Orthopedic Board Review MCQs: Trauma, Arthroplasty & Hip | Part 70
Key Takeaway
This page offers Part 70 of a comprehensive OITE & AAOS Orthopedic Board Review. It features 100 verified, high-yield MCQs for orthopedic residents and surgeons preparing for certification exams. Covering Arthroplasty, Fracture, Hip, Osteoporosis, and Trauma, this interactive quiz aids focused, effective board exam preparation.
About This Board Review Set
This is Part 70 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 70
This module focuses heavily on: Arthroplasty, Fracture, Hip, Osteoporosis, Trauma.
Sample Questions from This Set
Sample Question 1: A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?...
Sample Question 2: A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotatio...
Sample Question 3: What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?...
Sample Question 4: 0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?...
Sample Question 5: Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Paprosky WG (ed): Revision Total Hip Arthroplasty. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 64-69.
Question 2
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
Fullerton LR Jr, Snowdy HA: Femoral neck stress fractures. Am J Sports Med
1988;16:365-377.
Question 3
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 4
0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?
Explanation
Cryotherapy has been demonstrated to achieve what effect after total knee replacement?
Decreased transfusion requirement
Improved pain, swelling, and analgesia
Improved range of motion at the time of discharge
Better long-term knee range of motion Corrent answer: 3
In a meta-analysis of randomized controlled trials on the efficacy of cryotherapy after total knee arthroplasty, patients treated with cryotherapy had less blood loss but no difference in transfusion requirements. There was better range of motion at the time of discharge from the hospital. There was no improvement in pain, swelling, or analgesia requirements. Patients treated with cryotherapy did not have better long-term range of motion.
Compared to retention of the native patella in primary total knee arthroplasty, routine patella resurfacing is associated with
no patellar complications.
an increased occurrence of anterior knee pain.
a decreased patellar fracture rate.
a decreased risk for revision surgery.
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
What clinical outcome is associated with total hip replacements that have metal-metal bearings (compared to total hip replacements with metal-polyethylene bearings)?
Soft-tissue sarcomas
Similar revision rates at 5 years
Increased nephrotoxicity
Pseudotumors
Patients with metal-metal total hip bearings have higher levels of cobalt and chromium in the bloodstream, but systemic migration of wear debris from total hip bearings is also common to total hip arthroplasties with polyethylene bearings. There is no direct evidence that patients with metal-metal total hip arthroplasties experience a higher incidence of cancer. Chromosome abnormalities have been detected in patients with metal-metal hip bearings, and the clinical consequences of this finding remain unknown. Also, pseudotumors can form around the periprosthetic joint space in response to localized metal ion debris and the host inflammatory response, although these tumors are not specific for failed metal-metal total hip arthroplasties. Metal-on-metal hip replacements have higher revision rates compared to conventional hip replacements in multiple registry studies. Although metal-on-metal articulations have not been shown to cause renal failure, they are not recommended in patients with chronic renal insufficiency.
A 55-year-old man with unilateral osteoarthritis of the hip underwent a total hip arthroplasty using cementless fixation. The acetabular cup was 52 mm and the femoral head was 28 mm and made of cobalt-chromium alloy. The bearing surface was made of annealed highly cross-linked polyethylene, with an estimated thickness of 6.5 mm. What should the orthopaedic surgeon tell the patient regarding wear of the bearing surface?
A highly cross-linked polyethylene bearing has superior wear characteristics compared to a conventional polyethylene bearing.
A highly cross-linked polyethylene bearing has similar wear characteristics compared to a conventional polyethylene bearing.
The incidence of osteolysis is expected to be higher with highly cross-linked polyethylene than with conventional polyethylene.
The volumetric wear rate would be lower if a 36-mm femoral head were used.
In a prospective, randomized clinical trial of 100 patients undergoing cementless total hip arthroplasties, the investigators compared highly crossed-linked polyethylene to conventional polyethylene. All of the femoral heads were 28 mm. The mean follow-up was 6.8 years. The mean head penetration was 0.003 mm/year for the highly cross-linked polyethylene group in comparison to 0.051 mm/year for the conventional polyethylene group (P =
.006). The improved wear is seen with larger-diameter heads as well. The volumetric wear rate of highly cross-linked polyethylene is equivalent to slightly higher with a larger head than a 28-mm head. Incidence of periarticular osteolysis is lower with highly cross-linked polyethylene.
A 49-year-old active man has groin pain 3 years after undergoing an uneventful total hip replacement using a cobalt-chrome femoral head articulating against a cobalt-chrome acetabular insert. The pain intensifies with activity and travels down his thigh. Examination and radiographic evaluation are not particularly helpful; there is no evidence of spinal or vascular disease. What is the next step in the evaluation of this patient?
A 3-phase bone scan
Measurement of synovial metal ions levels
Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and
possible hip aspiration
Bearing exchange to a metal-polyethylene combination Corrent answer: 3
ESR, CRP, and possible hip aspiration is the most logical next step even though at some point, bearing exchange may emerge as the ultimate treatment for a metal-metal adverse reaction in this patient. But the initial workup of a patient with a painful total hip that was otherwise functioning well must include the differential diagnosis of infection, which must be excluded with an appropriate laboratory workup, clinical history, and hip aspiration. The latter study may also help to diagnose a reaction to the metal bearing; cobalt and chromium levels in the aspirate can be investigated, and the color and quantity of the aspirate can be examined along with the cell count. Serum levels of metal ions at this stage could be both helpful and difficult to interpret.
Figures A and B are the radiographs of a 25-year-old woman whose right knee pain has progressed during the last several years to pain with any activity and pain at night. What is the most appropriate treatment?
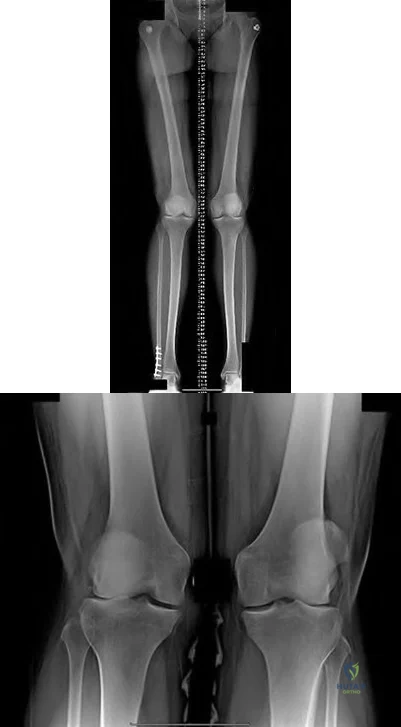
Proximal tibial osteotomy
Distal femoral osteotomy
Lateral unicompartmental arthroplasty
Total knee arthroplasty
Arthroscopic partial lateral meniscectomy Corrent answer: 2
This patient is a good candidate for a joint-preserving procedure. Her symptoms and radiographic findings reveal valgus malalignment of the knee with narrowing of the lateral joint space. The alignment can be corrected with a varus-producing distal osteotomy. Most patients do not proceed to knee arthroplasty for at least 10 years after this procedure. Osteotomy is preferred over partial or total knee arthroplasty because of the patient's young age.
Varus proximal tibial osteotomy would result in joint line obliquity.
An orthopaedic surgeon noticed a displaced calcar fracture during stem insertion when performing total hip arthroplasty using cementless fixation. What is the most appropriate course of action?
Intraoperative exploration to determine the extent of the fracture
Use of a longer stem without fixation of the calcar fracture
Complete insertion of the stem and measures to protect the patient against full weight bearing for 4 weeks
Removal of the stem, internal fixation of the fracture, and definitive reconstruction at a later stage after the fracture has healed
Calcar fractures can occur with both cemented and cementless stem fixation during surgery. The distal extent of the fracture must be identified either by direct visualization or intraoperative radiograph prior to fixation or implantation of the femoral component. The recommended treatment is to fix the calcar fracture with cerclage wires/cables to restore the mechanical stability of the femoral metaphysis. The same stem can be inserted successfully. The majority of these fractures unite without adverse stem fixation problems.
A 48-year-old woman had an 8-month history of spontaneous onset of left medial knee pain. She was otherwise healthy with an unremarkable past medical history. Prior to the onset of knee pain, she jogged, played tennis, and golfed regularly. She wished to remain active. Examination showed a fit woman with a BMI of 26, a stable left
knee with full range of motion, and some mild medial joint line tenderness. Radiograph results were normal. An MRI scan showed diffuse grade 3 and a focal area of grade 4 chondromalacia on the medial femoral condyle. The medial meniscus had a degenerative signal but no tear. The remainder of the knee showed no additional pathology. What is the most appropriate initial treatment?
Lateral heel wedge
Low-impact aerobic exercises
Glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day
Arthroscopic debridement and microfracture of the focal area of grade 4 chondromalacia to reduce risk for progression
This patient has early medial compartmental osteoarthritis of her knee. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), there is Level 1 evidence and an "A" recommendation for the use of low-impact aerobic exercises. The guideline also has "A" recommendations with Level 1 evidence indicating that glucosamine and chondroitin should not be prescribed and that arthroscopic debridement not be performed in the absence of symptoms of a meniscal tear or loose body. Lateral heal wedge is not appropriate; the AAOS guideline provides a "B" recommendation with Level 2 evidence indicating that a lateral heal wedge not be prescribed.
Figure 36 is the postoperative photograph of a patient who underwent a total knee arthroplasty 10 days after surgery. Knee aspiration suggests a Streptococcus infection.

Stop physical therapy and institute oral antibiotics.
Stop physical therapy and institute intravenous (IV) antibiotics.
Open irrigation and debridement, polyethylene spacer exchange, and IV antibiotics
Remove components and insert an antibiotic spacer.
An acute postoperative infection during the first 2 to 4 weeks should be treated with a return to the operating room for open irrigation and debridement of the wound. Polyethylene spacer exchange aides in washing out the entire knee joint. IV antibiotics are also indicated in this situation. To address persistent wound drainage, there is no role for oral or IV antibiotics alone. Removal of the arthroplasty components is recommended for infections after the initial 2- to 4-week postoperative period. However, several recent publications demonstrate a failure rate higher than 50% when the organism is a methicillin-resistant Staphylococcus aureus. Six weeks after surgery, this scenario is no longer considered an acute postoperative infection, and most authors recommend a 2-stage protocol with removal of components and placement of an antibiotic-impregnated cement spacer and 4 to 6 weeks of IV antibiotics.
What is the difference in outcome when comparing high tibial osteotomy (HTO) to total knee arthroplasty (TKA)?
TKA has a longer recovery period than HTO.
HTO provides more complete pain relief than TKA.
HTO is more reliable in older patients than TKA.
HTO outcomes among thin, active, young patients who undergo this procedure approach outcomes associated with TKA.
The ideal candidate for HTO is a thin, active person with a stable knee, unicompartmental knee symptoms, and age younger than 60. TKA offers a shorter recovery period and more complete pain relief than HTO. TKA is believed to be more reliable than HTO for patients older than age 60.
Figure 39 is a radiograph of a 72-year-old man who underwent an open reduction and internal fixation of a right femoral neck fracture. After 3 months he started to develop pain, and during the next 8 months he complained of progressive pain and shortening of the hip. What is the most appropriate treatment?

Girdlestone
Total hip replacement
Hardware removal
Hardware removal with revision open reductions and internal fixation Corrent answer: 2
Even though a relatively short amount of time has passed since the index surgery, this patient has developed significant osteonecrosis that has caused collapse of the bony structures and the hardware prominent. Total hip replacement gives the most efficient pain relief. Hardware removal with or without re-reduction does not provide reliable pain relief. A girdlestone does not allow the patient to function.
Figure 40 is the radiograph of a 68-year-old woman who has right knee pain that is limiting her activity and severe preoperative valgus deformity. During total knee arthroplasty, what pathologic features are typically encountered?

