Orthopedic MCQ Exam: Fracture, Hip & Knee Practice Questions | Part 76

Key Takeaway
This page presents Part 76 of a high-yield MCQ bank for orthopedic surgeons and residents. Designed by Dr. Mohammed Hutaif, it offers 100 verified, exam-formatted questions replicating OITE and AAOS board exams. Master Fracture, Hip, and Knee topics through interactive study and exam modes to ensure successful board certification.
About This Board Review Set
This is Part 76 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 76
This module focuses heavily on: Fracture, Hip, Knee.
Sample Questions from This Set
Sample Question 1: Back pain and ipsilateral knee pain are common long-term sequelae of hip arthrodesis. To limit these problems, what position should be avoided during fusion of the hip?...
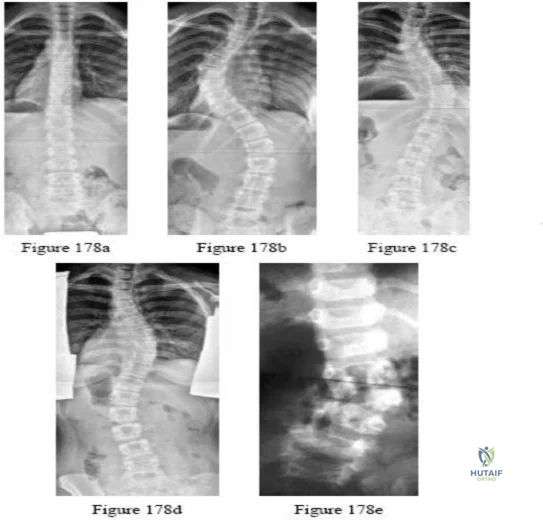
Sample Question 2: -Figures a and b are the posteroanterior and lateral radiographs of a 13-year-old girl with a progressive curve despite bracing with a thoracolumbosacral orthosis. Examination reveals no pain or neurologic findings. The lumbar curve measure...
Sample Question 3: Biomechanical in vitro studies of double-row anchor fixation of rotator cuff tears show what initial advantage over single-row anchor fixation? Review Topic...
Sample Question 4: Which of the following factors is associated with improved outcomes following surgery for hip fractures?...
Sample Question 5: Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progre...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Back pain and ipsilateral knee pain are common long-term sequelae of hip arthrodesis. To limit these problems, what position should be avoided during fusion of the hip?
Explanation
REFERENCES: Callaghan JJ, Brand RA, Pederson DR: Hip arthrodesis: A long-term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Callaghan JJ, McBeath AA: Arthrodesis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 749-759.
Question 2
-Figures a and b are the posteroanterior and lateral radiographs of a 13-year-old girl with a progressive curve despite bracing with a thoracolumbosacral orthosis. Examination reveals no pain or neurologic findings. The lumbar curve measures 59 degrees and the thoracic curve measures 52 degrees.The most appropriate treatment is

Explanation
Question 3
Biomechanical in vitro studies of double-row anchor fixation of rotator cuff tears show what initial advantage over single-row anchor fixation? Review Topic
Explanation
Question 4
Which of the following factors is associated with improved outcomes following surgery for hip fractures?
Explanation
Question 5
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of

Explanation
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an infection, and revascularization is not indicated.
Question 6
A patient sustained a puncture wound to the plantar aspect of his foot. He was wearing shoes and socks at the time of the injury. Systemic antibiotic administration with specific coverage for which bacterial species (in addition to Staphylococcus aureus) should be instituted?
Explanation
Puncture wounds sustained through a shoe and sock increase risk for Pseudomonas infection. Clostridium are associated with soil-contaminated wounds. Mycobacterium marinum is associated with injuries sustained within water.
RECOMMENDED READINGS
DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. View Abstract at PubMed
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
Question 7
He is intubated and being resuscitated. The calf is very swollen with compartment pressures: anterior 25 mm Hg, lateral 24 mm Hg, deep posterior 21 mm Hg, and
Explanation
Question 8
Which of the following is most important to acheive a good outcome following a Syme amputation?

Explanation
Question 9
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of
Explanation
REFERENCES: Hamer AJ, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood. J Bone Joint Surg Br 1984;66:770-771.
Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1077-1135.
Question 10
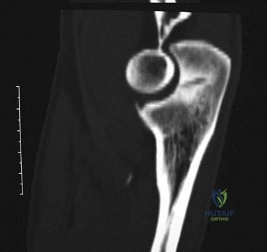
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 11
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?
Explanation
REFERENCES: Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
McCarty EC, Warren RF, Deng XH, et al: Temperature along the axillary nerve during radiofrequency-induced thermal shrinkage. Am J Sports Med 2004;32:909-914.
Question 12
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?
Explanation
REFERENCES: Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207.
Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 13
A patient presenting with scapulothoracic dissocation and ipsilateral extremity neurologic injury is most likely to have which of the following outcomes?

Explanation
The referenced study by Althausen et al found that outcomes from this injury were: a flail extremity in 52%, early amputation in 21%, and death in 10%.
The other referenced study by Ebraheim et al found that 12/15 patients had a complete brachial plexus injury and that none recovered any function (the other 3 patients died in the acute period).
Question 14
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 15
The condition seen in Figure 60 is attributable to

Explanation
Cephallomedullary implants for treatment of proximal femur fractures have gained in popularity over the last decade. Although these implants have improved outcomes for certain fracture types, multiple complications are associated with this implant. Failure may occur secondary to implant design (for example, mismatch of curvature of the nail to the femur, which can result in distal anterior cortical perforation).
RECOMMENDED READINGS
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013 Jun;27(6):303-7. doi: 10.1097/BOT.0b013e318283f24f. PubMed PMID: 23287752.
View Abstract at PubMed
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000093. doi: 10.1002/14651858.CD000093.pub4. Review. Update
in: Cochrane Database Syst Rev. 2010;(9):CD000093. PubMed PMID: 18646058. View Abstract at PubMed
Question 16
A patient underwent a right hip arthroscopy, CAM resection, and labral repair while positioned supine on a fracture table with a perineal post. The leg was in traction for 4 hours, and no intrasurgical complications were noted. At the 2-week follow-up appointment, the patient was experiencing numbness and tingling in the perineum on the surgical side and noted pain predominantly while sitting. What is the likely cause of these symptoms?
Explanation
Although all of these responses are known complications related to hip arthroscopy, the symptoms of perineal numbness and pain associated with prolonged traction time indicate a compression injury to the pudendal nerve against the perineal post used to provide counter traction. Perineal numbness usually occurs on the surgical side, with pain in the area of the anus to the penis/clitoris. Pain is predominantly experienced while sitting, but is relieved when sitting on a toilet. Pain can be relieved with a diagnostic pudendal nerve block. This injury is not unique to hip arthroscopy; it also is described in the trauma literature. To prevent compression-type injuries, a well-padded post larger than 9 cm in diameter should be positioned against the medial thigh. Traction force should be kept to a minimum and the
extremity positioned in slight abduction. Continuous traction time should not exceed 2 hours, with intermittent traction used during prolonged procedures.

