Explanation
REFERENCES: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995.
van Alfen N, van Engelen BG: The clinical spectrum of neuralgic amyotrophy in 246 cases. Brain 2006;129:438-450.
Question 33
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?

Explanation
clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
Question 34
A 70-year-old woman had poliomyelitis as a young child, and the residual weakness she has as an adult principally involves the lower extremities. She now notes progressive weakness in both legs and she tires easily. What is the best course of action?
Explanation
REFERENCES: Dalakas MC, Elder G, Hallett M, et al: A long-term follow-up study of patients with post-poliomyelitis neuromuscular symptoms. N Eng J Med 1986;314:959-963.
Kasser JE (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 683-687.
Question 35
The arrow in the axial T 1 -weighted MRI scan shown in Figure 18 is pointing to which of the following structures?
Explanation
REFERENCES: Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Denman EE: The anatomy of the space of Guyon. Hand 1978;10:69-76.
Question 36
A B C Figures 64a through 64c are the MR images and radiograph of an active 30-year-old man who has been treated for pain in his subtalar joint for 6 months. He has had casting, physical therapy, and bracing but continues to have activity-limiting pain. An injection into the subtalar joint under fluoroscopic guidance temporarily relieved his pain. His best surgical option at this time is

Explanation
When contemplating the causes of subtalar joint degeneration in young patients, an unstable tarsal coalition should be considered in the absence of antecedent trauma. Initial treatment with casting is appropriate because this intervention can relieve symptoms for many patients. There are 2 surgical options for a symptomatic tarsal coalition: bar resection or completion fusion. Risk factors for a poor outcome after bar resection are adult age and a bar that encompasses more than 50% of the middle facet of the subtalar joint. Because this patient has both risk factors, the appropriate procedure is a subtalar fusion.
RECOMMENDED READINGS
Comfort TK, Johnson LO. Resection for symptomatic talocalcaneal coalition. J PediatrOrthop. 1998 May-Jun;18(3):283-8. PubMed PMID: 9600549. View Abstract at PubMed
Thorpe SW, Wukich DK. Tarsal coalitions in the adult population: does treatment differ from the adolescent? Foot Ankle Clin. 2012 Jun;17(2):195-204. doi: 10.1016/j.fcl.2012.03.004. Epub 2012 Apr 6. Review. PubMed PMID: 22541520. View Abstract at PubMed
Question 37
A 10-year-old girl is seen in the emergency department after being involved in a motor vehicle accident. She has right hip pain and is unable to bear weight. She has no neurovascular deficits and no other injuries. Radiographs reveal a posterior dislocation of the right hip without apparent fracture. The acetabulum appears to be developing normally. What is the best course of treatment? Review Topic
Explanation
Question 38
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 39
What are the two terminal branches of the lateral cord of the brachial plexus?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.
Shin AY, Spinner RJ, Steinmann SP, et al: Adult traumatic brachial plexus injuries. J Am Acad Orthop Surg 2005;13:382-396.
Question 40
In X-linked hypophosphatemic rickets, the gene defect may be found in which of the following?
Explanation
Question 41
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of
Explanation
REFERENCES: Ahn NU, Ahn UM, Andersson GB, et al: Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am 2003;14:675-692.
Algers G, Pettersson K, Hildingsson C, et al: Surgery for chronic symptoms after whiplash injury: Follow-up of 20 cases. Acta Orthop Scand 1993;64:654-656.
Rao R: Neck pain, cervical radiculopathy, and cervical myelopathy: Pathophysiology, natural history, and clinical evaluation. Instr Course Lect 2003;52:479-488.
Question 42
A 17-year-old man sustained a 5-mm laceration on the lateral aspect of the hindfoot while working on a farm. Examination in the emergency department revealed no fractures. Twenty-four hours later, he returns to the emergency department with increasing foot pain. Thin brown drainage is seen emanating from the wound. He has a temperature of 102.0° F (38.9° C), a pulse rate of 120, and a blood pressure of 80/40 mm Hg. Examination of the foot reveals diffuse swelling, ecchymosis, tenderness, and crepitus with palpation. Current radiographs are shown in Figures 40a and 40b. Management should now consist of
Explanation
REFERENCES: Pellegrini VD, Reid JS, Evarts CM: Complications, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 1, pp 458-463.
Ayers DC, Murray DC: Complications of the treatment of fractures and dislocations: General considerations, in Epps Jr CH (ed): Complications in Orthopedic Surgery, ed 4. Philadelphia, PA, JB Lippincott, 1994, pp 3-48.