Lateral femoral hypoplasia
Internal rotation of the tibia relative to the femur
Medial patella tracking
Tight medial collateral ligament Corrent answer: 1
In patients with severe valgus deformity, problems frequently encountered include loose or attenuated medial collateral ligament, tight lateral retinaculum and lateral ligamentous structures (lateral collateral, posterolateral corner), atrophic lateral femoral condyle, lateral patella tracking, and external rotation of the tibia relative to the femur. The hypoplastic lateral condyle can cause internal rotation of the anteroposterior cutting block if the posterior condyler line is used for rotational alignment. The medial soft tissues are typically attenuated and stretched.
A 59-year-old active woman underwent elective total hip replacement using a posterior approach. She had minimal pain and was discharged to home 2 days after surgery. Four weeks later she dislocated her hip while shaving her legs. She underwent a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Observation and patient education regarding hip dislocation precautions
Revision to a larger-diameter femoral head
Revision to a constrained acetabular component
Application of a hip orthosis for 3 months Corrent answer: 1
First-time early dislocations are often successfully treated without revision surgery, especially when there is no component malalignment. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful, but is usually reserved for patients with recurrent dislocations.
Patellar pain, subluxation, or dislocation after total knee arthroplasty can result from which of the following component orientations?
Internal rotation of the tibial component
Lateralization of the tibial component
Lateralization of the femoral component
External rotation of the femoral component Corrent answer: 1
Internal rotation of the components of a total knee arthroplasty, both the tibial and femoral components, can lead to symptoms ranging from patellar pain to dislocation. Most researchers agree that proper external rotation of the femoral component is parallel or nearly so to the femoral epicondylar axis with the knee in the 90-degree flexed position. Proper rotational positioning of the tibial component places the midportion of the tibial component rotationally aligned within the medial one-third of the tibial tubercle. Internal rotation of the tibial component causes relative lateralization of the tibial tubercle and the extensor mechanism. Lateralization of the femoral component moves the trochlear groove laterally. Lateralization of the tibial component moves the tibial tubercle medially, which may be beneficial to patellar tracking.
How does the risk for periprosthetic infection after total knee arthroplasty compare to risk for infection after total hip arthroplasty?
Higher in primary arthroplasty
Lower in primary arthroplasty
Lower in revision arthroplasty
Equivalent in both primary and revision arthroplasty Corrent answer: 1
Risk for periprosthetic infection is higher in the knee (1%-2%) than it is in the hip (0.3%-1.3%). The risk for infection is higher after revision joint replacement surgery compared to primary joint replacement surgery.
Osteoarthritis is not associated with a higher risk for periprosthetic infection, but certain inflammatory conditions such as rheumatoid arthritis and psoriatic arthritis place patients at higher risk for postoperative infection.
What factor is associated with a higher risk for dislocation after total hip arthroplasty?
Male gender
Previous hip surgery
A direct lateral surgical approach
Metal-on-metal bearing surfaces Corrent answer: 2
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase risk for this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose lower risk for dislocation.
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
Posterior capsulorrhaphy
Use of a jumbo cup
Use of a lateralized liner
Use of a larger femoral head diameter Corrent answer: 2
When addressing recurrent dislocation after total hip arthroplasty, surgical considerations that must be addressed include approach, soft-tissue tension, component positioning, impingement, head size, and acetabular liner profile. These considerations most often involve tensioning or augmentation of soft tissues, as in capsulorrhaphy or trochanteric advancement; correction of malpositioned components; use of larger femoral head sizes that increase motion before impingement; improving the head-to-neck ratio; and increasing femoral offset. The use of a larger-diameter acetabular component may lead to soft-tissue overgrowth around the liner, causing impingement and increasing the risk for recurrent dislocation.
A 67-year-old active man returns for routine follow up 12 years after hip replacement. He has no hip pain. Radiographs revealed a
well-circumscribed osteolytic lesion around a single acetabular screw. All hip components were perfectly positioned. Six months later, comparison radiographs show an increase in the size of the osteolytic lesion. A CT scan shows a well-described lesion that is 3 cm at its largest diameter and is localized around 1 screw hole with an eccentric femoral head. What treatment is appropriate, assuming well-fixed cementless total hip components exist?
Revision of the polyethylene liner, removal of the screw, and debridement of the osteolytic lesion with or without bone grafting
Revision of the acetabular component to a newer design without screws
Removal of the screw, revision of the polyethylene liner, and stem cell injection into the lytic lesion
Removal of the offending screw from the metal socket and placement of a new polyethylene liner in the existing socket
With a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected with liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings during revision surgery. Here, complete cup revision is not warranted considering the appropriate implant position. Beaule and associates reviewed 83 consecutive patients (90 hips) in which a well-fixed acetabular component was retained in clinical scenarios such as the one described; no hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, or if the osteolytic lesion is not amenable to debridement through the screw hole, acetabular component revision may be indicated.
What has been identified as a risk factor for total knee arthroplasty failure after previous high tibial osteotomy?
Body mass index higher than 35
Female gender
Preoperative stiffness
Advanced age
Increased weight, male gender, young age at the time of total knee arthroplasty, laxity, and limb malalignment preoperatively have been identified
as risk factors for early failure for total knee arthroplasty following high tibial osteotomy.
You are caring for an 18-year-old boy with severe hip arthritis and pain from a missed slipped capital femoral epiphysis. You decide that a hip arthrodesis is the best treatment option. What is the optimum position for a hip arthrodesis to maximize function and prevent complications?
0° external rotation, 0° adduction, 0° hip flexion
5° external rotation, 5° adduction, 20° hip flexion
5° external rotation, 15° abduction, 5° hip flexion
15° external rotation, 0° adduction, 20° hip flexion
15° external rotation, 15° abduction, 5° hip flexion
Hip arthrodesis is a salvage procedure for patients with hip arthritis without ipsilateral knee, contralateral hip, or lumbar spine pathology. The optimal position for hip arthrodesis is 5 degrees of adduction, 5-10 degrees of external rotation, and 20-35 degrees of hip flexion.
In their review, Beaule et al. discuss the current indications and techniques regarding hip arthrodesis including appropriate leg position, surgical techniques, methods to optimize function, and later conversion to hip arthroplasty.
Callaghan et al. evaluated the long term efficacy (20-25 yrs) of hip arthrodesis. They found the onset of ipsilateral knee, contralateral hip, or lumbar spine pathology usually began 20 years after the arthrodesis. Of their patients, they found a 15% rate of conversion to hip arthroplasty by 20 years.
What limits indications for the use of constrained liners?
Association with periprosthetic fracture
Technical difficulty associated with insertion
High costs associated with their use
High failure rates associated with their use Corrent answer: 4
Because of reports of relatively high failure rates associated with constrained liners, indications are limited to continued instability after appropriate component position or deficient abductor mechanism and instability. Neither cost nor technical insertion issues are relevant with regard to indications for use. Periprosthetic fractures are not associated with constrained liner usage.
What serum inflammatory marker has the highest correlation with periprosthetic joint infection?
C-reactive protein
Serum white blood cell count
Erythrocyte sedimentation rate
Interleukin 6 (IL-6)
Although CRP and ESR can be elevated in the setting of infection, IL-6 has been shown to have the highest correlation with infection. Serum white blood cell count has been shown to be ineffective in correlating with periprosthetic joint infection.
A 68-year-old man reports hip pain 15 years after successful cementless total hip arthroplasty. Radiographs show 3 mm of linear wear of the modular acetabular liner and a retro-acetabular osteolytic lesion. Both the titanium femoral and acetabular components appear to be well fixed. The orthopaedic surgeon recommends revision of the acetabular liner and femoral head. This patient is at increased risk for
dislocation.
periprosthetic fracture.
infection.
progressive osteolysis.
Isolated acetabular liner revision is frequently performed in cases of liner wear and periprosthetic osteolysis in the absence of acetabular component loosening. Many reports have documented an increased incidence of dislocation following this type of revision surgery. This dislocation rate can be reduced by using a larger-diameter femoral head at the time of revision. If the
acetabular component is loose or malpositioned, it should be revised. If the locking mechanism is damaged, then a replacement liner may be cemented into the well-fixed shell. Numerous studies have shown that many osteolytic lesions will reduce in size or heal without bone grafting, and removal of the source of wear debris will arrest the progression of osteolysis. The risk for periprosthetic fracture and infection are lower than risk for dislocation in this setting.
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day.
weight loss through dietary management and low-impact aerobic exercises.
arthroscopic debridement and lavage.
a valgus-directing brace.
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), Level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day and arthroscopic debridement and lavage).
The range of knee mobility after total knee replacement is multifactorial and dependent upon implant design, surgical implantation accuracy, and patient-specific variables. What total knee implant design is associated with the most knee flexion after total knee replacement?
Highly conforming articular surface geometry
Higher-flexion femoral component design manufactured to allow the most knee flexion
Posterior cruciate-stabilized implant, with or without a higher flexion
manufacturing modification
Posterior cruciate-retaining design with a mobile bearing, custom implanted based on CT scan data
A posterior cruciate-stabilized implant has the best support in the literature in terms of the most favorable range of motion after knee arthroplasty, regardless of whether the femoral component is designed with a higher flexion variation. The higher flexion design is a manufacturing variation that is intended to increase motion by clearing the posterior condyles in flexion.
Although the knee may not gain more flexion, this design allows for more safety in deep flexion. The long-term outcomes of increased stresses on the polyethylene are not known, however. By itself, a higher-flexion design does not lead to increased knee mobility. The effects of mobile bearings, custom CT scan-based knee implantation, and highly conforming designs on ultimate knee range of motion are uncertain.
In total knee arthroplasty, in vitro testing has shown that crosslinking can diminish the rate of polyethylene wear by 30% to 80%.
What other change in material properties is possible when polyethylene is highly cross-linked?
Increased ductility
Increased wettability
Diminished fatigue strength
Decreased resistance to abrasive wear Corrent answer: 3
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been identified as causing implant failure in most recent clinical trials, but remain the most important mechanical issues associated with current material processing methods.
What factor is associated with a high risk for developing pseudotumors after metal-on-metal hip resurfacing?
Large-diameter components
Age 40 or older for men
Age 40 or younger for women
Diagnosis of primary osteoarthritis Corrent answer: 3
The recent experience of a large clinical cohort revealed the most likely risk factors as female gender, age younger than 40, small components, and the diagnosis of hip dysplasia causing osteoarthritis. Failure was least likely among men and procedures involving larger components. These data have prompted some authors to caution against use in women and to primarily target candidates who are men younger than age 50. Small components may be more prone to failure because of malpositioning and edge loading, which have been noted to be more common in dysplasia cases.
A 70-year-old man is scheduled to undergo bearing surface revision for wear and osteolysis 10 years after cementless total hip arthroplasty. The femoral head is 28 mm alumina-oxide ceramic material. The components are in good position, and there is no evidence of fixation loosening of either component by radiograph or preoperative bone scan. What outcome is associated with isolated polyethylene exchange?
Reduced risk for future wear and osteolysis with a larger femoral head
Reduced risk for future wear and osteolysis with a cobalt chrome femoral head
Similar risk for dislocation compared to primary total hip arthroplasty
Increased risk for dislocation compared to primary total hip arthroplasty Corrent answer: 4
The major complication associated with polyethylene exchange is postoperative dislocation. Maloney and associates noted a dislocation rate of 11% in a study of 35 hips after such revision. Boucher and associates reported a 25% rate of dislocation in a study of 25 patients. Larger femoral heads result in higher volumetric wear in contrast to smaller-diameter heads. Stem revision is not indicated because there is no fixation loosening. Moreover, stem biomaterial has no effect on polyethylene wear.
A healthy, active 68-year-old woman had a total hip arthroplasty 3 months ago. She has been to the emergency department with a posterior dislocation 3 times during the last 2 months. Plain radiographs and a CT scan confirm that the acetabular component is oriented in 5 degrees of retroversion and 55 degrees of abduction.
What is the most appropriate treatment?
Revision of the femoral and acetabular components
Maximizing head-neck ratio and increasing head length
Acetabular component revision
Closed reduction with an abduction brace and reinforcement of hip precautions
Acetabular malposition can lead to recurrent instability. When this cause is confirmed, reorientation of the component can lead to successful revision surgery. Revision of the femoral component may not be necessary if the acetabular component is repositioned. Increasing length and maximizing head-neck ratio cannot make up for component malposition. There is no role for nonsurgical treatment in the setting of recurrent instability with component malposition in an active, healthy patient.
A 55-year-old woman with history of HIV infection is scheduled for revision total knee arthroplasty to address instability. The index surgery was done 3 years ago. What is the white blood cell (WBC) count threshold in the synovial fluid for an infection diagnosis?
Question 5
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?
Explanation
REFERENCE: Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 6
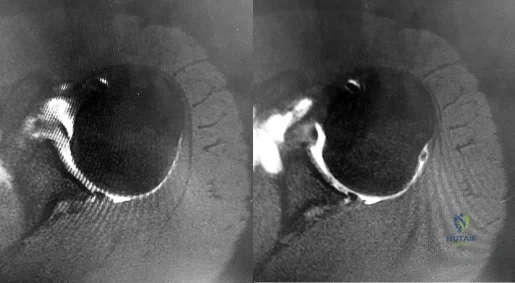
Figures 150a through 150d are the radiographs and MR images of a 37-year-old woman who has a 3-month history of severe right hip pain. She does not recall any trauma prior to the pain onset and denies any past steroid exposure. She has 3 children and is not currently pregnant. The pain is located in her groin and the onset was sudden. The pain is refractory to anti-inflammatory medications. What is the most appropriate treatment?
Explanation
The patient’s MR images are consistent with transient hip osteoporosis. No signs suggest avascular necrosis. She has no joint narrowing. Transient osteoporosis of the hip is characterized by bone marrow edema in the femoral head and neck. This condition affects more men than women and is sometimes seen in the third trimester of pregnancy but can be seen in women who are not pregnant as well. This is a self-limiting condition, and the treatment is limited weight-bearing activity until the symptoms resolve. Core decompression is rarely used in these cases. There is no indication for arthroplasty or osteotomy in this scenario.
Question 7
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?

Explanation
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 8
The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has
Explanation
REFERENCES: Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
Shackford S: Spine injury in the polytrauma patient: General surgical and orthopaedic considerations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 9-15.
Question 9
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon: Results of operative treatment. J Bone Joint Surg Am 1996;78:1015-1023.
Question 10
What is the most commonly reported complication following elbow arthroscopy?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 11
A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values show a WBC count of 11,400/mm3 and an erythrocyte sedimentation rate of 52mm/h. What is the most appropriate action? Review Topic
Explanation
susceptibility to antibiotics, and implant stability. An MRI scan to evaluate for a rotator cuff tear is not indicated at this time.
Question 12
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle? Review Topic

Explanation
such as Parsonage-Turner syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
Question 13
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
Explanation
and degenerative joint disease.
Question 14
Genetic mutations that may result in the cervical abnormalities noted in the figures generally affect the
Explanation
The figures are characteristic of a child with Klippel-Feil syndrome (congenital cervical spine abnormalities) in association with congenital scoliosis in the upper thoracic spine and a right-sided Sprengel deformity (congenital elevation of the scapula). Sprengel deformity occurs in as many as 30% of children with Klippel-Feil syndrome. Other congenital conditions that are commonly associated with Klippel-Feil, and that should be screened for, include deafness in 30%, genitourinary abnormalities in 25% to 35%, and cardiovascular abnormalities in 4% to 29% of children with Klippel-Feil syndrome.
In Sprengel deformity, there is usually a tether called the omovertebral connection between the abnormally elevated scapula and the spinous processes in the upper thoracic region. This tether is most commonly bony but also may be cartilaginous or fibrous. Although there also may be abnormalities in the ribs, clavicle, or humerus, they are morphologic abnormalities only, not tethers.
Patients with Klippel-Feil syndrome should be discouraged from participating in contact or collision sports if they have a massive fusion of the cervical spine, any involvement of C2, or limited cervical motion. Fusions at 1 or 2 interspaces below C3 and normal cervical motion do not preclude participation in activities. A Sprengel deformity may limit abduction of the shoulder and normal racquet or throwing mechanics, but, in the absence of pain, is not a contraindication to attempted participation.
Klippel-Feil syndrome affects a heterogenous cohort of patients and different inheritance patterns have been seen, including autosomal-dominant and autosomal-recessive types, with varying levels of penetrance. The first human Klippel-Feil syndrome locus was identified on chromosome 8 and is called SGM1. Other candidates for mutations in Klippel-Feil include PAX genes and Notch pathway genes. In general, the involved genes help regulate the formation and segmentation of the vertebrae.
Between days 20 and 30 following conception, the paraxial mesoderm subdivides into segments called somites. As they mature, somites develop into 3 layers called the sclerotome, myotome, and dermatome. The sclerotome undergoes a process of resegmentation during which the caudal section from 1 somite joins with the rostral section of the immediately caudal somite to form the vertebral bodies. It is during the processes of segmentation and resegmentation that the abnormalities leading to Klippel-Feil syndrome occur. Gastrulation refers to the phase early in embryonic development when the single-layered blastula is reorganized into a trilaminar structure with 3 germ layers: the ectoderm, mesoderm, and endoderm. Neurulation refers to the process by which the notochord induces formation of the neural tube from the neural plate, forming the brain and spinal cord.