Question 17
An injury to the axillary nerve would result in deltoid muscle weakness. 5 . An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging.

Explanation
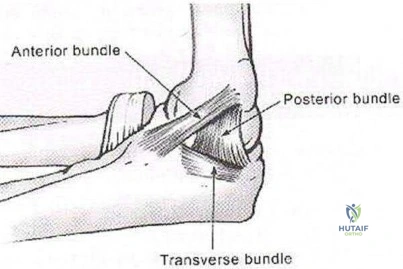
The medial ulnar collateral ligament, or medial collateral ligament of the elbow, is composed of three bundles: an anterior bundle, a posterior bundle, and a variable
transverse oblique bundle. During late cocking and early acceleration phases of the overhead throw, the medial UCL is subjected to the greatest amount of valgus stress to the elbow. During this phase, the forearm lags behind the upper arm and generates valgus stress while the elbow is primarily dependent on the anterior band of the UCL for stability. This puts the ligament at greatest risk of injury during this phase.
Fleisig et al. examined the kinetics of baseball pitching and the implications on injury mechanisms. They showed that the UCL contributes to 54% of the varus torque that is generated during the early acceleration of throwing. The position of greatest load occurred when the arm was flexed to 95 +/14 degrees with an applied valgus load.
Illustration A shows a diagram of the medial ulnar collateral ligament ligament bundles. Incorrect Answers:
A 14-year-old elite basketball player develops acute medial elbow pain after a fall. Physical examination reveals medial elbow tenderness over the submlime tubercle, but full range of motion. The provocative tests seen in Figure A exacerbate his elbow pain. Radiographs of the elbow are normal. What would be the next best step in treatment?
Supervised elbow stretching program Therapeutic elbow arthroscopy

Static elbow external fixation for 3 to 6 weeks, then MR arthrography if pain continues Activity avoidance for 6 weeks

Serial inflammatory markers and rheumatology referral
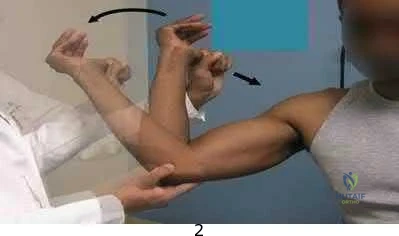
Figure A shows a moving valgus stress, which is a provocative test for ulnar collateral ligament (UCL) injury and elbow valgus instability. The initial treatment would be a short period of immobilization, rest and flexor pronator strengthening in this patient population.
Adolescent UCL injuries can be effectively treated with a short period of rest and NSAIDs to control pain. As the acute inflammation resolves, the patient can be started on a supervised therapy program. This should target flexor pronator muscles, as they are important secondary dynamic stabilizers of valgus stress. Once symptoms have improved and the athlete has regained full range of motion and strength, a mediated throwing program may be initiated. Throwing athletes should be educated to avoid provocative activities during this period.
Chen et al. wrote a JAAOS article on shoulder and elbow injuries in the skeletally immature athlete. They state that surgery is reserved for older athletes with persistent valgus instability despite > 6 months of non-surgical management.
Murthi et al. reviewed recurrent elbow instability. They state the anterior bundle of the medial ulnar collateral ligament complex is the primary valgus stabilizer of the elbow. The anterior band is taut for the first 60° of elbow flexion, and the posterior band is taut from 60° to 120° of flexion. The secondary valgus stabilizers of the elbow joint include the radial head, the anterior and posterior aspects of the capsule, and the muscular forces around the joint.
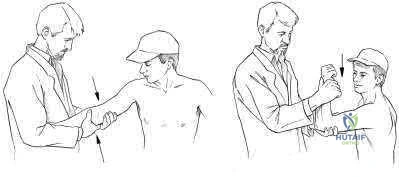
Figure A is showing a moving valgus stress. Illustration A shows provocative tests for valgus instability of the elbow. The image on the left shows a valgus stress test. This assesses the anterior bundle of the medial ulnar collateral ligament complex by flexing the elbow to 25-30 degrees and applying a valgus load across the elbow. The image on the right shows milking maneuver. This assesses the posterior bundle of the medial ulnar collateral ligament complex by pulling on the

beyond 90°. Incorrect Answers:
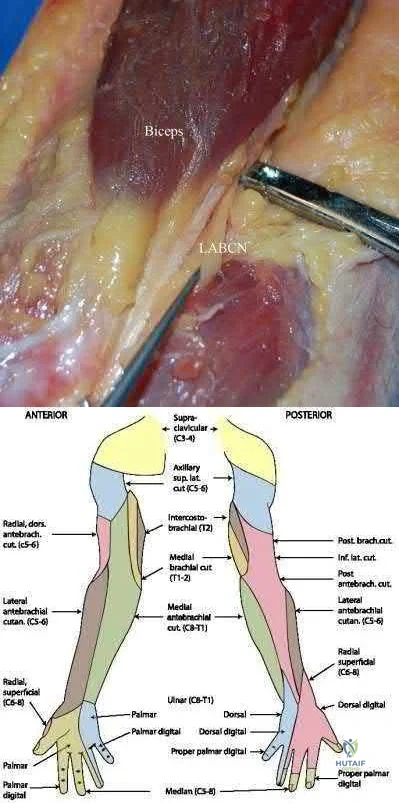
A young, healthy male undergoes a distal biceps repair and sustains an iatrogenic nerve injury during the procedure. Which of the following clinical findings are most likely to be seen in this circumstance? Inability to extend the thumb