Question 43
Figure 13 shows the MRI scan of a 29-year-old rock climber who reports increasing shoulder pain and weakness. Based on these findings, atrophy will most likely occur in which of the following muscles?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Ianotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG: Association of glenoid labral cysts and labral tears in glenohumeral instability: Radiologic findings and clinical significance. Radiology 1994;190:653-658.
Question 44
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 45
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?
Explanation
REFERENCES: Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Samson IR, Springfield DS, Suit HD, Mankin HJ: Operative treatment of sacrococcygeal chordoma: A review of twenty-one cases. J Bone Joint Surg Am 1993;75:1476-1484.
Question 46
A patient has a large T11-T12 disk herniation that is causing substantial compression of the spinal cord. The patient reports walking imbalance over the past few weeks. Examination of the patient's reflexes is likely to show Review Topic
Explanation
Question 47
Two major pharmacologic classes of bisphosphonates exist: nitrogen-containing and non-nitrogen-containing compounds. The nitrogen-containing compounds work by which of the following actions?
Explanation
Question 48
The function of which of the following structures is to resist internal tibial rotation with the knee in full extension? Review Topic
Explanation
The posterior oblique ligament is a structure within the posteromedial corner of the knee, with attachments proximally to the adductor tubercle of the femur and distally to the tibia/posterior knee capsule. The posterior oblique ligament and posteromedial capsule play a significant role in the prevention of additional posterior tibial translation in the knee in the setting of posterior cruciate ligament injury. They also act to resist internal tibial rotation with the knee in full extension.
Griffith et al. reports that the posterior oblique ligament provides significant resistance to valgus and internal rotation forces with knee extension. They used a cadaver model and demonstrated that the superficial MCL resists valgus and external rotation forces more than the posterior oblique ligament, while the posterior oblique ligament is more involved in resisting internal rotation.
Tibor et al. reviews the anatomy of the posteromedial corner of the knee. They report that failing to recognize injury to these structures may cause failure of cruciate ligament reconstruction surgery, and that reconstruction or repair of the posteromedial corner may be indicated in the face of multiple ligament injuries.
Illustration A shows the posteromedial corner of the knee, including the posterior oblique ligament.
Incorrect answers:
1-4: These structures are not primary restraints to internal tibial rotation in full extension.
Question 49
In infantile idiopathic scoliosis, which of the following factors suggests progression? Review Topic
Explanation
Question 50
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of
Explanation
REFERENCES: Simon MA, Springfield DS: Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 51
Following its exit from the sciatic notch, the sciatic nerve passes between what two muscles?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 335-348.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Williams,
1978, Figure 4-34.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 52
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 53
Which of the following ligaments provides the major static restraint to lateral patellar displacement?
Explanation
The medial patellotibial band was found to be functionally unimportant and the medial patellomeniscal ligament was found to contribute 22% to the lateral displacement force.
Question 54
A 27-year-old right hand dominant construction worker falls off a scaffold onto his outstretched arm. Figure A exhibits the radiograph taken at a local emergency room. Following treatment, he is placed in a sling and follows up at your office two weeks later. He complains of a feeling that his arm is going to 'pop out'. Which specific physical examination finding is likely to be present? Review Topic
Explanation
Posterior dislocations occur less frequently than anterior dislocations, and are often missed. Following closed reduction, persistent instability can occur, usually associated with posterior capsular or labral pathology. Posteriorly directed provocative maneuvers, such as the Kim test can be positive.
Robinson et al. performed an epidemiologic analysis on 120 posterior dislocations. Recurrent instability occurred at a rate of 17.7%. Risk factors for recurrent instability included age less than 40-years-old, dislocation during seizure, and a large reverse Hill-sachs (>1.5 cm3).
Kim et al. describe the Kim lesion, a separation between the posteroinferior labrum and the articular cartilage without complete detachment of the labrum, which cause persistent posterior instability.
Figure A depicts a posterior dislocation on xray. Illustration A depicts the Kim test, which is performed by having the patient seated, arm at 90° abduction, followed by flexing the shoulder to 45° forward flexion while simultaneously applying axial load on the elbow and posterior-inferior force on the upper humerus. The test is positive when there is pain. Video 1 depicts the proper way to perform a Kim Test.
Incorrect answers:
Question 55
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 56
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
Explanation

OrthoCash 2020
Which of the following is the most common cause of early revision surgery (<20 weeks) following a hip resurfacing arthroplasty?