Question 15
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
REFERENCES: Veltri DM, Warren RF: Isolated and combined posterior cruciate injuries. J Am Acad Orthop Surg 1993;1:67-75.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont IL, American Academy of Orthopaedic Surgeons, 2002, pp 489-511.
Question 16
A patient in the recovery room has weakness of the extensor hallucis longus and tibialis anterior muscles following a total knee replacement. Initial management should consist of
Explanation
This is a rare
complication of TKA, and when conservative nonoperative measures do not lead to sufficient improvement in nerve function, consideration may be given to operative decompression of the peroneal nerve.
Question 17
What is the plasma half-life of warfarin?
Explanation
Question 18
During spinal deformity surgery, which of the following is the most specific early indicator of an intraoperative injury to the spinal cord? Review Topic
Explanation
Question 19
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 197.
Question 20
Figure 94 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. After injury to the structure as indicated by the asterisks, which examination test most likely will demonstrate an abnormal finding?
Explanation
The structure shown is the PL bundle of the anterior cruciate ligament (ACL), which is tight near terminal knee extension. Biomechanical analysis suggests the PL bundle provides a greater degree of rotational stability than the anteromedial bundle. The pivot-shift test evaluates for rotational instability of the ACL, while the Lachman test assesses anterior-posterior stability. The posterior drawer and PL drawer test findings are positive after a posterior cruciate ligament tear and PL corner injury, respectively.
RESPONSES FOR QUESTIONS 95 THROUGH 98
Axillary nerve injury
Musculocutaneous nerve injury
Radial nerve injury
Glenoid fracture
Loss of reduction
Deltoid detachment
Chondrolysis
Recurrent instability
Propionibacterium acnes (P. acnes) infection
Staphylococcus epidermidis
Staphylococcus aureus
Select the complication listed above that is most commonly associated with the shoulder arthroscopy scenarios described below.
Question 21
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?

Explanation
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Question 22
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
REFERENCES: Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181.
Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Kuroda R, Kambic H, Valdevit A, et al: Articular cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med 2001;29:403-409.
Question 23
Optimal management of the injury shown in Figure 31 should include which of the following?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 24
Figure 1 is the clinical photograph of a 65-year-old right-hand dominant man who has finger contracture and stiffness. He experiences minimal pain but has severe functional limitations and elects for treatment with injectable collagenase Clostridium histolyticum . What types of collagen will be affected by this injection?

Explanation
Type II collagen is the predominant type found in articular cartilage. Type IV collagen is the predominant type found in the basement membranes of neurovascular structures. Collagenase Clostridium histolyticum injection targets type I and type III collagen.
Question 25
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?

Explanation
DISCUSSION: A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
Question 26
An orthotic that provides laterally based hindfoot posting support would be most useful for which of the following conditions? Review Topic
Explanation
Cavovarus feet may be seen in multiple conditions, including Charcot-Marie-Tooth disease. The initial deformity is plantarflexion of the first ray, which is often followed by compensatory hindfoot varus. In flexible deformities, orthotics that post the lateral forefoot and lateral heel should be utilized.
Schwend et al. review the etiology, diagnosis and management of the cavus foot in children. They note that shoe inserts with lateral support can be used in patients when there is flexibility to the hindfoot. Recession of the orthotic to accommodate a plantarflexed first ray is also beneficial.
Illustration A shows an orthotic with lateral foot posting and a recessed area for the first metatarsal head. Illustration B shows an AP radiograph of the left foot demonstrative of an accessory navicular. This may be associated with a flatfoot deformity. Illustration C shows a lateral radiograph of a right foot with a middle facet coalition. This may give rise to a rigid, painful flatfoot deformity. Illustration D shows a lateral radiograph of a right foot with collapse of the medial longitudinal arch. This patient had a flexible flatfoot that was painful. Illustration E shows an AP radiograph of a left foot with evidence of metatarsus adductus. Note the alignment of the 2nd metatarsal axis relative to the proximal articular surface of the middle cuneiform. In this case, the metatarsus adductus angle (MAA) was 24 degrees (normal is < 20 degrees).
Incorrect Answers:
Question 27
He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?

Explanation
Question 28
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 29
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 30
5 g/dL and his base deficit is 10mEq/L. What is the most appropriate next step in management?
Explanation
Of all of the reported values, the most important predictor of morbidity and mortality is the base deficit (normal range -2 to +2mEq/L), which represents overall resuscitation status. Another representative parameter of resuscitation status is lactate (normal <2mg/dL). Heart rate, blood pressure and hematocrit are not reliable predictors of normalized resuscitation status, morbidity or mortality.
Callaway et al. retrospectively reviewed a large cohort of blunt trauma patients over a 6 year period. Only base deficit and lactate levels were directly correlated with and were reliable predictors of mortality.
Paladino et al. retrospectively reviewed a prospective database of over 1400 patients. Base deficit and lactate were significant and useful predictors of triage upon initial presentation to denote severe versus non-severe injury.
Martin et al. retrospectively analyzed over 2000 sets of laboratory data in 427 ICU patients. Base deficit (anion status), even in ICU patients with normal lactate levels, were predictive of decreased survival.
Incorrect Answers:
OrthoCash 2020
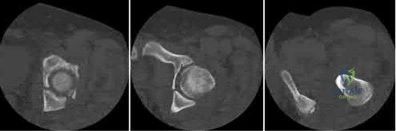
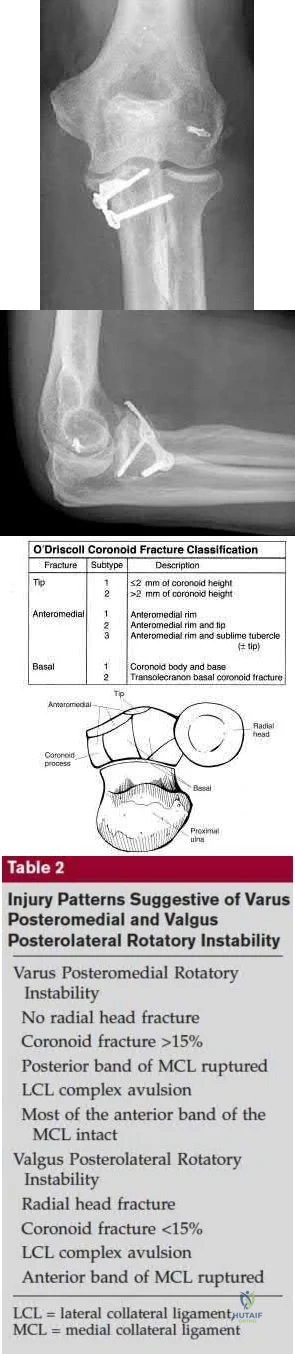
A 26-year-old male sustains an elbow injury after a fall from a skateboard resulting in valgus and supination forces across the left elbow. A CT scan of the left elbow is shown in Figures A through D. This fracture pattern is most commonly associated with what other traumatic elbow pathology?
Posteromedial rotatory instability
Capitellum fracture
Radial head fracture and posterolateral ulnohumeral dislocation
Trans-olecranon fracture dislocation
Medial (ulnar) collateral ligament rupture Corrent answer: 3
The clinical presentation is consistent with a coronoid tip fracture. This fracture pattern is associated with a radial head fracture and posterolateral ulnohumeral dislocation - together making up the terrible triad injury.
A terrible triad injury is the result of a valgus and supination injury and involves posterolateral elbow dislocation or lateral collateral ligament injury, radial head fracture, and fracture of the coronoid process. The elbow may dislocate postero-laterally with the anterior bundle of the MCL intact, but if the MCL is injured it is typically the last structure to fail. The coronoid fracture is typically a small fragment isolated to the tip. This is a result of a posteriorly directed force driving the coronoid into the trochlea prior to posterior elbow dislocation. CT scan is a useful modality when small or comminuted fragments are difficult to visualize on plain radiographs.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figures A through D show consecutive 2.00 mm sagittal CT reformats demonstrating a small coronoid fracture fragment which was addressed with suture fixation.
Incorrect Answers:
OrthoCash 2020
A 62-year-old right-hand-dominant school teacher sustains a mechanical fall at home and presents with right shoulder pain. Plain
radiographs of the right shoulder are pictured in Figures A and B. The patient asks you what she can expect in terms of recovery following this injury. Which of the following is the most appropriate statement?
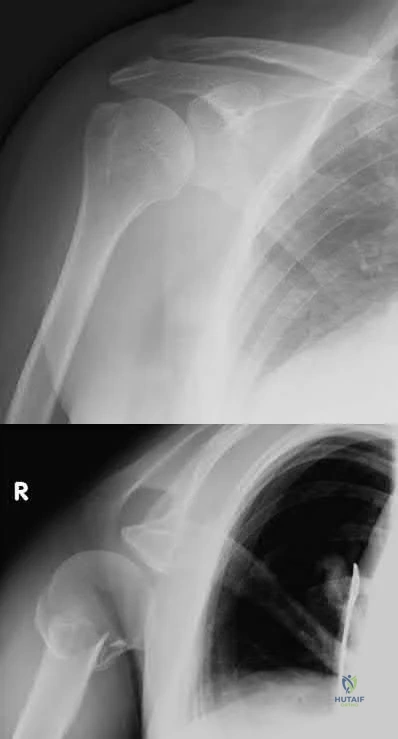
At 1-year post-injury, the right shoulder range of motion will most likely be equal to the contralateral extremity.
At 1-year post-injury, you will most likely have returned to your baseline functional status.
Early range of motion exercises risk fracture displacement and should be avoided until at least 4 weeks post-injury.
Most patients do not return to work following this injury.
One in 5 patients with this fracture go on to nonunion and you may benefit from surgery in the future to address this.
This patient has a minimally displaced (1-part) proximal humerus fracture involving the humeral neck and greater tuberosity. This injury pattern is most commonly managed nonoperatively with the majority of patients returning to their baseline functional status by 1 year.
Proximal humerus fractures (PHF) can be classified by number of parts (Neer classification), with a part defined as a fracture fragment displaced > 1cm (> 5mm for greater tuberosity) or angulated > 45°. One-part PHF comprise ~80% of all PHF and are treated nonoperatively with a sling and early range of motion (ROM).
Tejwani et al performed a prospective study of 67 patients with 1-part PHF. At 1-year follow up the ASES score and functional status was similar to pre-injury status. However, ROM of the affected shoulder was diminished in both external and internal rotation. Forward flexion was preserved.
Hanson et al prospectively analyzed 160 patients with PHF of all types (1-4 parts and head-splitting) managed nonoperatively. At 1-year follow up, 93% showed solid union. Constant and DASH scores improved steadily over time but were still lower compared to the contralateral extremity. Of employed patients, 97.6% returned to work with a median time off of 10 weeks and no difference between manual and nonmanual workers.
Figures A and B are the AP and axillary radiographs of the right shoulder, respectively, demonstrating a 1-part PHF involving the humeral neck and greater tuberosity.
Incorrect Responses:
OrthoCash 2020
A 44-year-old male presents with the isolated injury seen in Figure A after a motor vehicle accident and underwent the operative treatment seen in Figure B within 8 hours from the time of incident. Which of the following complications is this patient at highest risk of developing?

Pulmonary embolus
Periprosthetic fracture
Contralateral hip fracture
Osteonecrosis
Infection
This young male patient has sustained a displaced femoral neck fracture and underwent open reduction internal fixation with 3 cannulated screws. Based on the available options, the patient is most at risk of developing osteonecrosis of the femoral head.
Femoral neck fractures in young patients typically are the result of a high-energy trauma. Fracture displacement has been shown to disrupt vascular supply to the femoral head by interrupting retinacular vessels and ligament teres vascularization, as well as increasing intracapsular pressure, producing a tamponade effect. The incidence of osteonecrosis in patients younger than 60 years with displaced femoral neck fractures has been shown to be between 15-30%. Quality of reduction is one key factor that has been shown to influence outcomes postoperatively.
Loizou et al. prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using standard fixation modalities. They showed that osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%). The population at greatest risk were women younger than the age of 60 with displaced fractures.
Barnes et al. review subcapital hip fractures. They found that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years treated with internal fixation.
Figure A shows a displaced, Garden 3/Pauwels III hip fracture. Figure B shows anatomical fixation with 3 cannulated screws.
Incorrect Answers:
OrthoCash 2020
A 58-year-old male is involved in a motor vehicle collision and sustains the injury shown in Figure A in addition to right 5th and 6th rib fractures. Upon evaluation in the emergency department, he is noted to have a 2 centimeter laceration over the anterior aspect of his left leg with visible bone. Vitals and labs are normal. Which of the following statements is most accurate regarding surgical management for this patient?