Lateral volar forearm numbness Inability to flex the middle finger Medial volar forearm numbness Dorsal thumb numbness
The most commonly injured nerve during a distal biceps repair is the lateral antebrachial cutaneous nerve (LABCN). Injury to this nerve would result in lateral volar forearm numbness.
Distal biceps avulsions can be partial or complete. Indications for surgical management include young, healthy patients who do not wish to sacrifice function, as well as partial biceps avulsions that do not respond to conservative management. Repair of a distal biceps avulsion can be approached through either an anterior one-incision technique or a two-incision technique (BoydAnderson). The one-incision technique uses the interval between the brachioradialis (radial nerve) and pronator teres (median nerve), while the two-incision technique uses this same interval in addition to a second posterolateral elbow incision. The lateral antebrachial cutaneous nerve is the most common nerve injured during either approach.
Kelly et al. retrospectively reviewed 74 distal biceps tendon repairs, and found five sensory nerve paresthesias. The lateral antebrachial cutaneous nerve was most commonly injured, followed by the superficial radial nerve.
Cain et al. retrospectively reviewed 198 distal biceps tendon repairs, and found a 36% complication rate. Lateral antebrachial cutaneous nerve paresthesias were found in 26%, while radial sensory nerve paresthesias were found in 6%, and posterior interosseous nerve (PIN) injury in 4%.
Illustration A shows the close relationship between the lateral antebrachial cutaneous nerve (LABCN) and the distal biceps. Illustration B shows the sensory nerves of the upper extremity and their respective areas of innervation.
Incorrect Answers:
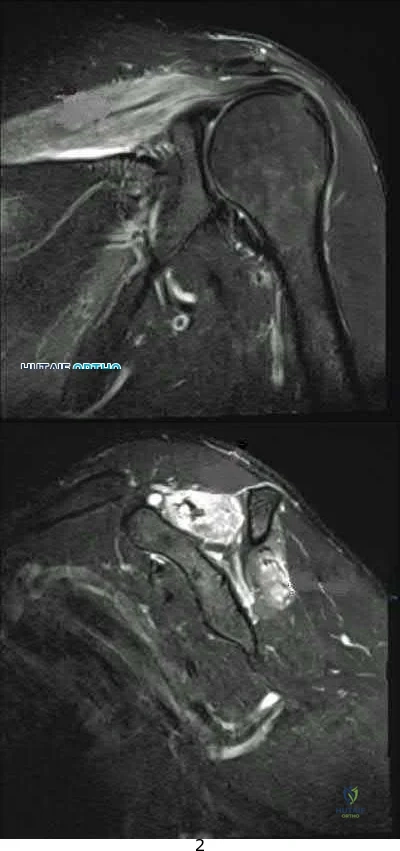
A 33-year-old female presents with left shoulder weakness. Two weeks prior to presentation, the patient experienced sudden-onset, left shoulder pain, which occurred a few days after receiving the influenza vaccine. The pain subsided over the next day, followed by gradual weakness of her shoulder and eventual general disuse of her left upper extremity. An initial visit to her primary care provider resulted in the recommendation of observation. On physical exam, there is weakness and gross atrophy of the shoulder girdle. Figures A & exhibit T2-weighted MRI images of her left shoulder. To further confirm her suspected diagnosis, she is sent for electromyography.
What is the expected result?
Normal results
Fibrillation potentials consistent with compression at the spinoglenoid notch 3 . Sharp waves and fibrillations potentials associated with the deltoid and biceps

Acute denervation of both peripheral nerve and nerve root distribution with sharp waves and fibrillation potentials