Periprosthetic fracture
Rupture of abductors
Dislocation
Heterotopic ossification
Post-operative stiffness
Periprosthetic fracture, specifically femoral neck fracture, is the most common cause of early revision less than 20 weeks following surgery.
The rate of femoral neck fractures following hip resurfacing varies, but most literature reports a rate of 1%. A majority of these fractures happen in the early post-operative period and are the most frequent cause of revision surgery within several months following surgery. The cause is usually multifactorial, but placing the femoral implant in varus, osteonecrosis, and notching have been proven risk factors for fracture.
Little el al. report on 377 patients undergoing hip resurfacing. 13 required revision including 8 for fracture of the femoral neck and 3 for loosening of a component. Evidence of osteonecrosis was seen in two of these cases, leading the authors to believe it may contributed to fracture.
Illustration A shows a comparison of a typical total hip replacement and a hip resurfacing arthroplasty. Illustration B shows notching of the femoral neck, a known cause of femoral neck fracture following hip resurfacing. Illustration C shows a femoral neck fracture in a patient with a hip resurfacing.
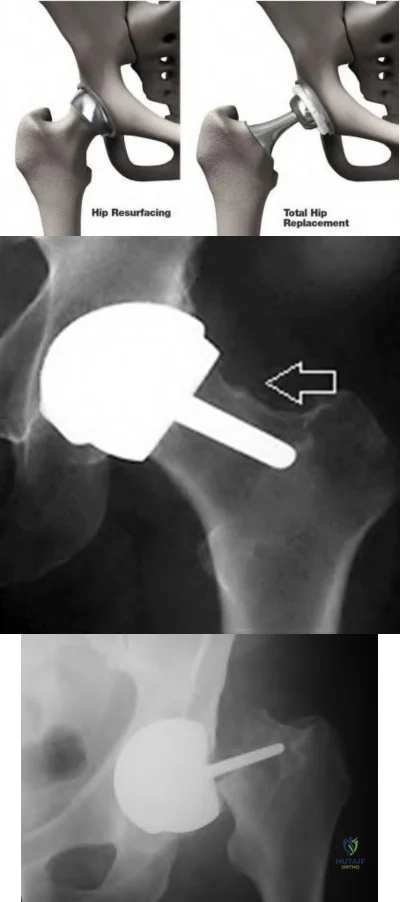
OrthoCash 2020
A 55-year-old male undergoes a revision total knee arthroplasty of an implant that is only 3 years old. At the time of surgery, the tibial polyethylene liner shows catastrophic delamination and cracking. What is the most likely cause of this extensive, accelerated wear of the polyethylene liner?
Sterilization in ethylene oxide
Gamma irradiation of the polyethylene liner in the presence of air
Gamma irradiation of the polyethylene liner with vacuum packaging
Gamma irradiation of the polyethylene liner in nitrogen
Gamma irradiation of the polyethylene liner in argon Corrent answer: 2
Irradiation of polyethylene in air (i.e. oxygen present) has been shown to be a risk factor for catastrophic failure after total knee replacement.
Free radicals are generated when polyethylene is irradiated in the presence of air. Initially, these free radicals result in cross-linking. However, if the polyethylene is exposed to these free radicals for an extended period of time, delamination, cracking, and catastrophic failure may ensue. The industry has completely abandoned this method of sterilization as a result. Currently, the standard of care is irradiation of polyethylene in an inert gas (e.g. argon, nitrogen or vacuum packaging). The amount of oxidative products when polyethylene is sterilized in the absence of oxygen is much less and does not lead to catastrophic failure.
Sterilization without irradiation is another option (ethylene oxide). When this occurs, there is no cross-linking and thus the increased wear properties are lost. However, since there is no oxidization, you do not have the risk of catastrophic failure as seen in those liners irradiated in the presence of oxygen.
The cited reference by McNulty et al. from Orthopedics discusses the influence of sterilization methods on wear performance. They found that gamma irradiation and storage of the polyethylene components in an essentially oxygen-free environment imparted by gamma irradiation in a vacuum foil pouch (GVF) protects the components from oxidization.
Illustration A shows a polyethylene liner that has undergone catastrophic wear as a result of irradiation in the presence of oxygen.
Incorrect Answers:
catastrophic wear, although wear properties are less than gamma irradiation in the absence of air.

OrthoCash 2020
Which of the following interventions reduces osteolysis around distal portion of the femoral stem when performing a total hip arthroplasty?