Reamed intramedullary nailing is favored due to increased rates of union
Unreamed intramedullary nailing is favored due to presence of concomitant rib fractures
Reamed intramedullary nailing is favored due to decreased rates of infection
Unreamed intramedullary nailing is favored due to less local trauma
Both unreamed and reamed intramedullary nailing are equivalent Corrent answer: 5
Both unreamed and reamed intramedullary nailing are equivalent treatments in patients with open tibia fractures. Intramedullary nailing is the treatment of choice for stable patients with tibial shaft fractures.
Tibial shaft fractures can be the result of low energy twisting injuries or higher energy axial loads. Closed fractures with acceptable alignment can be often be treated with closed reduction and casting. Intramedullary nailing, unreamed or reamed, is the treatment of choice for open fractures except in the setting of damage control orthopaedics when an external fixator may be more appropriate.
Bhandari et al. investigated reamed and unreamed intramedullary nailing for tibial shaft fractures in a randomized trial ("SPRINT" Trial - Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators). They concluded that reamed nailing was more beneficial (decreased rate of primary outcome event: need for bone grafting, implant exchange or removal for infection, debridement for infection) for closed fractures, but had no benefit in open fractures.
Finkemeier et al. evaluated consecutive patients treated with unreamed and reamed intramedullary nailing and found similar rates of union in both open and closed tibial shaft fractures at six and twelve months.
Figures A shows AP and lateral xrays of the left tibia showing a tibial shaft fracture.
Incorrect Answers:
OrthoCash 2020
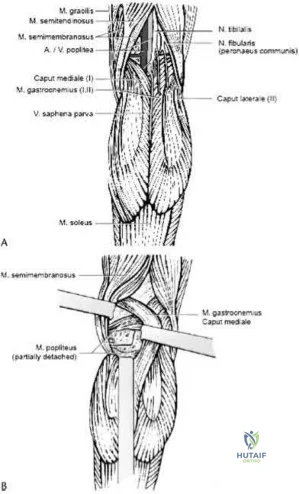
A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
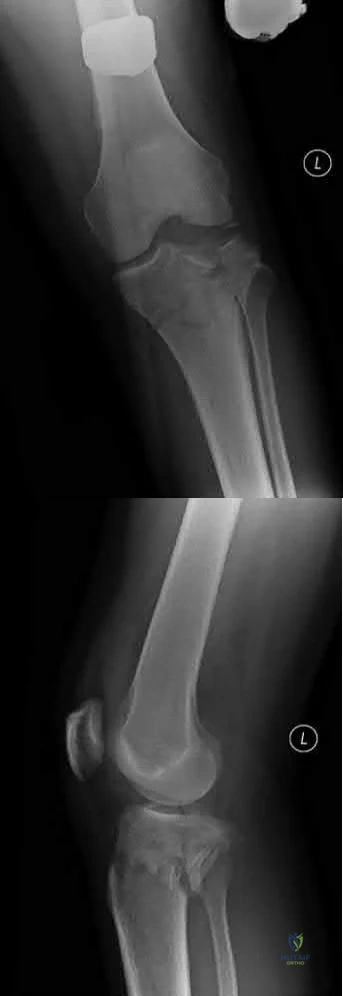
Popliteus and pes anserine
Lateral head of the gastrocnemius and pes anserine
Politeus and lateral head of the gastrocnemius
Iliotibial band and medial head of the gastrocnemius
Pes anserine and medial head of the gastrocnemius Corrent answer: 5
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
OrthoCash 2020
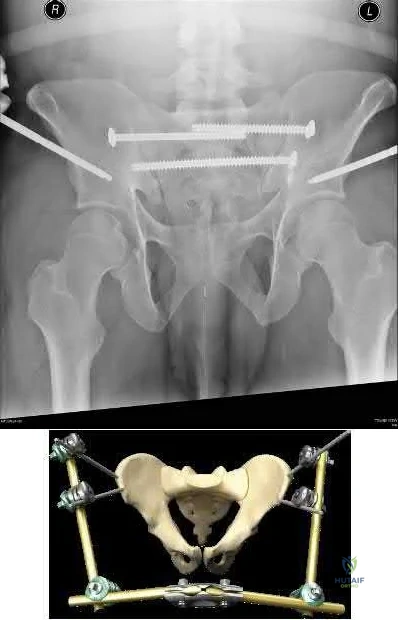
A 25-year-old male presents to the emergency department with the injury seen in Figure A after a motorcycle collision. The patient has a blood pressure of 70 systolic, elevated lactate and a tense abdomen with positive FAST examination. Trauma surgery will be performing an emergent laparotomy. Orthopaedic surgery is consulted and places a pelvic external fixator intraoperatvely to assist with resuscitation. What is an advantage of supra-acetabular external fixator pins as compared with iliac crest pins?

Less interference with pelvic surgical incisions
Less risk of pin tract infection
Less risk of malreduction
Less control of posterior pelvic ring
No interference with laparotomy Corrent answer: 1
One advantage of supra-acetabular external fixator pins is that they do not interfere or contaminate future approaches to the pelvis or acetabulum involving the lateral window.
In multiply injured patients with pelvic trauma external fixation of the pelvic ring is a valuable tool to assist with resuscitation. Pelvic external fixation should be applied rapidly and allow full access to the abdomen for general surgery intervention. Regardless of the technique used, a pelvic external fixator should form a stable construct that minimizes motion of fracture surfaces and allows for clot formation.
Haidukewych et al evaluated the safety of supra-acetabular pin placement in a cadaveric study. The authors found that the lateral femoral cutaneous nerve (LFCN) was most at risk during pin placement.
Figure A demonstrates a widely displaced symphyseal dislocation with associated bilateral sacroiliac (SI) dislocations (APC 3). Illustration A demonstrates an outlet radiograph of a supra-acetabular external fixtator in conjunction with posterior pelvic ring fixation for an LC3 pelvic ring injury.
Illustration B is an illustration of iliac crest external fixation. The video demonstrates techniques for application of both supra-acetabular and iliac
crest external fixation pins.
Incorrect Answers:
OrthoCash 2020
What physical exam finding is most likely to be found in association with the injury shown in Figures A and B?

Numbness in the small finger and ulnar side of the ring finger
No elbow instability
Varus posteromedial rotatory instability
Valgus posterolateral rotatory instability
An anterior open wound Corrent answer: 3
The x-ray shows a fracture of the anteromedial facet of the coronoid with an intact radial head. Large anteromedial facet fractures are associated with varus posteromedial rotatory instability.
The anteromedial facet of the coronoid provides support to the medial elbow against varus stress. Varus and posteromedial force applied to the elbow results in disruption of the lateral collateral ligament (LCL) from its proximal origin. The coronoid is fractured as it is forced against the medial trochlea.
Coronoid fractures of significant size involving the sublime tubercle (insertion of medial collateral ligament) result in varus instability.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques. He states that when a coronoid fracture is associated with a pattern of varus instability, it requires fixation with either suture, buttress plating or screw fixation. Concomitant LCL repair or reconstruction will also be necessary.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong
associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figure A is an AP view of an elbow with an anteromedial facet of the coronoid fractured. The lateral joint space is widened due to injury to the LCL. The medial joint space is narrowed and collapsed. A lateral view is shown in Figure
B. Illustrations A and B show AP and lateral views of a coronoid fracture fixed with buttress plating. The LCL origin was fixed with a suture anchor. Illustration C shows the O'Driscoll classification of coronoid fractures. Illustration D lists injury patterns that suggest posteromedial versus posterolateral rotatory instability.
Incorrect Answers:
OrthoCash 2020
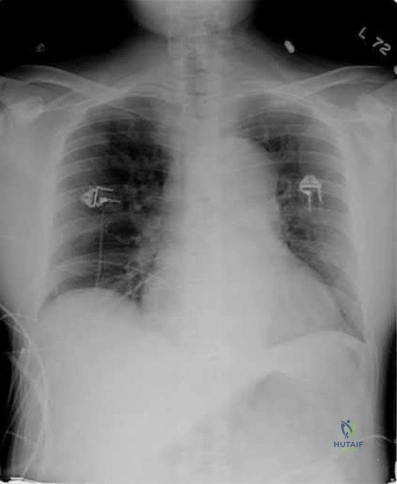
A 35-year-old man presents to the ED as the restrained driver of a high speed motor vehicle collision complaining of hip, chest, and abdominal pain. He becomes diaphoretic, tachycardic, and hypotensive in the trauma bay and is noted to have diminished lower extremity pulses. He is found on ATLS workup to have mediastinal widening.
Which of the following injuries is most associated with thoracic aortic injury?

Thoracic aortic rupture is associated with posterior hip dislocation in deceleration trauma mechanism of injuries.
Posterior hip dislocations are infrequently associated with local vascular injuries. With bilateral perfusion deficits, more proximal large vessel trauma should be considered, and in this situation, thoracic surgery should be involved emergently. Screening chest x-ray in the trauma bay should be reviewed for widened mediastinum, suggestive of aortic injury, as shown in illustration A. Given the high energy mechanism associated with these injuries, a full ATLS trauma survey must be done for every patient.
Marymont et al. studies the association between posterior hip dislocation and thoracic aortic injury. They performed a retrospective chart review of 89 posterior hip dislocations and found 8% had an aortic injury. Although not statistically significant, they note the importance of evaluation for aortic injury in patients with posterior hip dislocations given its emergent life-threatening nature.
In addition to associated chest injuries, Schmidt et al. highlight the importance of evaluating the ipsilateral knee after high-energy traumatic hip dislocation. In a prospective study, they identified a 93% rate of ipsilateral knee injury on MRI including effusion (37%), bone bruising (33%), and meniscal tear (30%) as the most common. They recommend a thorough exam but also expanded use of knee MRI after hip dislocation.
Illustration A shows an example of chest x-ray with a widened mediastinum, suggestive of thoracic aortic injury.
OrthoCash 2020
A 31-year-old female smoker was involved in a skiing accident approximately 9 months ago and underwent open reduction internal fixation of the radius and ulna at the time of injury. She now returns to the clinic complaining of increasing pain with range of motion and activity. Radiographs from her most recent follow-up can be seen in Figure A. Laboratory tests show ESR, CRP and WBC count to be within normal limits. Which of the following options is the most appropriate next step in management?

Bone scan
Above elbow cast
Removable splint
Reamed intramedullary nail
Iliac crest bone grafting + compression plating Corrent answer: 5
This patient is presenting with an atrophic non-union of the ulna after open reduction internal fixation for a both bone forearm fracture 9 months ago. The most appropriate next step in management would be iliac crest bone grafting and compression plating of the ulna.
The primary issue with an atrophic nonunion is biological. The blood supply is poor and therefore incapable of purposeful fracture healing. Smokers, as in this vignette, are at high risk for nonunion. The treatment of an atrophic nonunion involves improving biology at the fracture site through use of autologous bone graft (e.g. iliac crest) and providing mechanical stability by means of compression plating (e.g. 3.5 mm LC-DCP).
dos Reis et al. reports excellent results of 31 cases of diaphyseal forearm fracture non-unions treated with autologous bone grafting and compression
plating. Thirty of thirty-one patients went on to bony union within 3.5 months of revision surgery.
Nadkarni et al. presented a case series of 11 patients with non-unions of various long bones initially managed with intradmedullary (IM) nail fixation. The authors successfully used locking compression plates while retaining the IM nails in the treatment of the nonunion in all cases.
Figure A shows an AP radiograph of a both bone forearm fracture. Figure B shows an AP and lateral radiograph of an atrophic non-union of the ulnar shaft. Illustration A shows a lateral x-ray of a fully healed radius and ulna after hardware removal 1 year after revision surgery.
Incorrect Answers:

OrthoCash 2020
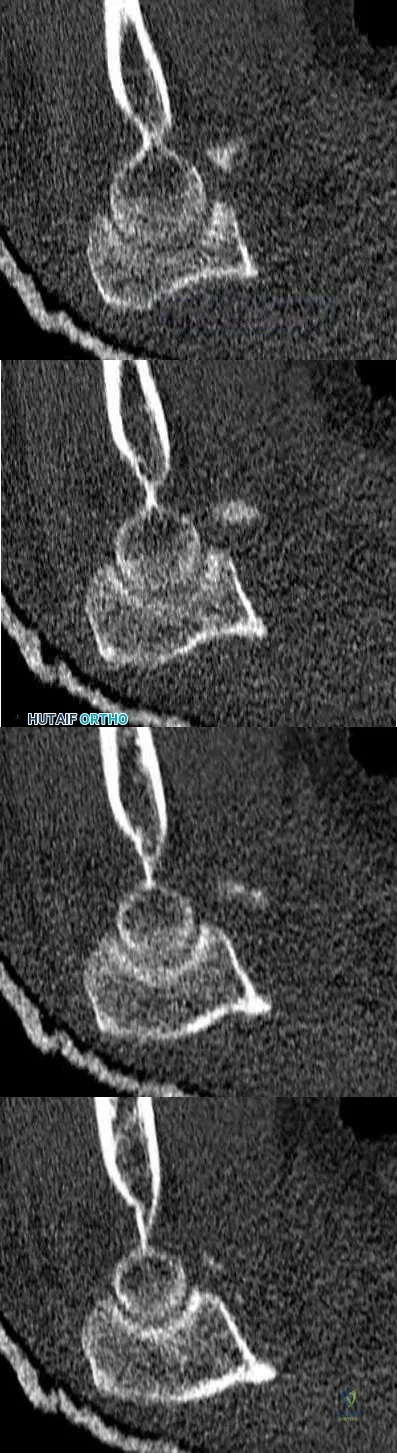
A 27 year-old patient sustains a fracture-dislocation of the acetabulum. Pelvic radiographs (Figures A and B) are taken at initial presentation and a CT scan (Figures C and D) is performed after reduction of the hip in the emergency room. What is the importance of the finding highlighted in the CT scan cuts?