Early reinnervation with polyphasic motor unit potentials
This patient has Parsonage-Turner Syndrome, which, when tested on EMG during the first 3 weeks, exhibits acute denervation of both peripheral nerve and nerve root distributions with positive sharp waves and fibrillation potentials.
Parsonage-Turner Syndrome is an idiopathic disorder with an etiology that is still unknown. Typical antecedent events can involve a viral illness, recent immunization, or elective surgery. Clinical presentation is usually initiated by acute onset shoulder pain, which quickly subsides and is followed by gradual weakness. Early MRI exhibits edema in the effected muscles, and fatty infiltration in later stages. Treatment is typically non-operative, and resolution can be seen as early as 6 weeks from onset.
Tjoumakaris et al. provide a thorough review of the diagnosis and management of ParsonageTurner Syndrome. The authors report the usefulness of MRI, which exhibits early edema and later fatty infiltration in the affected muscles, and urge the use of EMG as a confirmatory diagnostic measure as well as a monitoring tool to track resolution. Early identification and diagnosis may be treated with a short course of steroids, which may help shorten symptoms.
Stutz et al. concisely summarize Parsonage-Turner Syndrome and provide typical presentation, diagnosis and management principles. The authors note the common association with viral illness and/or recent immunization along with the importance of obtaining a baseline chest radiograph to rule out a compressive Pancoast tumor. Management is typically supportive with eventual resolution.
Figures A, B, and C are T2-weighted coronal, sagittal, and axial cuts of the shoulder girdle with associated edema in the supraspinatus and infraspinatus typically seen in Parsonage-Turner Syndrome.
Incorrect answers:
A total shoulder arthroplasty (TSA) would be the most appropriate treatment in which of the following arthritic patients?
Question 18
A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include
Explanation
REFERENCES: Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1120-1128.
Coe JD, Warden KE, Sutterlin CE, et al: Biomechanical evaluation of cervical spinal stabilization methods in a human cadaveric model. Spine 1989;14:1122-1131.
Question 19
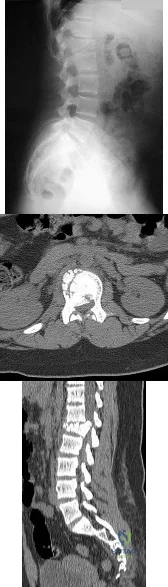
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
REFERENCES: McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 20
What adaptations occur in the dominant shoulder of throwers compared to their nondominant shoulder? Review Topic
Explanation
Question 21
Compared with surgically treated patients, patients with extra-articular distal third humeral shaft fractures that are treated nonsurgically with functional bracing can be expected to show which of the following findings?
Explanation
Question 22
All of the following conditions are associated with the female athlete triad EXCEPT? Review Topic
Explanation
The female athlete triad is an interrelationship of menstrual dysfunction (i.e., amenorrhea or oligomenorrhea), low energy availability (insufficient caloric intake for demand, with or without an eating disorder) and decreased bone mineral density. It is relatively common among young women participating in sports. More recently, it has been suggested that endothelial dysfunction also results, due to an imbalance between vasodilating and vasoconstricting agents triggered from inappropirate levels of nitric oxide on the microscopic level, which predisposes these women to atherosclerotic changes and increases their risk of cardiovascular disease in the future.
Matheson et al. analyzed cases of 320 athletes with bone scan-positive stress fractures (M = 145, F = 175) seen over 3.5 years and assessed the results of conservative management. They found that conservative treatment of stress fractures in athletes is satisfactory in the majority of cases.
Constantini et al. evaluated the prevalence of vitamin D insufficiency and deficiency among young athletes and dancers. They found a higher rate of vitamin D insufficiency among participants who practice indoors, during the winter months, and in the presence of iron depletion.
Nazem et al. reviewed the major components and health consequences of the female athlete triad as well as strategies for diagnosis and treatment of the conditions. They concluded that treatment requires a multidisciplinary approach involving health care professionals as well as coaches and family members.
Yagi et al. followed 230 runners participating in high school running teams for a total of 3 years to report occurrence of medial tibial stress syndrome (MTSS) and stress fracture. Predictors of MTSS and stress fracture were investigated. The authors reported a significant relationship between BMI, internal hip rotation angle and MTSS infemales.
Incorrect Answers:
Question 23
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include Review Topic
Explanation
Question 24
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
REFERENCES: Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 25
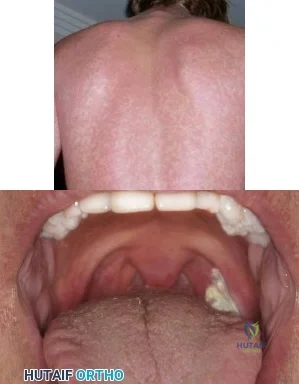
A 19-year-old football player is taken off the field because of fatigue. Examination reveals a rash shown in Figure A. Oral examination reveals findings shown in Figure B. Posterior cervical glands are palpable. A mass is palpable in the left upper quadrant. Which of the following is true regarding the most likely diagnosis? Review Topic
Explanation
IM is caused by the Epstein-Barr virus (EBV). Annual incidence is 1-3% in college freshmen. It is characterized by Hoagland's triad (fever, pharyngitis, lymphadenopathy). Some have rash and splenomegaly. Splenic rupture is rare (0.1-0.2% of patients). It is caused by sudden increase in portal venous pressure from a simple Valsalva maneuver or from external trauma. The risk of rupture is highest in the first 3 weeks of illness.
Putukian et al. reviewed IM and athletic participation. They recommend return to LIGHT activity after 3 weeks from symptom onset when the athlete is afebrile, has a good energy level, and does not have any significant associated abnormalities. They recommend returning to CONTACT sports after at least 3 weeks when the athlete has no remaining clinical symptoms, is afebrile, and has a normal energy level.
Jaworski et al. discussed infectious diseases in athletes. They state that splenic rupture occurs because of lymphocytic infiltration that distorts the support structure of the spleen, leading to fragility. They recommend return to light, non-contact activities once the athlete is afebrile and appropriately hydrated, fatigue has improved, and a minimum period of 3 weeks has passed from symptom onset.
Figure A shows a petechial rash, which can be seen in IM. Amoxicillin increases the risk of rash. Figure B shows unilateral exudative pharyngitis. The left tonsil is
covered
by
a
white
exudate/pseudomembrane.
Incorrect
Question 26
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?
Explanation
REFERENCES: Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacment and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 27
A 24-year-old dancer reports posterior ankle pain when in the “en pointe” position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Question 28
One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?
Explanation
Dysphagia after anterior cervical diskectomy and fusion is a common, usually transient finding after anterior cervical approaches to the spine. While it has been reported to occur in up to 70% of patients 2 weeks following surgery, in most cases the symptoms quickly resolve. There is, however, a small subset of patients for whom symptoms of dysphagia will persist. Lee and associates prospectively studied the rate of dysphagia after anterior cervical diskectomy and fusion, reporting a 15% rate of dysphagia at 12 months, and 12% at 24 months. Phillips and associates analyzed the 2-year data from the PCM FDE clinical trial and found a 12.1% incidence of dysphagia in the ACDF arm.
RECOMMENDED READINGS
Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study. Spine J. 2007 Mar-Apr;7(2):141-7. Epub 2007 Jan 22. PubMed PMID: 17321961. View Abstract at PubMed
Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004 Jul 1;29(13):1441-6. PubMed PMID: 15223936. View Abstract at PubMed
Edwards CC 2nd, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST, Riew KD. Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am. 2004 Feb;86-A(2):251-6. PubMed PMID: 14960668. View Abstract at PubMed
Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC. A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine (Phila Pa 1976). 2013 Jul 1;38(15):E907-18. doi: 10.1097/BRS.0b013e318296232f.
Rihn JA, Kane J, Albert TJ, Vaccaro AR, Hilibrand AS. What is the incidence and severity of dysphagia after anterior cervical surgery? Clin Orthop Relat Res. 2011 Mar;469(3):658-65. PMID: 21140251.View Abstract at PubMed
Question 29
Mechanical reduction of the pain associated with the condition shown in Figure 6 can be accomplished through the use of a cane on the contralateral side. Similarly, if this patient must carry any type of load in his or her arms, it should be carried
Explanation
REFERENCE: Tan V, Klotz MJ, Greenwald AS, Steinberg ME: Carry it on the bad side! Am J Orthop 1998;27:673-677.
Question 30
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty? i. Infection
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
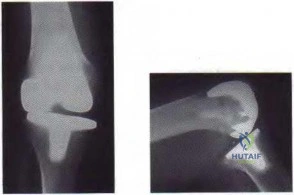
Figure 59a Figure 59b
Question 31
The initiating cellular event in development of posttraumatic osteoarthritis is attributed to which of the following?
Explanation
Question 32
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 33
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?

Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 34
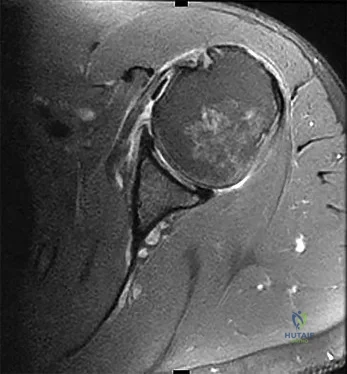
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of
Explanation
REFERENCE: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 35
A 25-year-old patient presents with a posterior wall/ posterior column acetabular fracture. She is scheduled for open reduction internal fixation through a posterior approach. What position of the leg exerts the least amount of intraneural pressure on the sciatic nerve?