Use of an extended offset femoral neck component
Use of a proximal circumferentially coated ingrowth stem
Use of a collared stem
Use of a long femoral stem
Ensuring that the stem fills the diaphysis of the femur Corrent answer: 2
Osteolysis of the femur is caused by activation of macrophages by microscopic polyethylene particles within the "effective joint space", defined as any area where joint fluid can come into contact with bone. This can occur above the acetabular cup, through screw holes, and down the femoral shaft around the prosthetic stem. Ideally, with a cementless stem, both the proximal and metaphyseal femur are well filled by the prosthesis. Collared stems are used to augment poor calcar bone quality or bone loss.
Sinha et al showed in a retrospective review of 101 hips with cementless circumferentially coated femoral stems no distal femur osteolysis occurred, but 82% showed “evidence of proximal femur stress shielding”, though only 38% showed proximal femoral osteolysis.
OrthoCash 2020
During a minimally invasive approach to total hip arthroplasty a femoral periprosthetic fracture occurs. Which of the following steps is crucial to properly treat this complication?
Transitioning to an extensile approach to adequately visualize and reduce the fracture
Limiting post-operative weight bearing
Switching to a cemented femoral stem to avoid the stresses created during press-fit fixation
Delaying the arthroplasty until the fracture has healed
Supplementing the fracture with autograft Corrent answer: 1
Proper treatment of an intraoperative femoral fracture during total hip arthroplasty involves adequate exposure, anatomic reduction, and bypassing the fracture site by 2 cortical diameters of the femur with a long stem. This may involve repositioning the patient on the table if the arthroplasty is performed in the supine position. Minimally invasive surgical techniques have been developed to insert the components through smaller exposures and less soft tissue dissection. The purported advantages include faster rehabilitation, less blood loss, shorter hospital stays, and better cosmesis. However, complications an arise if the surgeon sacrifices surgical exposure and visualization.
Fehring et al review 3 cases of total hip arthroplasty performed through minimally invasive techniques with catastrophic outcomes. Intra-operative fracture, chronic instability, and death were all identified.
OrthoCash 2020
A 70-year-old man underwent total hip arthroplasty 4 months ago and has experienced 3 dislocations. Radiographs reveal no failure of the hardware and an acetabular component that has an abduction
angle of 40 degrees and a version of 10 degrees retroverted. What is the most appropriate treatment for the recurrent dislocations?
hip abduction brace
revision of the acetabular liner to a constrained type
revision of the entire acetabular component
revision of the femoral head to a larger size
revision to an extended offset prosthesis Corrent answer: 3
Per Dorr et al: post-operative hip instability can be caused by several factors: soft tissue imbalance, component malposition, or position. Component malposition, as in this case, should be treated with revision of the offending component. In this case the acetabulum was placed in retroversion when it should have been 15-20 degrees anteverted. None of the other options addresses the cause of the instability. According to Morrey, the most signficant risk factors to instability are prior hip surgery, trochanteric nonunion, and posterior surgical approach. He wrote that the most reliable way to correct instability is to reorient a retroverted acetabular cup.
OrthoCash 2020
In patients with sickle cell disease and asymptomatic osteonecrosis of the femoral head identified with magnetic resonance imaging, what percentage will eventually go on to femoral head collapse?
Question 57
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
REFERENCES: Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 58
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
Explanation
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, www.aaos.org/research/guidelines/ PEguide.asp
Question 59
A 67-year-old man with right shoulder osteoarthritis (OA) remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder shows eccentric posterior glenoid wear with 10° of retroversion. What is the appropriate management of this glenoid bone loss during surgery for an anatomic total shoulder arthroplasty?
Explanation
glenoid bone grafting may be considered for glenoid retroversion >15°.
Question 60
A 23-year-old male is an unrestrained driver in a motor vehicle accident and sustains an unstable pelvic ring fracture. During fluoroscopic-aided fixation, a lateral sacral view is required for proper placement of which of the following fixation methods?

Explanation
Routt et al (1997) examined the sacral slope and sacral alar anatomy in cadavers and a series of patients. They determined that the pelvic outlet and lateral sacral plain films provide the best plain radiographic view of the sacral ala. They recommended routine usage of these views intraoperatively to guide screw placement.
Routt et al (2000) reported on the early complications of percutaneous placement of iliosacral screws for treatment of posterior pelvic ring disruptions. While technically challenging, this technique leads to less blood loss and lower rates of infection compared to traditional open techniques.