Comminution indicates a better result with non-operative management
Significant marginal impaction could compromise the results of the surgical reduction if the joint surface is not properly restored
The impacted fracture segment will heal without fixation because it is not gapped or translated
The CT scan finding highlighted indicates osteochondral defects to the femoral head, which can be addressed arthroscopically
Intraarticular fracture fragments should be discarded from the surgical field, as incorporation of the fragments into the fixation construct leads to a high rate of avascular necrosis
The CT images shown in Figures C and D display significant marginal impaction of the joint surface.
Marginal impaction is common in posterior wall fractures and fracture-dislocations. Critical review of CT imaging of posterior wall fractures can help with preoperative planning for identifying impaction of the articular surface of the acetabulum. Restoration of the sphericity of the acetabulum to match that of the femoral head is important for successful outcome following ORIF of posterior wall fractures. A common surgical technique to accomplish joint surface restoration includes freeing the impacted articular segments, bone grafting of the void created to support the articular segments, and buttress plating of the posterior wall fracture fragments.
Patel et al. discuss the challenge of interpreting imaging of the acetabulum for assessing fracture characteristics that may significantly impact success or surgical intervention. These characteristics include: articular displacement, marginal impaction, incongruity of the joint surface, intra-articular fragments, and osteochondral injury to the femoral head. Based on expert review of images, determination of significant marginal impaction had a poor intraobserver reliability, as did each of the other modifiers listed.
Figures A and B are radiographs of the posterior wall fracture and hip dislocation. They do not show the large amount of marginal impaction of the acetabular surface. Figure C (coronal reconstruction) and Figure D (sagittal reconstruction) point out a large a amount of marginal impaction of the acetabular. Note the disruption of the joint surface on the intact portion of the acetabulum.
Incorrect answers:
Comminuted posterior wall fractures still should be surgically stabilized if the joint is unstable
This impacted fragment on the margin of the main fracture line will likely heal regardless of restoration of the articular surface; however, this malreduction will lead to a incongruent joint surface
These CT cuts do not show any osteochondral defects of the femoral head; however if found in other CT cuts or intraoperatively, they should be appropriately addressed
Intraarticular fracture fragments should be removed from the joint, but if they make up a substantial portion of the joint surface, they should be incorporated in the fixation construct to obtain the goal of anatomic reduction of the joint surface
OrthoCash 2020
A 32-year-old female is involved in a motor vehicle collision and suffers a right hip dislocation. She is in the twelfth week of pregnancy.
Evaluation in the emergency department reveals no other injuries and ultrasound reveals a strong fetal heart rate and no abnormalities. She undergoes emergent closed reduction but the hip remains unstable and a traction pin is placed. Post-reduction films are shown in Figure
What is the most appropriate next step in management?

Acute open reduction internal fixation
Exam under anesthesia
Skeletal traction for 6-8 weeks
Fetal monitoring until 15 weeks followed by open reduction internal fixation
Percutaneous pinning
This patient has a large posterior wall fracture of the right acetabulum with an unstable hip. The most appropriate next step in treatment is open reduction and internal fixation.
Fixation of acetabular fractures during pregnancy is not contraindicated in the setting of stable fetal heart rate and no abnormalities on pelvic ultrasound.
There is, however, an increased risk of complications for the mother and fetus. Injury severity and mechanism are most closely associated with increased rate of fetal complications. The trimester of pregnancy is not associated with increased risk of complications.
Leggon et al. reviewed 101 cases of pelvic and acetabular fractures in pregnant patients and found mechanism of injury and injury severity were associated with higher mortality for both mother and fetus. Trimester of pregnancy was not associated with increased mortality.
Flik et al. reviewed orthopaedic trauma in a pregnant patients and recommended fetal ultrasound for assessment of fetal well-being in all pregnant patients.
Desai et al. investigated orthopaedic trauma during pregnancy and reported minimal radiation risk to the fetus when obtaining x-rays. They also advocate for LMWH as one of the safest choices for anticoagulation.
Figure A is an x-ray showing a right posterior wall acetabular fracture. Figures B and C are Judet views of the pelvis focusing on the right hip. A large posterior wall fragment is visible in Figure B.
Incorrect Answers:
OrthoCash 2020
Figure A is radiograph of a 50-year-old male science teacher that was involved in a motor vehicle accident. He underwent closed reduction as seen in Figure B and C. What would be the most appropriate treatment?

Open reduction and internal fixation with medial bridge plate and lateral screw in non-lagging mode
Tibiotalocalcaneal arthrodesis
Open reduction and internal fixation with lateral and medial screw in lagging mode
Closed reduction and internal fixation with medial and lateral screw in non-lagging mode
Closed reduction with percutaneous pins Corrent answer: 1
This patient is presenting with a Hawkins II talar neck fracture with medial wall comminution. The most appropriate treatment of this patient would be open reduction internal fixation with medial plate and lateral screw in non-lagging mode.
The treatment of talar fractures is based on the severity of the fracture, soft-tissues, and patient factors. The fracture and subluxation of the subtalar joint should be reduced and stable anatomical fixation should be obtained. When there is comminution of either the superior, lateral or medial aspects of the talus, one should avoid shortening the medial wall as this will cause a varus malunion. The use of a medial or lateral plate can help to re-establish column length, which can often prevent this potential complication.
Sanders et al. showed significant complications after fixation of talar neck fractures. They showed the incidence of secondary reconstructive procedures following talar neck fractures increased from 24% +/- 5% at 1 year to 48%
+/- 10% at 10 years post-injury.
Vallier et al. retrospectively reviewed the records of 39 fractures of the talar neck treated with open reduction and internal fixation. Twenty-one (54%) of thirty-nine patients had development of posttraumatic arthritis, which was more common after comminuted fractures (p < 0.07) and open fractures (p = 0.09).
Vallier et al. reviewed 81 talar neck fractures to revisit the rate of osteonecrosis and post-traumatic arthritis based on the Hawkins Classification. They found that delaying definitive internal fixation does not increase the risk of developing osteonecrosis. Thirty-five patients (54%) developed posttraumatic arthritis, including 83% of those with an associated talar body fracture (p < 0.0001) and 59% of those with Hawkins type-III injuries (p < 0.01).
Figure A shows a Hawkins II talar neck fracture. Figures B and C are saggital and coronal CT images, respectively, of the foot. There is significant comminution of the medial wall of the talus with extension into the subtalar joint.
Incorrect Answers:
There is some research to suggest primarily subtalar arthrodesis with these injuries. However, to date, there is no high level evidence that has conclusively shown subtalar arthrodesis to be better than ORIF.
OrthoCash 2020
A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?

Age less than 30
Marijuana use
Use of negative pressure wound therapy
Male gender
Ability to return to work Corrent answer: 5
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
4: These options are not as strong of a factor of patient satisfaction in longterm follow up after trauma-induced lower extremity amputation.
OrthoCash 2020
A 34 year-old male falls off of motorcycle on an outstretched hand suffering the injuries shown in Figures A and B. He is brought to the operating room and undergoes radial head replacement and fixation and repair of the coronoid and the lateral collateral ligament (LCL). Prior to closing, the elbow is still unstable upon testing range of motion. What is the next best step in management?

Exchange radial head for larger implant
Complete resection of radial head
Cast at 90 degrees of flexion for 6-8 weeks
Reinforce LCL repair with non-absorbable suture
Repair the ulnar collateral ligament Corrent answer: 5
Following complete fixation and repair of a terrible triad, a final range of motion test should be performed prior to closure. If still unstable, the next step should be to assess and repair the ulnar collateral ligament. Another option
would be to placed a hinged external fixator.
Operative reconstruction of a terrible triad injury should be performed in a systematic fashion, working from deep to superficial. Working through a lateral incision and through the radial head fracture, the coronoid should be fixed first, followed by radial head fixation or replacement and then repair/reconstruction of the LCL. If still unstable, the medial side should be addressed, or the patient placed in a hinged external fixator.
Mathew et al review the anatomic, biomechanic, and operative principles (why the above step-by-step method works) to achieving appropriate stability in order to obtain early range of motion to maximize clinical outcome.
Pugh et al. in this retrospective, multi-center study report outcomes on 36 terrible triad injuries fixed with the standard protocol described above. The authors recommend following this systematic approach to achieve the best results.
Figures A and B are AP and lateral radiographs exhibiting a terrible triad elbow fracture-dislocation.
Incorrect answers:
OrthoCash 2020
When treating the pathology depicted in Figures A through D, which of the following is necessary to preserve the blood supply to the femoral head?

Dissection of the gluteal musculature off the iliac crest
Ligation of the ascending branches of the lateral femoral circumflex artery
Greater trochanteric osteotomy
Identification and detachment of the piriformis tendon
Supine positioning
Figures A-D show a femoral head with associated acetabular fracture (Pipkin IV). Both the posterior wall fracture and the femoral head fracture can be addressed through a surgical dislocation via greater trochanteric osteotomy.
Pipkin IV femoral head fracture (with associated acetabular fractures) are somewhat problematic in that the femoral head fracture is usually anterior, while the acetabular fracture usually involves the posterior wall. A Kocher-Langenbeck approach gives good access to the posterior wall but limited access to the articular surface and femoral head avascular necrosis (AVN) is a concern. A Smith-Peterson approach provides good access to the femoral head
but not to the posterior wall. Combined approaches significantly increase the amount of surgical dissection. Surgical dislocation with trochanteric flip osteotomy provides access to the femoral head and posterior wall while preserving blood supply to the femoral head.
Solberg et al. retrospectively reviewed 12 patients with Pipkin IV injuries treated via a trochanteric flip osteotomy. All patients healed their acetabular fractures. Eleven of 12 patients healed their femoral head fractures and one patient (8.3%) developed osteonecrosis.
Henle et al. likewise treated 12 patients with Pipkin IV injuries through a trochanteric flip osteotomy. Two of 12 patients (16.7%) developed osteonecrosis. The remaining 10 patients (83.3%) had good or excellent results. Heterotopic ossification occurred in five patients, causing significant range of motion loss in four of these.
Figure A is a pre-reduction AP pelvis in which the posterior wall fracture is apparent. Figure B is a post-reduction AP pelvis in which an infra-foveal femoral head fracture is apparent (Pipkin IV). Figure C is an axial CT cut which further characterizes the posterior wall fracture. Figure D is an obturator oblique showing femoral head dislocation and posterior wall fracture. The video shows a surgical hip dislocation technique.
Incorrect Answers:
OrthoCash 2020
A 42-year-old male presents to your clinic for the first time with the radiographs seen in Figure A. He sustained the injury 4 weeks ago while skiing overseas and treatment was provided by the local orthopaedic surgeon. The operative note states that he sustained an Gustilo Type I open fracture. After surgical fixation of this type of injury, what is the most common complication requiring reoperation?

Chronic elbow instability
Post-traumatic arthritis
Infection
Heterotopic ossification
Loss of elbow range of motion Corrent answer: 5
This patient sustained a terrible triad elbow fracture-dislocation. Reduced range of motion of the elbow joint is the most common complication REQUIRING reoperation with these injuries.
Terrible triad elbow fracture-dislocations are characterized by posterolateral dislocation/lateral collateral ligament (LCL) injury, radial head fracture and coronoid fracture. Displaced fractures result in elbow instability. Acute radial head stabilization, coronoid open reduction and internal fixation, and LCL +/-medial collateral ligament (MCL) repair/reconstruction is considered the most appropriate treatment for displaced fractures. Operative complications include elbow stiffness, recurrent instability, arthritis, failure of hardware, heterotopic ossification, posterior interosseous nerve palsy and infection.
Egol et al. looked at the functional outcomes of 27 patients that underwent fixation of terrible triad injuries. At one year follow-up, the average flexion-extension arc of elbow motion was 109 degrees +/- 27 degrees, and the average pronation-supination arc was 128 degrees +/- 44 degrees. Grip strength averaged 72% of the contralateral extremity. Although operative fixation led to functional elbow stability, results were poor.
They included a reference to McKee et al. to highlight that intra-articular fractures of the elbow have high rates of stiffness. While not specific to terrible
triads, they looked at the effectiveness of the posterior elbow approach in 25 patients that underwent internal fixation of intra-articular distal humerus fractures. They showed poor outcomes at a mean follow-up of 36 months with reduced range-of-motion, decreased strength and high re-operation rates.
Figure A shows AP fluoroscopic image of a terrible triad injury that has undergone operative fixation. The radial head and coronoid have undergone open reduction internal fixation, and the MCL bony avulsion has been repaired.
Incorrect Answers:
OrthoCash 2020
Figure A is a radiograph from a 59-year-old male that was transferred to a Level I trauma center five hours after a motor vehicle accident. Closed reduction and skeletal traction was successfully performed in the trauma bay. Which of the following factors has been shown to increase the risk of unsatisfactory clinical outcome for this patient?

Need for skeletal traction
Mechanism of injury
Gender
Age
Time to reduction Corrent answer: 4
Age greater than 55-years-old has been found to be an independent risk factor for inferior clinical outcome in patients with combined acetabular fractures and hip dislocations.
The most important initial step in management following resuscitation involves urgent reduction of the dislocated hip. This should be followed by a preoperative CT scan and ultimately surgical fixation of the combined acetabular fracture. Hip dislocations should be reduced within 6-12 hours for optimal outcome, although different critical times have been cited, particularly for dislocations with concomitant acetabular fractures. Skeletal traction may be required to maintain hip reduction.
Moed et. al. present a Level 3 retrospective review of 100 patients who had been treated with open reduction internal fixation of an acetabular fracture. The authors found that factors associated with unsatisfactory clinical outcomes included age greater than 55, intra-articular comminution, osteonecrosis, and delay of greater than 12 hours for reduction of an associated hip dislocation.
Additionally, they showed that there was a strong association of clinical outcome and final radiographic grade.
Figure A demonstrates an acetabular fracture with concomitant hip dislocation. Incorrect Answers:
injury, male gender, and time to reduction <6 hours have not been shown to be related to unsatisfactory outcomes.
OrthoCash 2020
A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?

Varus malunion
Nonunion
Valgus malunion
Malrotation
Superficial peroneal nerve injury Corrent answer: 3
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Varus malunion is more likely to occur in midshaft tibia fractures with an intact fibula.
Nonunion after a proximal tibial fracture treated with intramedullary nailing is less common than malunion.
Malrotation occurs most commonly after IM nailing of fractures through the distal third of the tibia.
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.