Explanation
Question 36
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of
Explanation
REFERENCES: Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Indelicato PA: Injury to the medial capsuloligamentous complex of the knee, in Feagin J (ed): The Crucial Ligaments, ed 2. 1994, pp 351-360.
Question 37
A 68-year-old male presents with gait instability, clumsiness of the hands, and the MRI images shown in Figure A. You decide to proceed with surgical decompression. When planning your surgical treatment, it is important to note that compared to a posterior approach, the anterior procedure has: Review Topic

Explanation
Cervical myelopathy has a progressive course and therefore if there is evidence of functional impairment surgical decompression is indicated. Either an anterior decompression or posterior decompression can be used depending on a variety of factors including number of levels involved and sagittal alignment of the cervical spine. In general, a posterior approach is used when three or more levels are involved and the spine is in neutral or lordotic alignment.
Fehlings et al. did a prospective study on the risks of complications associated with surgical treatment of cervical myelopathy. They found that combined anterior and posterior procedures had a significantly higher rate of complication than either anterior-only or posterior-only procedures. Posterior procedures had a higher rate of wound infections compared to anterior. They found no statistical difference in the over-all complication rate, incidence of C5 radiculopathy, or dysphagia between an anterior-only or posterior-only procedure.
Fehlings et al. did a prospective study on outcomes following surgical treatment of cervical myelopathy. At one year follow-up they found a significant improvement in mJOA score, Nurick grade, NDI score, and all SF-36v2 dimensions. With the exception of mJOA scores, these improvements were not statistically related to severity of disease.
Liu et al. performed a meta-analysis of outcomes following surgical decompression of cervical myelopathy. They found outcomes following anterior procedures were better than those for posterior procedures when there were less than 3 affected levels. With 3 or greater levels, no statistical difference in outcomes could be found between the two approaches. They note none of their reviewed publications represent high-quality prospective randomized trials.
Figure A is a sagittal MR image of the cervical spine showing multi-level degenerative disease with cord compression consistent with cervical myelopathy.
Incorrect Answers:
Question 38
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?
Explanation
REFERENCES: Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
Oestreich AE, Mize WA, Crawford AH, et al: The “anteater nose”: A direct sign of calcaneonavicular coalition on the lateral radiograph. J Pediatr Orthop 1987;7:709-711.
Question 39
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
REFERENCES: Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 40
A 30-year-old accountant and recreational softball player, who is seen at the end of his baseball season, reports a several month history of pain along the medial side of his dominant elbow. He cannot identify a specific injury and notes it only hurts when he throws the ball in from the outfield. Besides the pain, he remarks that his speed and distance while throwing have diminished considerably. Examination reveals tenderness along the medial elbow but no weakness or gross instability is found. Radiographs are normal. Based on the history, what is the most likely diagnosis? Review Topic
Explanation
the forearm during resisted forearm pronation and is not associated with the throwing motion in particular. Valgus extension overload may mimic medial collateral ligament injury, not varus extension injuries. Medial epicondylitis may be confused with ligament insufficiency but the examination and a history of pain only while throwing make this an unlikely diagnosis.
Question 41
Which of the following is considered a contraindication to functional bracing for the treatment of humeral shaft fractures?
Explanation
1) massive soft-tissue or bone loss; 2) an unreliable or noncompliant patient; and 3) an inability to maintain acceptable fracture alignment of up to 20 degrees of anterior or posterior angulation, 30 degrees of varus or valgus angulation, and greater than 3 cm of shortening.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Sarmiento A. Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-486.
Question 42
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
Explanation
REFERENCE: Noble AR, Branham D, Willis M, et al: Mechanical effects of the extended trochanteric osteotomy. J Bone Joint Surg Am 2005;87:521-529.
Question 43
A 32-year-old woman has had progressive left foot pain over the first metatarsophalangeal (MTP) joint. Footwear is becoming problematic. There is full range of motion of the first MTP with medial eminence pain. Her weightbearing radiograph reveals a hallux valgus angle (HVA) of 35 degrees and a 1-2 intermetatarsal angle (IMA) of 10 degrees. What is the best next step?
Explanation
Patients with painful progressive hallux valgus are surgical candidates. Presurgical evaluation includes radiographic examination. The IMA between the first and second metatarsals as well as the HVA must be measured. If the IMA is smaller than 15 degrees and the HVA is smaller than 35 degrees, a distal osteotomy is preferred. Distal soft-tissue reconstruction is only useful for IMAs smaller than 11 degrees and HVAs smaller than 25 degrees. Proximal osteotomies and the Lapidus bunionectomy are reserved for larger hallux valgus deformities with IMAs exceeding 15 degrees and HVAs exceeding 35 degrees.
RECOMMENDED READINGS
Pentikainen I, Ojala R, Ohtonen P, Piippo J, Leppilahti J. Distal Chevron Osteotomy: Preoperative Radiological Factors Contributing to Long-Term Radiological Recurrence of Hallux
Valgus. Foot Ankle Int. 2014 Sep 5. pii: 1071100714548703. [Epub ahead of print] PubMed PMID: 25192724. View Abstract at PubMed
Fakoor M, Sarafan N, Mohammadhoseini P, Khorami M, Arti H, Mosavi S, Aghaeeaghdam A. Comparison of Clinical Outcomes of Scarf and Chevron Osteotomies and the McBride Procedure in the Treatment of Hallux Valgus Deformity. Arch Bone Jt Surg. 2014 Mar;2(1):31-
Question 44
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Loebenberg MI, Plate AM, Zuckerman JD: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 45
The most common reason for proximal femur fracture fixation failure (Figure 15) is secondary to which common deformity?