Barei et al described methods of anterior and posterior pelvic ring disruptions. They determined that successful placement depends on accurate closed reduction, excellent intraoperative fluoroscopic imaging, and detailed preoperative planning. Early treatment decreased hemorrhage, provides patient comfort, and allows early mobilization.
Question 61
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of Review Topic

Explanation
Question 62
A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
Explanation
REFERENCES: Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
McGuire R Jr: The role of anterior surgery in the treatment of thoracolumbar fractures. Orthopedics 1997;20:959-962.
Question 63
A 66-year-old female presents to your clinic complaining of back pain, difficulty standing-up straight, weakness in her legs, and neurogenic claudication. On upright thoracolumbar radiographs, there is a 75 degree thoracolumbar curve with the apex at L2, and the C7 plumb line falls 12 cm anterior to the posterosuperior corner of S1. Aside from a decompression of the stenotic levels, which of the following choices will lead to the MOST reliable decrease in overall disability? Review Topic
Explanation
Spinal malalignment in Adult Spinal Deformity (ASD) challenges balance mechanisms used for maintenance of an upright posture to achieve the basic human needs of preserving level visual gaze and retaining the head over the pelvis. Severe malalignment can result in greater muscular effort and energy expenditure to maintain the erect posture as well as use of compensatory mechanisms. As such, surgical correction of these deformities are aimed at achieving proper spinopelvic alignment.
Glassman et al. performed a multi-center retrospective study of 298 adults with spinal deformity. Regardless of operative (129 patients) or non-operative care (172 patients) a positive sagittal balance was the found to be the most reliable predictor of clinical symptoms in both patient groups.
Schwab et al. published a current concepts review on operative management for adult spinal deformities and identified three major goals of surgery: (1) Correct the SVA to
within 5 cm of neutral, (2) Ensure the pelvic tilt is less than 20 degrees, (3) Ensure the lumbar lordosis is within 9 degrees of the pelvic incidence.
Illustration A demonstrates how to measure the SVA. Illustration B depicts the realignment objectives in the saggital plane as described by Schwab et al.
Incorrect
Question 64
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 65
A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.
The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts.
The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 66
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
application of a hinged external fixator may be considered.
Question 67
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of
Explanation
REFERENCES: King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Wang SY, Lomasney LM, Demos TC, Hopkinson WJ: Radiologic case study: Traumatic myositis ossificans. Orthopedics 1999;22:991-995, 1000.
Question 68
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 69
A healthy 2-year-old boy falls from a swing and sustains a displaced midshaft femoral fracture with 1 cm of shortening. What is the most appropriate treatment?
Explanation
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Figure 29a Figure 29b
Question 70
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 71
A 63-year-old woman who sustained a distal radial fracture 2 months ago now reports that she is unable to achieve active extension of the thumb at the interphalangeal joint. What type of trauma may lead to this clinical finding?
Explanation
REFERENCES: Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles’ type of fracture. Hand 1982;14:41-47.
Hirasawa Y, Katsumi Y, Akiyoshi T, et al: Clinical and microangiographic studies on the rupture of the EPL tendon after distal radial fractures. J Hand Surg Br 1990;15:51-57.
Question 72
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight. After closed manipulative reduction and splint placement, she is scheduled for operative treatment. The stability of the syndesmosis should be evaluated after

Explanation
Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
Maximizes the surface area for ankle joint loading
Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 73
A 70-year-old woman reports anterior knee pain after undergoing an uncomplicated total knee arthroplasty 6 months ago. Examination reveals prepatellar tenderness, with no extensor lag. The radiographs shown in Figures 25a through 25c reveal a well-fixed patellar component. Management should consist of
Explanation
REFERENCES: Rorabeck CH, Angliss RD, Lewis PL: Fractures of the femur, tibia, and patella after total knee arthroplasty: Decision making and principles of management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 449-458.
Hozack WJ, Goll SR, Lotke PA, Rothman RH, Booth RE Jr: The treatment of patellar fractures after total knee arthroplasty. Clin Orthop 1988;236:123-127.
Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 74
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 75
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of
Explanation
(greater than 50%) for treating MDI.
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896.
Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am
2000;82:919-928.
Miniaci A, Birnie J: Thermal capsular shrinkage for treatment of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003;85:2283-2287.
Question 76
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
REFERENCE: Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 77
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C
Explanation
Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
Elbow arthroscopy with debridement
Immobilization and rest for 6 weeks
Corticosteroid injection
Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 78
In displaced calcaneal fractures, what fragment is the only one that remains in its anatomic position?