OrthoCash 2020
A 24-year-old motorcyclist is brought in as a polytrauma after striking a tree at 65 mph. He is found to have injuries involving the chest, abdomen, pelvis, as well as a left open femoral shaft fracture. He undergoes resuscitation in the trauma bay. Which of the following parameters best supports proceeding with irrigation, debridement and external fixation as opposed to immediate reamed intramedullary nailing?
Temperature = 35.5°C (95.9°F)
Fractures of ribs 2-3 with left apical pneumothorax
Grade IV liver laceration with SBP = 85 mmHg
Left superior and inferior pubic ramus fractures
Lactate = 2.3 mg/dL
Significant abdominal trauma with evidence of hemorrhagic shock (SBP < 90 mmHg) following resuscitation is an unstable parameter and therefore is an indication to proceed with damage control orthopaedics (irrigation and debridement of open fractures and temporizing external fixation) in a polytraumatized patient.
The management of orthopaedic injuries in a polytrauma patient depends on the physiological stability of the patient. In an unstable patient, damage control orthopaedics (DCO) is preferred over early total care (ETC) to avoid an iatrogenic second hit with development of adult respiratory distress syndrome (ARDS) and/or multiple organ failure. Clinical parameters indicative of instability include shock (BP < 90 mmHg, refractory to blood products, lactate
> 2.5 mg/dL), coagulopathy (platelet count < 90,000 mm3, fibrinogen < 1 g/L), hypothermia (< 35°C), and significant chest, abdomen or pelvis injuries (pulmonary contusions, severe liver/spleen lacerations, pelvic ring disruption).
Pape et al. (2009) authored a review article detailing the management of a multitrauma patient. Polytrauma patients can be classified as stable, borderline, unstable or in extremis using a variety of criteria pertaining to hemodynamic stability, coagulation, temperature and soft tissue injury.
Patients who are stable or borderline can undergo ETC, while patients who are unstable or in extremis should be managed with DCO.
Pape et al. (2008) concluded that all patients who underwent early femoral nailing demonstrated increased systemic inflammatory response compared to external fixation, regardless of clinical stability. However, unstable patients
with a preexisting elevation of inflammatory status are likely more impacted by this additional increase. Improved postoperative clinical status coincided with a less vigorous inflammatory response.
Illustration A is a table from Pape et al (2009) depicting the criteria used to determine clinical condition of a polytraumatized patient. Illustration B is an algorithm from Pape et al (2009) detailing management of the multitrauma patient.
Incorrect Responses:
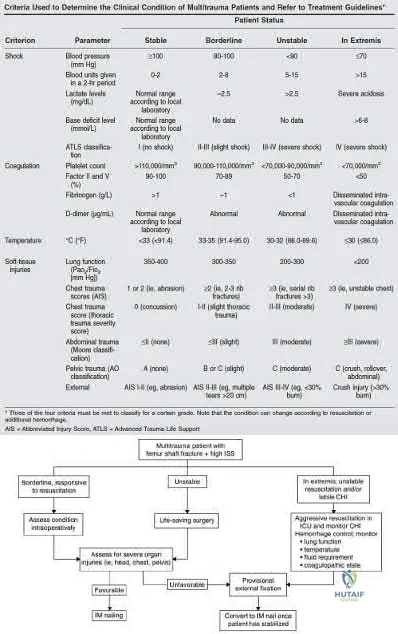
OrthoCash 2020
A 92-year-old female sustains the injury shown in Figure A to her nondominant extremity as the result of a non-syncopal ground-level fall. She denies any previous injury or pain of the elbow, and her medical history is significant only for osteoporosis and hypothyroidism. What is the most appropriate treatment for her injury?

Immediate range of motion as tolerated with a sling for comfort
Long arm cast for 3 weeks, then physical therapy for motion
Open reduction and internal fixation
Radiocapitellar arthroplasty
Total elbow arthroplasty Corrent answer: 5
Use of total elbow arthroplasty (TEA) in the elderly is a well-recognized method of treatment of complex distal humerus fractures. This procedure allows for improved ROM, improved patient-reported outcomes, and decreased revision rates as compared to fixation.
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, which is important, as most recommendations list restrictions of lifting no more than 5-10 pounds postoperatively.
McKee et al conducted a prospective, randomized, controlled trial to compare functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary semiconstrained total elbow arthroplasty (TEA). Patients who underwent TEA had a quicker procedure, improved DASH scores at 6 months, improved elbow ROM, and decreased revision rates.
Athwal et al review TEA and the options available at the time of publication. They also report on the techniques and purported advantages of arthroplasty as compared to fixation of complex distal humerus fractures.
Frankle et al reviewed patients >65 years old with distal humerus fractures at a minimum of 2 years follow-up. Outcomes were excellent in 33% of cases undergoing ORIF and 92% excellent with TEA. They recommend TEA in instances of arthritis, osteoporosis, or other diagnoses requiring steroids.
Figure A shows a significantly comminuted distal humerus fracture in an osteoporotic patient. Illustration A shows the same patient after undergoing total elbow arthroplasty.
Incorrect Answers:
1:Immediate range of motion is not recommended for this injury, even with the "bag of bones" treatment method. A brief period of immobilization is generally recommended for this technique.
2: Casting is not indicated for this injury.
3: ORIF of this injury will lead to worse outcomes as compared to arthroplasty. 4: Isolated radiocapitellar replacement is not indicated for this injury.

OrthoCash 2020
A 56-year-old right hand dominant attorney falls from standing and sustains the closed injury shown in Figure A. The treating surgeon elects to fix her fracture using a plate and screw construct. Based on
the available imaging, which of the following fracture characteristics best justifies this fixation choice?

Fracture displacement
Intra-articular fracture extension
The fracture extends distal to the coronoid
Oblique fracture line
Fracture comminution
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on interfragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation
was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
OrthoCash 2020
A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries?

Bilateral open reduction and internal fixation
Open reduction internal fixation on the right, reamed intramedullary nailing on the left
Temporizing external fixation on the right, open reduction and internal fixation on the left
Bilateral reamed intramedullary nailing
Bilateral temporizing external fixation Corrent answer: 5
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which
carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
OrthoCash 2020
Which of the following has been shown to be the greatest risk factor for refracture after implant removal from a radial shaft?
Removal of locking screws
Removal of small fragment plates
Removal of metaphyseal implants
Removal of implants less than 1 year after insertion
Removal of protective splinting from limb earlier than 10 weeks postoperatively
Removal of implants earlier than 1 year after insertion is a risk factor for refracture of the bone after implant removal.
The risk of refracture after hardware removal is multifactorial. Multiple
variables have been studied such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The variable that seems to correlate most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are also at higher risk for refracture in the forearm.
Deluca et. al reported on a case series of patients who sustained a refracture of a forearm after implant removal. They noted that radiolucency at the site of the original fracture was seen in most refractured patients when the plate was removed. They also recommend delaying implant removal to two years after insertion to minimize risk.
Rumball et. al reported that the incidence of refracture after forearm implant removal is 6% in their series. They found that early removal, lack of postoperative immobilization, and plate size are the most critical risk factors for refracture.
Illustration A shows a forearm with evidence of refracture after implant removal.
Incorrect Answers:

OrthoCash 2020
A 23-year-old male arrives to the trauma bay after a motorcycle crash caused by a drive-by shooting. The patient is awake and alert and following commands. Vital signs include a blood pressure of 145/90 and a heart rate of 117bpm. Initial lactate is reported as 2.4 mmol/L. The patient has 2 rib fractures on the right with a clear chest radiograph. The patient is neurovascularly intact with a 4cm transverse wound over the medial ankle. Figures A, B and C exhibit his orthopaedic injuries. What is the most appropriate management?

Irrigation, debridement and placement external fixator right ankle, external fixation femur and intramedullary fixation tibia
Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and tibia
Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and external fixation tibia
Irrigation, debridement and placement external fixator right ankle, femur and tibia
Irrigation, debridement and external fixation right ankle and skeletal traction
The patient is relatively hemodynamically stable. In this case the femur and tibia should be definitively fixed while the open ankle fracture can be irrigated and debrided and placed in a spanning external fixator, temporizing for later definitive fixation.
Aside from an elevated heart rate and mildly elevated lactate (normal < 2.5 mmol/L), the patient is relatively stable making him a good candidate for long bone stabilization and temporizing external fixation of the right ankle. Gross contamination of the open injury also supports temporizing fixation, which can be brought back for repeat I&D and possible fixation.
Pape et al. compared outcomes for intramedullary nailing (IMN) versus staged fixation for femur fractures in stable versus borderline patients. Borderline patients were defined as those with multi-system injury (especially to lungs) and exhibited higher lung complications following acute IMN when compared to stable patients with isolated orthopaedic injuries.
O'Brien reviewed the literature regarding early total care in regards to IMN stabilization of femur fractures. Summarized data noted isolated injuries treated with early IMN had good outcomes, whereas those with head or lung injury had worse outcomes and pulmonary complications.
Figure A exhibits a right open ankle fracture dislocation. Figure B exhibits a mid-shaft tibia fracture. Figure C exhibits a ballistic mid-shaft femur fracture.
Incorrect Answers:
OrthoCash 2020
Figure A is an anterior-posterior (AP) radiograph of a 27-year-old male who was a bicyclist struck by a motor vehicle. He was intubated in the field and unresponsive in the trauma slot. Ultrasound of his abdomen is positive for blood and he is brought to the operating room emergently for an exploratory laparotomy. He is found to have ischemic bowel and a grade 4 liver laceration. His lactate is 9.0 mg/dL. Which figure represents the next appropriate step in regard to his pelvic ring injury?
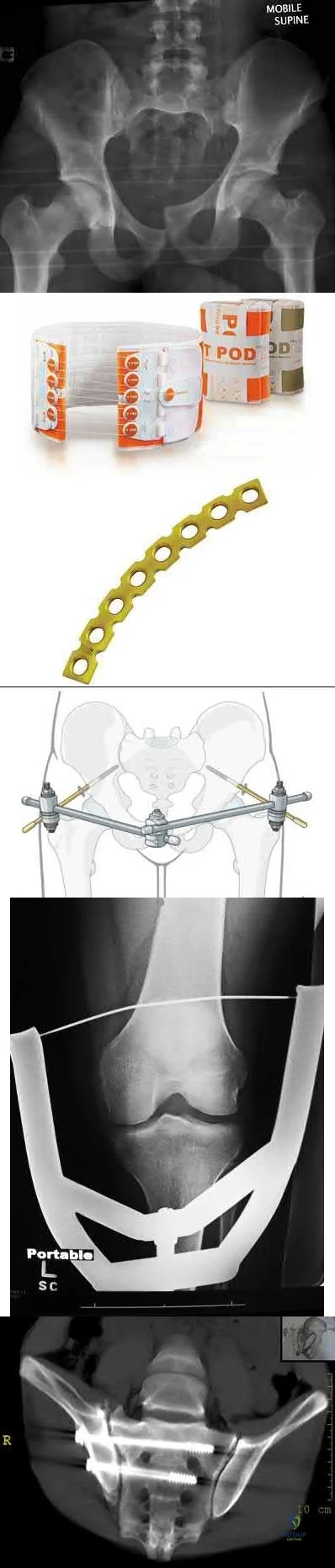
The radiograph exhibits an elevated left hemipelvis with complete sacroiliac disruption, which can be temporized with placement in skeletal traction.
The patient is unstable, as indicated by an elevated lactate level. The most appropriate next step is temporizing skeletal traction to reduce the left hemipelvis.
Langford et al. review the initial diagnosis, evaluation and resuscitation in the management of pelvic fractures. Reduction of pelvic volume can be achieved with pelvic binders and temporizing external fixation for anterior posterior compression (APC) and/or lateral compression (LC) fracture patterns, while skeletal traction can help do the same in vertical shear patterns.
Matullo et al. review the uses of skeletal traction in orthopaedic trauma, where lower extremity skeletal traction can be an efficient, fast, easy way to help reduce pelvic volume in vertical shear injuries, especially when the patient is unstable and not cleared for definitive fixation.
Figure A exhibits an elevated left hemipelvis indicative of a vertical shear injury and complete SI disruption. Figure B is an example of a pelvic binder. Figure C is a pelvic reconstruction plate. Figure D is a schematic of an anterior pelvic external fixator. Figure E is a schematic drawing of a patient in lower extremity
skeletal traction. Figure F is a radiograph exhibiting S1 and S2 sacroiliac (SI) screws.
Incorrect answers:
OrthoCash 2020
A 38-year-old man is involved in a motor vehicle collision and suffers the grossly open injury shown in Figure A. He subsequently undergoes irrigation and debridement and placement of an external fixator. In Figure B, if the proximal pin is placed at the red circle as compared to the black circle, the patient is at increased risk for which of the following?