Explanation
Malposition of a proximal lag screw may result in cut-out similar to that seen with a sliding hip screw. Varus malreduction also can result in implant failure. Studies have shown no difference in complication or healing rates when comparing short and long cephallomedullary nails.
RECOMMENDED READINGS
Kleweno C, Morgan J, Redshaw J, Harris M, Rodriguez E, Zurakowski D, Vrahas M, Appleton
P. Short versus Long Cephalomedullary Nails for the Treatment of Intertrochanteric Hip Fractures in Patients over 65 Years. J Orthop Trauma. 2013 Nov 13. [Epub ahead of print] PubMed PMID: 24231580.View Abstract at PubMed
Haidukewych GJ. Intertrochanteric fractures: ten tips to improve results. Instr Course Lect. 2010;59:503-9. Review. PubMed PMID: 20415401. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 20
A 23-year-old man sustains multiple injuries in a high-speed motor vehicle collision. Among his injuries are a right transverse-posterior wall acetabular fracture, a left open tibia fracture with compartment syndrome, and a right calcaneus fracture.
Question 46
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate
in patients with anterior knee pain.
Question 47
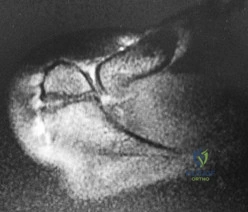
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of Review Topic
Explanation
Question 48
A 14-year-old boy has had a 3-month history of low back pain with no known trauma. The pain is worse with activity and relieved by rest, although he does report difficulty with prolonged sitting in school. The patient was on the football team but stopped participating because of the back pain during football practice. He reports no history of radicular pain and denies any numbness, tingling, or weakness in the legs. Neurologic examination is normal. Back examination reveals slight tenderness over the lower back area but no swelling or skin defects. Strength testing is 5 over 5 in the lower extremities and the straight leg raise test is negative. Back range of motion is nearly full, but back extension is painful. The hamstrings are slightly tight. Initial radiographs, including AP, lateral and oblique views, are negative. What is the best test to determine the patient's diagnosis? Review Topic
Explanation
have no role in the evaluation of the patient who presents with classic spondylolysis-type symptoms. The most sensitive physical examination finding is pain with back extension. Oblique radiographs can be obtained, but they are not as sensitive or specific as a bone scan with SPECT. The patient does not have any signs of a disk problem; therefore, an evaluation of the disk is not helpful.
(SBQ13PE.79) A 17-year-old male American football lineman presents with low back pain of insidious onset that is somewhat worse with activity. He has no neurologic complaints, night pain or fevers. His symptoms have been present for a few years but this is the first time he has sought medical attention. What physical examination finding is most likely to be found in this clinical scenario? Review Topic
Popliteal angle of 5 degrees
Heel cord tightness
Increased femoral anteversion
Pain with lumbar extension in single leg stance
Numbness of the skin of the anterolateral calf and dorsum of the foot
The patient demographics and clinical presentation are consistent with lumbar spondylolysis. Pain with lumbar extension is the most common physical exam finding.
Office assessment of the patient with spondylolysis should note pertinent negatives that would signify other causes of back pain. The history is most commonly negative for neurologic symptoms such as weakness or numbness, although patients will occasionally have radicular pain. On exam, patients may have localized spasm or tenderness, step off (if there is spondylolisthesis), hamstring tightness. The most common finding is pain with lumbar extension.
McCleary et al. review the diagnosis and treatment of spondylolysis in athletes. They identify three types of patients with spondylolysis: (1) female dancer or gymnast who is hyperlordotic, with increased motion and flexibility, (2) male weightlifter or football player undergoing a growth spurt, with decreased motion and flexiblity, especially of the spinal erectors, and (3) a novice athlete undergoing vigorous preparation for a new sport, with poor core strength and flexibility.
Incorrect
Question 49
A large circumferential proximal femoral allograft is to be used in the reconstruction of a failed femoral component in a total hip arthroplasty. To enhance fixation of the graft to the implant, which of the following strategies should be used?
Explanation
REFERENCES: Allan DG, Lavoie GJ, Rudan JF, et al: The use of allograft bone in revision total hip arthroplasty, in Friedlaender GE, Goldberg VM (eds): Bone and Cartilage Allografts: Biology and Clinical Applications. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1991, pp 263-264.
Gross AE, Lavoie MV, McDermott P, Marks P: The use of allograft bone in revision of total hip arthroplasty. Clin Orthop 1985;197:115-122.
Head WC, Berklacich FM, Malinin TI, Emerson RH Jr: Proximal femoral allografts in revision total hip arthroplasty. Clin Orthop 1987;225:22-36.
Question 50
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
REFERENCES: Denis F, Davis S, Comfort T: Sacral fractures: An important problem.
A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.
Wood KB, Denis F: Fractures of the sacrum and coccyx, in Vacarro AR (ed): Fractures of the Cervical, Thoracic and Lumbar Spine. New York, NY, Marcel Dekker, 2003, pp 473-488.
Question 51
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic
Explanation
Question 52
- Radiographs of the cervical spine of a 73-year-old man who fell down stairs reveal cervical spondylosis without evidence of fracture or dislocation. MRI and CT scans are consistent with the plain radiographs. After 72 hours, neurologic evaluation reveals intact sensation; however, weakness of the upper extremities is greater than that of the lower extremities. What is the most likely diagnosis?
Explanation
extremity deep pressure and proprioceptive preserved. 3-Posterior cord syndrome is rare with loss of deep pressure, deep pain, and proprioception. 4-Brown-Sequard syndrome-Uncommon-Ipsilateral motor deficit, contralateral pain and temperature deficit. 5-Cervical nerve root injury- functional impairment of the cervical spine. Symptoms are often acute and severe, dependent on the level of the lesion. An infraforaminal protrusion may compress only the spinal root ganglion resulting in severe brachialgia with paresthesia and numbness but with little or no motor involvement.
Question 53
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
Explanation
REFERENCES: Chiu WC, Haan JM, Cushing BM, et al: Ligamentous injuries of the cervical spine in unreliable blunt trauma patients: Incidence, evaluation, and outcome. J Trauma 2001;50:457-463.
Sanchez B, Waxman K, Jones T, et al: Cervical spine clearance in blunt trauma: Evaluation of a computed tomography-based protocol. J Trauma 2005;59:179-183.
Nunez D Jr: Value of complete cervical helical computed tomographic scanning in identifying cervical spine injury in the unevaluable blunt trauma patient with multiple injuries:
A prospective study. J Trauma 2000;48:988-989.
Question 54
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
REFERENCES: Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.
Question 55
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow? Review Topic

Explanation
Question 56
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Explanation
REFERENCE: Mann RA, Coughlin MJ: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 174.
Question 57
Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve A B C D