Explanation
REFERENCES: Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Eastwood DM, Gregg PJ, Atkins RM: Intra-articular fractures of the calcaneum: Part I. Pathological anatomy and classification. J Bone Joint Surg Br 1993;75:183-188.
Eastwood DM, Langkamer VG, Atkins RM: Intra-articular fractures of the calcaneum: Part II. Open reduction and internal fixation by the extended lateral transcalcaneal approach. J Bone Joint Surg Br 1993;75:189-195.
Question 79
A 56-year-old woman undergoes an arthroscopic rotator cuff repair for a two-tendon retracted tear (supraspinatus and infraspinatus), requiring the use of four suture anchors placed in a double row technique. At her 1 month follow-up visit, what is the appropriate recommendation for her continued rehabilitation program? Review Topic
Explanation
Question 80
A 40-year-old male who sustained an open pilon fracture 2 weeks ago is scheduled for a below-the-knee amputation (BKA). What laboratory value is the best predictor for wound healing?

Explanation
Question 81
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of
Explanation
REFERENCES: Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737.
Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Blair B, Rokito AS, Cuomo F, et al: Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
Question 82
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
REFERENCES: Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 83
-What is the recommended treatment for this injury?
Explanation
The hypertrophic zone of the growth plate has been implicated as the weak link in the physis in acute injuries. Epiphysiolysis of the proximal humerus in throwing athletes occurs as the result of tension and shear on the physis. More than 90% of affected patients who are treated with rest for an average of 3 months become asymptomatic. Prevention is the best option. Set limitations of the number of pitches and types of pitches depending on the age of the player. Also recommend use of proper pitching mechanics.
Question 84
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 480.
Question 85
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Explanation
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 86
Figure 1 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snowboarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in

Explanation
Question 87
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of Review Topic
Explanation
Question 88
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 89
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.
Question 90
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 91
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 92
A 36-year-old professional baseball player reports the acute onset of severe right groin pain while attempting to avoid being hit by a baseball while at bat. Examination reveals tenderness, soft-tissue swelling, and ecchymosis in the right groin extending over the medial thigh. MRI scans are shown in Figures 8a and 8b. Management should consist of
Explanation
REFERENCES: Gilmore J: Groin pain in the soccer athlete: Fact, fiction, and treatment. Clin Sports Med 1998;17:787-793.
Irshad K, Feldman LS, Lavoie C, et al: Operative management of “hockey groin syndrome”:
12 years of experience in National Hockey League players. Surgery 2001;130:759-766.
Question 93
Which of the following is true regarding changes in the vascularity of the adult intervertebral disc with age? Review Topic
Explanation
The intervertebral disc is composed of an outer structure called the annulus fibrosis and an inner structure called the nucleus pulposus. The annulus fibrosis is composed
of type 1 collagen, water, and proteoglycans. The inner nucleus pulposus is composed of type 2 collagen, water, and proteoglycans. Intervertebral discs are avascular with capillaries terminating at the end plates. The nucleus pulposus receives nutrition primarily through diffusion through blood vessels within the endplate.
Roberts et al. review the histology and pathology of the intervertebral disc. They note that at birth, the cartilagenous end plates have large vascular channels through them as well as vascular channels through the annulus. Soon after birth, these vascular channels close with none remaining at the end of the first decade of life. However, with age, more blood vessels grow into the disc from the outer annulus fibrosis in response to degenerative changes.
Illustration A is a diagram of the vascular supply in an adult intervertebral disc. Incorrect Answers:
Question 94
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
REFERENCES: Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 95
Chemotherapy is routinely included in the treatment of which of the following soft-tissue sarcomas?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Rhabdomyosarcoma, in Soft Tissue Tumors, ed 3. St Louis, MO, CV Mosby, 1995, p 539.
Hays DM: Rhabdomyosarcoma. Clin Orthop 1993;289:36-49.
Question 96
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 97
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30° of flexion, which decreases as the knee is flexed to 90°. What is the most likely diagnosis?
Explanation
REFERENCES: Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 98
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, Ogose A (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 99
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 100
- The radiographs shown in Figures 71a through 71c, and the CT scan shown in Figure 71d reveal an acetabular fracture that should be classified as
Explanation
Note the classic “Spur Sign” seen in these radiographs. This is pathognomonic of a both-column fracture of the acetabulum.
The other defining feature of the both column fx (as evident by these films) is that there is no intact acetabulum connected to the bone fragment which is connected to the ipsilateral SI joint.