Foot drop
Injury to the anterior tibial artery
Septic arthritis
Flexion contracture of the knee
Patellar tendon rupture Corrent answer: 3
The patient is at increased risk of septic arthritis when placing the proximal tibial pin too proximal due to penetration of the joint capsule. Pin site flora can track into the joint and lead to a septic knee.
Tibial external fixators can be used to temporize tibial shaft, pilon, and ankle fractures not ready for definitive management due to soft tissue concerns and/or practice of damage control orthopaedics. Intracapsular placement of fixator pins can lead to septic arthritis. The capsular reflection typically extends 14 mm distal to the subchondral line.
DeCoster et al. reported a cadaveric dissection study for safe placement of proximal tibia pins and determined that the capsule inserts 14 mm below the articular surface along the posteromedial and posterolateral surfaces. For fractures requiring extremely proximal pin placement, they recommend
anterior cortex penetration only at least 6 mm distal to articular surface.
Reid et al. investigated safe transtibial pin placement using MRI and cadaveric and volunteer knees. They found that pin placement 14 mm distal to subchondral bone will result in low likelihood of capsular penetration.
Figure A is an AP radiograph showing a segmental middle third tibia/fibula fracture. Figure B is a lateral diagram of the tibia showing potential sites of proximal pin placement.
Incorrect Answers:
OrthoCash 2020
Figures A and B are radiographs of a 43-year-old, right-hand dominant, male that injured his arm in a motor vehicle accident. What would be an absolute indication for surgical fixation of his injury?
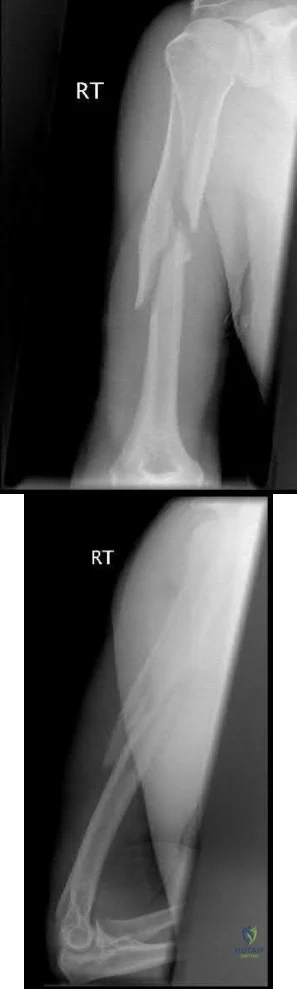
Radial nerve palsy
Intra-articular extension
2mm fracture distraction, 5 degrees of rotational malignment
Ipsilateral proximal both bone forearm fracture
Bilateral fracture
This patient has a humeral shaft fracture. An absolute indication for surgery would include a floating elbow, i.e. ipsilateral both bone forearm fracture.
The primary causes of humeral fractures include motor vehicle accidents, falls, or violent injury. Almost all cases are treated non-operatively with functional bracing. The absolute indications for surgical management include: ipsilateral vascular injury, severe soft-tissue injury, open fracture, compartment syndrome, and associated ipsilateral forearm fracture, ie, floating elbow. The relative indications for surgical management include: segmental fracture, intraarticular extension, significant fracture distraction, bilateral humeral fracture, inability to maintain acceptable alignment, and polytrauma.
Klenerman et al. reviewed non-operative treatment of humeral shaft fractures. They showed that acceptable results could be achieved even after 20° of
anterior bowing, 30° of varus angulation, 15° of malrotation, and 3 cm of shortening.
Carroll et al. reviewed the management of humeral shaft fractures. They state the indications for operative fixation to be polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical techniques include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing
Figure A and B shows a comminuted mid-shaft humeral fracture with intraarticular extension.
Incorrect Answers:
OrthoCash 2020
Which of the following findings is a contraindication in retrograde nailing of a periprosthetic distal femur fracture around a total knee arthroplasty?
Posterior-stabilized total knee implant
Cruciate retaining total knee implant
Spiral fracture pattern
Distal femoral replacement
Knee flexion contracture of 15 degrees Corrent answer: 4
A distal femoral replacement (TKA) implant will generally preclude placement of a retrograde nail due to the long stem on the femoral component.
Supracondylar femur fractures above a well-fixed TKA component are increasingly common. These fractures are often treated with a lateral locking plate, but can also be treated with a retrograde nail in certain circumstances. An important factor in determining if nailing is a viable option are knowing the TKA implant and it's design. In addition, if the TKA component is known, the maximum size of reamer head and nail can be determined preoperatively from the size of the femoral 'box'.
Schutz et al report on a prospective multicenter study of 112 patients who underwent fixation of a distal femur fracture with the LISS system. They report that 90% of fractures went on to union and they attribute all of the failures to either the high-energy nature of particular fractures or a lack of experience in applying the plate in an appropriate pattern. They also note that primary grafting of these fractures is not necessary.
Illustration A shows a periprosthetic femur fracture treated with a retrograde nail.
Incorrect Answers:
1: A posterior-stabilized implant can be treated with an intramedullary nail in many circumstances but can be technically challenging, depending on the components.
2: A cruciate retaining TKA is not a contraindication to use of a retrograde nail. 3: A spiral pattern periprosthetic supracondylar femur fracture can be treated with a femoral nail.
5: A knee flexion contracture will often provide the flexion necessary for access to the box of the femoral component. A knee extension contracture, however, can preclude access to this box for placement of a nail.

OrthoCash 2020
A patient falls and sustains the isolated injury seen in Figures A and B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?

Full pronation
25 degrees pronation
Neutral
25 degrees supination
Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with < 3 fragments. Radial head replacement is considered for comminuted
fractures (Mason Type III) with 3 or more fragments.
Cheung et al. reviewed the surgical approaches to the elbow. The lateral approach (Kocher or Kaplan) is most commonly used with these injuries. The Kocher approach utilizes the intramuscular plane between anconeus and extensor carpi ulnaris. Kaplan utilizes the plane between extensor digitorum commons and extensor carpi radialis brevis.
Figure A and B show AP and lateral radiographs of the left elbow. There is a displaced radial head fracture. Illustration A shows a schematic diagram of the radial head "safe zone" between the radial styloid to Lister's tubercle.
Incorrect Answers:
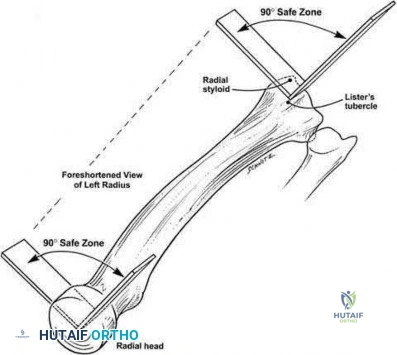
OrthoCash 2020
A 38-year-old male is involved in a high speed motor vehicle collision. He has a Glasgow Coma Scale of 13 and receives 2 liters of fluid en route to the emergency department. Upon evaluation in the emergency department, he is found to have a bilateral femoral shaft fractures, a right ankle fracture, and a left both bone forearm fracture. He also has 2 left sided rib fracture and a grade II liver laceration. His heart rate is 130 and blood pressure is 85/50. All of the following
would be indications to practice damage control orthopaedics in this patient except:
Bilateral femur fractures
Rib fractures
Lactate of 5.2
Urine output of 20 cc/hr
Heart rate and blood pressure Corrent answer: 2
Rib fractures without evidence of further thoracic trauma would not be an indication to practice damage control orthopaedics. This patient is underresuscitated based on his lactate level, urine output, and vital signs and definitive management should be delayed.
Damage control orthopaedics is the practice of delaying definitive management of fractures and utilizing temporary stabilization (such as an external fixator) until a patient has recovered from the initial physiologic insult of trauma.
Patients are at increased risk for perioperative complications such as ARDS and multi-system organ failure during the acute period after polytrauma. In addition to underresuscitation, other indications to practice damage control orthopaedics include: injury severity score>40 (or >20 with thoracic trauma), bilateral femoral fractures, hypothermia below 35 degrees Celsius, and pulmonary contusions.
Pape et al. (2007) studied the incidence of acute lung injuries in polytrauma patients undergoing either intramedullary nailing or external fixation and later definitive fixation of femoral shaft fractures. They found that patients undergoing immediate intramedullary nailing were nearly 6.7 times more likely to have acute lung injury
The Canadian Orthopedic Trauma Society studied the effect of reamed versus unreamed femoral nailing on incidence of ARDS for femoral shaft fractures in trauma patients using a randomized controlled study. They found no difference between the groups.
Pape et al. also examined the pathophysiological cascades that accompany soft tissue injuries of the extremities, abdomen, and pelvis and recommend a more comprehensive for evaluation of patients with these injuries.
Incorrect Answers:
OrthoCash 2020
The anterior intrapelvic (modified Stoppa) approach is most appropriate for which of the following fractures?
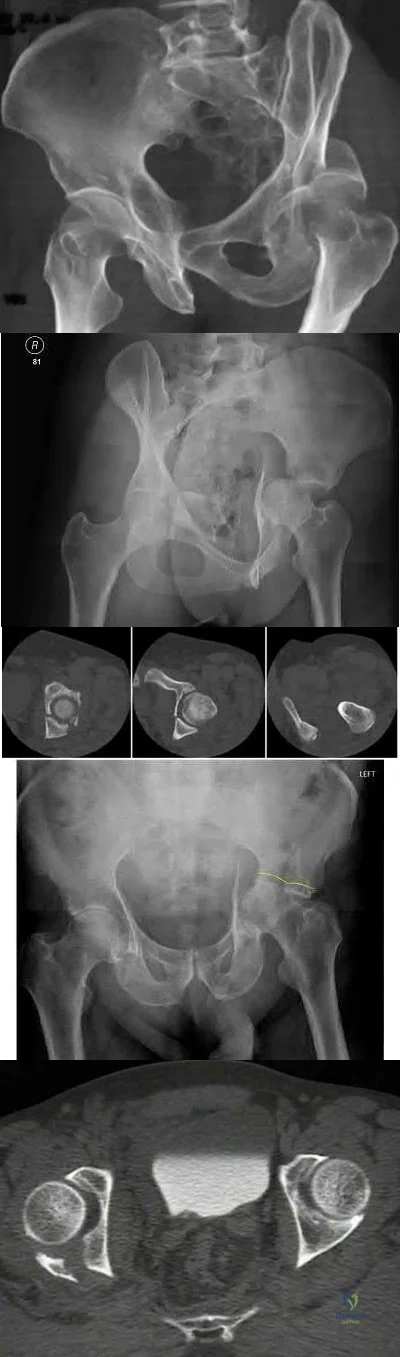
The anterior intrapelvic (AIP) or modified Stoppa approach provides access to the quadrilateral plate, which is a common location for fracture displacement in associated both column acetabulum fractures as seen in Figure D.
Compared to the traditional ilioinguinal approach, the modified Stoppa with a lateral window can offer comparable access to the quadrilateral plate, which can allow for its use in associated both column fracture patterns.
de Peretti et al. prospectively followed 25 patients with both column fractures
treated via an iliofemoral approach. Results led the authors to not recommend the extensile approach for both column fractures due to lack of efficiency and high complication rates.
Alonso et al. compared the extensile iliofemoral and triradiate approaches, and both reported acceptable results. However, concerning were the relatively high rates of heterotopic ossification, despite prophylaxis.
Bible al. performed a cadaver study to quantify the amount of access provided by the modified Stoppa approach. This approach provides access to approximately 80% of both the inner pelvis, and the quadrilateral plate, however, comparison to the ilioinguinal approach was not performed.
Shazar et al., in a cohort comparison between the ilioguinal and Stoppa approaches, noted better visualization and potential improve fracture reduction via the Stoppa approach for both column fractures. However, this study was limited in its retrospective and relative observer bias.
Figure A depicts a posterior wall fracture dislocation with concomitant femoral neck fracture. Figure B is an iliac oblique view which depicts a posterior column fracture. Figure C exhibits a posterior column + posterior wall fracture. Figure D depicts acetabular fracture with protrusio. Figure E exhibits a posterior wall fracture.
Incorrect answers:
OrthoCash 2020
Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated nonoperatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?

Hand dominance
Angulation of fracture
Smoking
Early physical therapy
Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with non-operative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to
impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than non-smokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
OrthoCash 2020
A 26-year-old male epileptic patients presents with right shoulder pain and deformity after a grand mal seizure. After medical stabilization, he denies previous injury to his shoulder. Pre-reduction and post-reduction radiographs of the shoulder are shown in Figures A-C, respectively; physical examination reveals a normal upper extremity neurovascular examination. After shoulder immobilization, what would be the next most appropriate step in management of this patient?