Explanation
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
RECOMMENDED READINGS
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. View Abstract at PubMed
Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.View Abstract at PubMed
RESPONSES FOR QUESTIONS 86 THROUGH 89
Proximal junctional kyphosis (PJK)
Adjacent segment degeneration
Intraoperative neurological injury
Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
Question 58
A 9-year-old boy sustained a traumatic brain injury and right lower extremity trauma in an accident involving a motor vehicle and a pedestrian. Initial evaluation in the emergency department reveals an obtunded patient who is breathing spontaneously and withdraws appropriately to painful stimuli. After initial resuscitation and stabilization, a CT scan reveals a right parietal intracranial hemorrhage. Radiographs of the swollen right thigh are shown in Figures 32a and 32b. Management of the fractured femur should ultimately consist of
Explanation
35 patients with head injury. In one patient with hemiplegia and a urinary tract infection, a deep wound infection developed, necessitating nail removal. The remaining patients all healed without major complications. Heinrich and associates treated 78 diaphyseal femoral fractures with flexible intramedullary nails, including 14 with head injury. No major complications were reported and all fractures healed.
REFERENCES: Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996,
pp 83-95.
Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Heinrich MS, Drvaric DM, Darr K, et al: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J Pediatric Orthop 1994;14:501-507.
Canale ST, Tolo VT: Fractures of the femur in children. Instr Course Lect 1995;44:255-273.
Question 59
A 75-year-old woman notes a slowly enlarging mass in the right anterior thigh. Her medical history is significant only for hypertension. An MRI scan of her thigh is shown in Figures 60a through 60d. Which of the following surgical margins is the most appropriate for removal of this lesion?
Explanation
REFERENCES: Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 60
below shows the radiograph obtained from a year-old woman who has sharp pain in her groin, thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best to proceed. What is the best next step?
Explanation
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the
injection.
Question 61
What is the main mechanism for nutrition of the adult disk?
Explanation
REFERENCES: Biyani A, Andersson GB: Low back pain: Pathophysiology and management. J Am Acad Orthop Surg 2004;12:106-115.
Urban JG, Holm S, Maroudas A, et al: Nutrition of the intervertebral disc: Effect of fluid flow on solute transport. Clin Orthop 1982;170:296-302.
Park AE, Boden SD: Intervertebral disk: Form and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 62
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
Question 63
In the injury shown in Figures 1 and 2, what ligament remains intact?

Explanation
Perilunate dislocations result from high-energy injuries to the extended wrist. The injury shown is a lunate dislocation. Two classification systems have been described, the Mayfield system and the Herzberg system. Mayfield described the four stages of progressive ligamentous instability following injury. In stage I, the radioscaphocapitate and scapholunate ligaments fail. Stage II involves dislocation of the lunocapitate joint, usually a dorsal dislocation of the capitate. In stage III, the lunotriquetral ligament fails. In stage IV, the dorsal radiocarpal ligament is torn, and the lunate dislocates volarly. The short radiolunate ligament is the only ligament that remains intact, resulting in rotation of the lunate volarly. Herzberg and associates further classified perilunate dislocations as stage I injuries and lunate dislocations as stage II injuries. Lunate dislocations were further classified into stage IIA, in which the lunate exhibits rotation less than 90°, and stage IIB, in which the lunate exhibits rotation greater than 90°. The radiographs represent a Mayfield stage IV, Herzberg stage IIA injury.
Question 64
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 65
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
REFERENCES: Sady SP, Wortman M, Blanke D: Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil 1982;63:261-263.
Tanigawa MC: Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys Ther 1972;52:725-735.
Wallin D, Ekblom B, Grahn R, Nordenberg T: Improvement of muscle flexibility: A comparison between two techniques. Am J Sports Med 1985;13:263-268.
Question 66
The preferred surgical approach to the elbow of a child with an irreducible type III supracondylar distal humerus fracture and pulseless extremity is through which of the following muscle intervals?
Explanation
REFERENCES: Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 115.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 119.
Question 67
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
REFERENCES: Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed):
Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 68
..Figures 78a and 78b are the radiographs of a 47-year-old right-hand-dominant woman who has a 3-month history of gradually progressive right shoulder pain. She reports no previous trauma, but does report pain at night and with activity such as weight training. Examination demonstrates active and passive range of motion to be 110 degrees forward elevation, external rotation to 20 degrees, and internal rotation to the sacrum. The next treatment step should include

Explanation
Rotator cuff and scapular stabilizer strengthening exercises
Diagnostic and therapeutic corticosteroid injection
Arthroscopic debridement
Completion of rotator cuff tear, repair, and biceps tenotomy
Acromioplasty
Repair of rotator cuff and superior labrum anterior to posterior (SLAP) repair
Repair of subscapularis tendon and biceps tenodesis
Question 69
Of all the pelvic ring injury types, anteroposterior compression type III pelvic ring injuries have the highest rate of which of the following?

Explanation
Question 70
Tension force in the anterior cruciate ligament during passive range of motion is highest at
Explanation
REFERENCES: Markolf KL, Burchfield DM, Shapiro MM, et al: Biomechanical consequences of replacement of the anterior cruciate ligament with a patellar ligament allograft. Part II: Forces in the graft compared with forces in the intact ligament. J Bone Joint Surg Am 1996;78:1728-1734.
Beynnon BD, Johnson RJ, Fleming BC, et al: The measurement of elongation of anterior cruciate-ligament grafts in vivo. J Bone Joint Surg Am 1994;76:520-531.
Question 71
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 72
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?
Explanation
REFERENCE: Gelehrter TD, Collins FS: Principles of Medical Genetics. Baltimore, Md, Williams & Wilkins, 1990, pp 27-45.
Question 73
A 20-year-old college soccer player comes for an evaluation 6 months after an injury during which he landed awkwardly from a jump. Although physical therapy, ice, and activity modification have helped him return to baseline motion, strength, and swelling, he continues to have lateral knee pain. He also notes a popping sensation on the lateral side of his knee with activity. A Lachman test, anterior and posterior drawer tests, a pivot shift test, and McMurray test findings are all negative. MR images reveal a 12-mm x 15-mm osteochondral defect in the lateral femoral condyle with full-thickness cartilage loss and approximately 4 mm of subchondral bone loss.
Explanation
Patellofemoral pain in a young athlete without patellar instability or a chondral or osteochondral defect often can be managed with nonsurgical treatment such as physical therapy and a home exercise program. Microfracture surgery is associated with good short-term results for younger athletes. Patients with no history of prior surgery, primary chondral rather than osteochondral lesions, and lesions smaller than 2 cm have experienced the best results. Microfracture surgery performed for chondral lesions of the central aspect of the medial femoral condyle is associated with worse results. Decreased activity levels over time of patients who undergo microfracture surgery are a concern. OAT provides good outcomes and return-to-sports rates for athletic people who are younger and have lesions smaller than 2 cm. Patients with lesions on the lateral femoral condyle have better success rates. Both microfracture surgery and OAT provide better results for chondral defects than osteochondral defects. OAT is associated with better results than microfracture for medium-sized lesions between 2 cm and 4 cm, while autologous chondrocyte implantation yields better improvement for patients with defects larger than 4 cm. All of the surgical techniques listed for articular cartilage repair are associated with better outcomes for patients younger than age 30.
Question 74
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?

Explanation
Question 75
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton’s neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657.
Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 76
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 77
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
Question 78
If the structure marked by the tip of the probe in Figure 94 is repaired to the bony glenoid with suture anchors during an arthroscopic stabilization procedure, what is the most likely result? Review Topic

Explanation
Question 79
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348.
Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 80
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?
Explanation
REFERENCES: Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Lemos MJ, Albert J, Simon T, et al: Radiographic analysis of femoral interference screw placement during ACL reconstruction: Endoscopic versus open technique. Arthroscopy 1993;9:154-158.
Question 81
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 82
A 65-year-old woman fell onto her outstretched right arm and immediately had pain. She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Beredjiklian PK, Nalbantoglu U, Potter HG, et al: Prosthetic radial head components and proximal radial morphology: A mismatch. J Shoulder Elbow Surg 1999;8:471-475.
Question 83
A 38-year-old woman has persistent elbow pain but is unable to recall a specific traumatic event. Examination reveals that the patient exhibits apprehension when the elbow is placed in valgus with forearm supination and axial loading. Because of chronicity and failure to respond to nonsurgical management, what is the most appropriate treatment? Review Topic
Explanation
Question 84
Figure 33 shows the oblique radiograph of an 11-year-old boy who has a mild left flatfoot deformity. Examination reveals that subtalar motion is limited and painful. Despite casting for 6 weeks, the patient reports foot pain that limits participation in sport activities. A CT scan shows no subtalar joint abnormalities. Management should now include
Explanation
has been described for treatment of the peroneal spastic flatfoot without demonstrable
tarsal coalition.
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Luhmann SJ, Rich MM, Schoenecker PL: Painful idiopathic rigid flatfoot in children and adolescents. Foot Ankle Int 2000;21:59-66.
Question 85
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
REFERENCES: Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 1831-1835.
Question 86
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
Explanation
REFERENCES: Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 87
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity. Postoperative radiographs are shown in Figures 3 and 4. How does the plate function?

Explanation
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 88
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern? Review Topic
Explanation
Question 89
Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic
Explanation
Question 90
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to Review Topic
Explanation
Question 91
A 6-year-old girl sustains an ankle injury after falling on roller blades. An AP radiograph is shown in Figure 68. Treatment should consist of which of the following?
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 92
A 30-year-old patient underwent open reduction internal fixation of a talar neck fracture 8 weeks ago. His current radiographs demonstrate a subchondral radiolucency of the dome of the talus. What is the next most appropriate course of action?

Explanation
Question 93
The patient is given a blood transfusion. After starting the transfusion, nurses note that her temperature is 38.8°C and she has shaking and chills. What is the most likely cause of this problem?
Explanation
Blood management and venous thromboembolism prevention are important considerations in the perioperative management of THA. Recommendations now focus on presurgical optimization of hemoglobin, use of antifibrinolytics intrasurgically, and minimized use of transfusions. Current recommendations do not favor autologous blood donation for patients with hemoglobin levels higher than 13 g/dL. There is a move toward increased use of aspirin for venous thromboembolism prophylaxis, but this modality can cause GI bleeding that may necessitate blood transfusion. Transfusion reactions are rare, and the most common cause is administration of an incompatible unit because of clerical error.
Question 94
Figure 43 shows an arthroscopic view of the posteromedial compartment of a patient’s left knee using a 70-degree arthroscope placed through the intercondylar notch. The arrow is pointing to what structure?
Explanation
REFERENCES: Miller MD: Basic arthroscopic principles, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, pp 224-237.
Gold DI, Schaner PJ, Sapega AA: The posteromedial portal in knee arthroscopy: An analysis of diagnostic and surgical utility. Arthoscopy 1995;11:139-145.
Question 95
Which of the following activities can improve posterior capsular contractures?
Explanation
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
Question 96
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?
Explanation
REFERENCES: Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1995;23:746-750.
Question 97
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?
Explanation
REFERENCES: Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Hasan SS, Leith JM, Campbell B, et al: Characteristics of unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg 2002;11:431-441.
Question 98
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279.
Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Wattenmaker I, Concepcion M, Hibberd P, Lipson S: Upper airway obstruction and perioperative management of the airway in patients managed with posterior operations on the cervical spine for rheumatoid arthritis. J Bone Joint Surg Am 1994;76:360-365.
Question 99
A 72-year-old man sustains a displaced four-part fracture of the proximal humerus with head split component following a fall. A primary shoulder arthroplasty has been recommended for acute management. In counseling the patient on pros and cons of hemiarthroplasty versus reverse arthroplasty, what statement can be made based on the available literature?
Explanation
arthroplasty in the setting of fracture is that forward elevation is independent of tuberosity healing and relies mainly on the deltoid muscle. Active external rotation following a reverse total shoulder for fracture, however, does appear to depend on successful union of the greater tuberosity. In a randomized controlled trial, the incidence of tuberosity healing was higher and the incidence of tuberosity resorption was lower in reverse arthroplasty compared with hemiarthroplasty. Forward elevation following a hemiarthroplasty for fracture generally follows a bimodal distribution, whereas outcomes following a reverse total shoulder have been more
consistent.
Question 100
Following ankle arthroscopy performed through a posterolateral portal, a patient notes numbness on the lateral half of the heel pad of the foot. What is the most likely injured structure?
Explanation
REFERENCES: Sitler DF, Amendola A, Bailey CS, et al: Posterior ankle arthroscopy:
An anatomic study. J Bone Joint Surg Am 2002;84:763-769.
Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 361.