Abduction brace for three weeks, followed by therapy
Right shoulder MR arthrogram
Open reduction and internal fixation
Hemiarthroplasty
Early range of motion Corrent answer: 3
This patient has presented with a fracture dislocation of the right shoulder. After urgent closed reduction, this patient requires open reduction internal fixation of the proximal humerus, and greater tuberosity fracture fragment in particular.
Isolated greater tuberosity fractures may be associated with shoulder dislocations. Careful review of imaging is critical to identify fracture lines that may extend into the humeral neck and head. If these extensions go undetected, catastrophic propagating fractures may occur during closed reduction maneuvers. Treatment is usually with open reduction internal fixation (ORIF). Young patients with proximal humerus fractures should be treated more aggressively with ORIF as compared to elderly patients. Another example would be a severely impacted valgus proximal humeral fracture in a young patient.
Erasmo et al. examined of 82 cases of humerus fracture dislocations treated with the lateral locking plates. Overall outcomes were excellent to good based on standard scoring systems. Complications included avascular necrosis (12%), varus positioning of the head (4.8%), impingement syndrome (3.6%), secondary screw perforation (3.6%), non-union (2.4%) and infection (1.2%).
Robinson et al. looked at severely impacted valgus proximal humeral fractures treated with open reduction internal fixation in young patients. Anatomic reduction is required with lateral plating to re-establish the normal head/neck angle. Good to excellent results can be achieved with fixation methods.
Figure A shows an anterior fracture-dislocation of the right shoulder. Figure B and C show post-reduction radiographs with a congruent glenohumeral joint. Displacement of the greater tuberosity (GT) fragment is greater than 5mm.
Incorrect Answers:
OrthoCash 2020
Pelvic packing can be performed to temporarily treat a hemodynamically unstable patient with a pelvic ring fracture. Which of the following is the preferred location of the skin incision to perform pelvic packing?
Right anterior superior iliac spine (ASIS) to mid-symphysis, left lateral window incision
Left ASIS to mid-symphysis, right lateral window incision
Subumbilical incision
ASIS to ASIS bilaterally
Pararectus incision
The preferred skin incision location is a subumbilical incision, 6-8cm extending upwards from the pubic symphysis towards the umbilicus; this allows access to all of the appropriate areas for pelvic packing.
Following skin incision, the rectus fascia is then divided in the midline which allows for access to both sides of the bladder for packing deep in the pelvic
brim. On each side, 3 lap pads are placed from sacroiliac joint to the retropubic space, all placed below the level of the pelvic brim.
Hak et al. review the options for emergent treatment in life threatening hemorrhage secondary to pelvic fractures. The authors offer several options for emergent treatment, which includes the use of pelvic binders, the placement of external fixators, pelvic packing and interventional angiography. Goals include reduction of pelvic volume and stopping rapid hemorrhage to save a patient's life. Pelvic packing, properly performed, is done through a subumbilical incision, as described above.
Osborn et al. retrospectively reviewed and compared emergent pelvic packing to angiography in hemorrhagic pelvic fracture clinical scenarios. The authors noted comparable results in mortality with a noted decrease in need for post-procedure transfusions in the pelvic packing group.
Cothren et al. reported their outcomes following an institutional algorithmic change from pelvic ex-fix/angiography to pelvic packing and ex-fix. Since their institutional change, the authors noted a significant decrease in transfusions, need for angiography and mortality.
Incorrect answers:
OrthoCash 2020
A 28-year-old man is brought by ambulance to the emergency department after falling from the roof of his home four hours ago. Upon initial evaluation, he has visible deformities of his bilateral lower extremities and a positive FAST exam. Heart rate is 135, blood pressure 85/58, and urine output is 40 cc over 3 hours. According to ATLS guidelines, what percentage of his blood volume has this patient likely lost?
Question 31
An year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 32
Delayed-onset muscle soreness (DOMS) is initially evident at the muscle tendon junction and can spread throughout the entire muscle. It is primarily associated with what type of exercise? Review Topic
Explanation
Question 33
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi Y: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7;223-227.
Question 34
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 35
- A skeletal survey is more accurate than a bone scan for detecting skeletal involvement in which of the following neoplastic diseases?
Explanation
Question 36
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 37
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 38
Which of the following is a function of siRNA (small interfering RNA)?
Explanation
siRNA are short (usually 20 to 24-bp) double-stranded RNA (dsRNA) sequences with phosphorylated 5' ends and hydroxylated 3' ends. Because of their ability to block a gene of interest, they have been generating interest in the treatment of disease processes that involve gene expression.
Noh et al. study the affects of PD98059, an extracellular signal-regulated kinase 1/2 (ERK1/2) inhibitor, on osteosarcoma. They found that blocking the ERK1/2 pathway with PD98059 induces osteosarcoma cell death by inhibiting a potential drug-resistance mechanism.
Illustration A shows how siRNA works to block translation of mRNA. Incorrect Answers:
Question 39
What is the most important predictor of functional outcome in patients with myelomeningocele?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 117-120.
Swank M, Dias L: Myelomeningocele: A review of the orthopaedic aspects of 206 patients treated from birth with no selection criteria. Dev Med Child Neurol 1992;34:1047-1052.
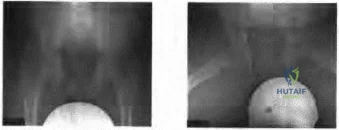
Figure 46a Figure 46b
Question 40
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren’s contracture?
Explanation
REFERENCES: McGrouther D: Dupuytren’s contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone,
1999, vol 1, pp 565-569.
McFarlane R: Patterns of diseased fascia in the fingers in Dupuytren’s contracture.
Plast Reconstr Surg 1974;54:31-44.
Question 41
A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 286.
Faraj AA, Davis TR: Percutaneous intramedullary fixation of metacarpal shaft fractures. J Hand Surg Br 1999;24:76-79.
Question 42
-Figure 39 is the anteroposterior radiograph of a marathon runner who has left groin pain that prevents her from running. She recently got back into her usual running routine after an ankle injury preventedbher from running for several months. She now has pain with any weight bearing. What is the most appropriate treatment option?
Explanation

Question 43
Which of the following is considered a contraindication to elbow arthroscopy? Review Topic
Explanation
Question 44
Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most likely to be injured?
Explanation
REFERENCES: O’Neill PA, Riina J, Sclafani S, et al: Angiographic findings in pelvic fractures. Clin Orthop 1996;329:60-67.
Belley G, Gallix BP, Derossis AM, et al: Profound hypotension in blunt trauma associated with superior gluteal artery rupture without pelvic fracture. J Trauma 1997;43:703-705.
Question 45
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient’s resuscitation can be described as which of the following?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury,
a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation endpoints: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 46
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 47
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Explanation
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 48
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.
Question 49
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 50
Figures 53a through 53d show the clinical photographs and radiographs of the lower extremity of a newborn male. Examination reveals this to be an isolated finding. The child otherwise has a normal neurologic examination. The hips are stable and there are no spinal defects. What is the most appropriate treatment at this time? Review Topic

Explanation
4 cm. The residual limb-length discrepancy presents the greatest challenge for orthopaedic management. This, however, can usually be handled with limb-lengthening techniques. Casting can be used for severe cases with unresolving significant contracture; however, gradual spontaneous correction is usually the norm. This condition is quite different from anterior lateral bowing that can be associated with neurofibromatosis and pathologic fracture or pseudoarthrosis of the tibia.
Question 51
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 52
An 82-year-old woman reports activity-related knee pain. History reveals that she underwent total knee arthroplasty 16 years ago. AP and lateral radiographs and a bone scan are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
well-defined borders. Joint space narrowing medially is consistent with polyethylene wear.
The most likely diagnosis is particle-mediated osteolysis. Metastatic tumors and primary sarcomas adjacent to an arthroplasty are extremely rare. In addition, malignant tumors and infection would more likely reveal a destructive lesion with poorly defined borders and increased uptake on a bone scan. Stress shielding with massive bone loss has not been described in knee arthroplasty literature, although this entity has been observed in fully porous-coated femoral implants in total hip arthroplasty.
REFERENCES: Robinson EJ, Mulliken BD, Bourne RB, et al: Catastrophic osteolysis in total knee replacement: A report of 17 cases. Clin Orthop Relat Res 1995;321:98-105.
Archibeck MJ, Jacobs JJ, Roebuck KA, et al: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Bugbee WD, Culpepper WJ, Engh CA Jr, et al: Long-term clinical consequences of stress-shielding after total hip arthroplasty without cement. J Bone Joint Surg Am 1997;79:1007-1012.
Question 53
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 54
- When taken concomitantly with which of the following, erythromycin can cause an increase in the blood level of
Explanation
Question 55
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
REFERENCES: Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496.
Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 56
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 295-297.
Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 379.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 23.
Ebraheim NA, Elgafy H, Xu R: Bone-graft harvesting from iliac and fibular donor sites: Techniques and complications. J Am Acad Orthop Surg 2001;9:210-218.
Question 57
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
Question 58
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 59
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
Explanation
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.

Question 60
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
Question 61
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
REFERENCES: Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 62
A 38-year-old man reports a 6-week history of shoulder pain and stiffness after falling on the stairs and landing onto the affected side. Radiographs are shown in Figures 54a and 54b. What is the most appropriate treatment? Review Topic

Explanation
Question 63
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?
Explanation
REFERENCES: Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Simonet WT, Cofield RH: Prognosis in anterior shoulder dislocation. Am J Sports Med 1984;12:19-24.
Question 64
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 65
Cell signaling through the activation of a transmembrane receptor complex formed by serine/threonine kinase receptors occurs with which of the following growth factors?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Schmitt JM, Hwang K, Winn SR, et al: Bone morphogenetic proteins: An update on basic biology and clinical relevance. J Orthop Res 1999;17:269-278.
Question 66
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
REFERENCE: Benassi MS, Magagnoli G, Ponticelli F, et al: Tissue and serum loss of metalloproteinase inhibitors in high grade soft tissue sarcomas. Histol Histopathol 2003;18:1035-1040.
Question 67
If additional posterior spinal surgery is performed to allow the patient to stand erect, the surgeon will need to advise the family about the risks of the procedure. In addition to risk for neurologic injury, what is the most likely complication?
Explanation
This case starts as standard degenerative spondylolisthesis but develops into a sagittal imbalance problem necessitating a major spinal procedure including
a pedicle subtraction osteotomy and extended posterior spinal instrumentation. Initially the patient had an L3-L5 posterior spinal fusion with a laminectomy and interbody fusion for an L4-L5 stenosis and degenerative spondylolisthesis. Two years after this procedure she is having difficult ambulation that improves with sitting. These symptoms are typical for neurogenic claudication associated with spinal stenosis. Adjacent segment degeneration leading to spinal stenosis is a common late complication associated with lumbar instrumented fusions, particularly in older patients. Figure 40b shows the adjacent segment degeneration at L5-S1 with the development of a degenerative spondylolisthesis. Degenerative spondylolisthesis is a radiographic sign of substantial degeneration of a disk space and is often associated with spinal stenosis. The primary procedure typically planned to address a degenerative spondylolisthesis is a laminectomy. An adjacent-level degenerative spondylolisthesis is typically instrumented and fused to the previous fusion construct.
The degeneration of the adjacent disk is also associated with a loss of disk height. A concern in this patient is the development of kyphosis at the L5-S1 disk space. Kyphosis at the lumbosacral junction can lead to sagittal imbalance issues. Spinal surgeons need to be aware of spinopelvic measurements to help prevent sagittal imbalance and proximal junctional failures. Improving the lumbar lordosis in this patient would necessitate restoration of the disk height at L5-S1. This can be accomplished with an interbody strut device placed either anteriorly or posteriorly via a posterolateral interbody approach at the time of the laminectomy.
This patient has undergone a posterior extension of her previous fusion without the addition of an interbody strut device. She now has further sagittal imbalance issues and an inability to stand erect without flexing her knees. This is a typical compensation posture that patients with significant sagittal imbalance acquire when trying to stand upright. Patients with sagittal imbalance are at increased risk for proximal junctional kyphosis or a more acute complication of proximal junctional failure.
The sagittal vertical axis is a plumb line dropped from C7 and should fall behind the hip joints and within 4 to 5 cm of the posterior corner of S1 (an easily identifiable radiographic marker). Pelvic incidence is a constant that is unique to each patient's spinopelvic anatomy. Pelvic incidence typically is within 10 degrees of the lumbar lordosis in an upright adult. Pelvic tilt (PT), on the other hand, can vary based on a patient's stance. PT is an indicator of the amount of compensation a patient has developed by retroverting their pelvis to stand upright. In an upright patient who is not compensating for loss of spinal sagittal alignment, the PT should be less than 20 degrees. In this case, the patient has a high PT and a significant lumbar lordosis/pelvic incidence mismatch with a significant positive sagittal imbalance (sagittal vertical axis of +8 cm). These are all indicators that a major spinal alignment procedure will be required to rebalance the spine. The use of posterior
osteotomies, such as a pedicle subtraction osteotomy, will be required if spinal realignment is planned. Pedicle subtraction osteotomies are considered 3-column osteotomies that remove the entire lamina, the facets, the pedicles (the posterior column), the underlying posterior vertebral wall and posterior vertebral body (middle column), and the underlying anterior vertebral body (anterior column) in a wedge fashion. Three-column osteotomies are associated with increased risk for neurologic injury and substantial blood loss. A Smith-Petersen osteotomy is a single-column posterior osteotomy that can provide a lesser amount of sagittal plane correction than pedicle subtraction osteotomy. A single-level Smith-Petersen osteotomy likely will not provide enough correction in this case.
RECOMMENDED READINGS
Lafage V, Schwab F, Vira S, Patel A, Ungar B, Farcy JP. Spino-pelvic parameters after surgery can be predicted: a preliminary formula and validation of standing alignment. Spine (Phila Pa 1976). 2011 Jun;36(13):1037-45. doi: 10.1097/BRS.0b013e3181eb9469. PubMed PMID:
Question 68
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 69
What is the most likely reason open fractures tend to heal more slowly than closed fractures?
Explanation
REFERENCES: Buckwalter JA, Einhom TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 377-381.
Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1-14.
2010 Pediatric Orthopaedic Examination Answer Book • 57
Question 70
A 10-year-old girl has a midshaft both bone forearm fracture. After attempted closed reduction, alignment consists of bayonet apposition, 10° of malrotation, and 8° of volar angulation. Management should now consist of
Explanation
REFERENCES: Do TT, Strub WM, Foad SL, et al: Reduction versus remodeling in pediatric distal forearm fractures: A preliminary cost analysis. J Pediatr Orthop B 2003;12:109-115.
Flynn JM: Pediatric forearm fractures: Decision making, surgical techniques, and complications. Instr Course Lect 2002;51:355-360.
Ring D, Waters PM, Hotchkiss RN, et al: Pediatric floating elbow. J Pediatr Orthop 2001;21:456-459.
Noonan KJ, Price CT: Forearm and distal radius fractures in children. J Am Acad Orthop Surg 1998;6:146-156.
Question 71
A 26-year-old woman who noted right-sided lumbosacral pain 10 days ago while vacuuming now reports that the pain has intensified. She denies any history of back problems. No radicular component is present, and her neurologic examination is normal. The next most appropriate step in management should consist of
Explanation
REFERENCES: Bigos S, Boyer O, Braen GR, et al: Acute low back pain in adults: Clinical practice guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD, Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, December, 1994.
Deyo RA: Conservative therapy for low back pain: Distinguishing useful from useless therapy. JAMA 1983;250:1057-1062.
Question 72
A Canale view best visualizes which of the following structures?
Explanation
REFERENCES: Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Bruden B: Roentgen examination of the subtaloid joint in fractures of the calcaneus. Acta Radiol 1949;31:85-91.
Question 73
9A 9B 9C 9D Figures 9a through 9d are the radiographs of a 21-year-old woman who is involved in a high-speed motor vehicle collision and sustains an isolated right closed-foot injury. Before surgery, the patient is advised about the relatively poor long-term outcomes associated with this injury. What is the most common reason for functional limitations after surgical treatment in this scenario?

Explanation
When a displaced talar neck fracture occurs, the rate of osteonecrosis is high; however, many revascularize the talus without collapse. A nonunion can occur but is less common than osteonecrosis and arthritis. A varus malunion can be debilitating and lead to subtalar arthritis. In a fracture with the talar body dislocated posteromedially (such as in this example) neurologic deficits in the tibial nerve distribution are common but typically improve with urgent
reduction. Studies show that posttraumatic subtalar arthritis is common after this injury and is the most likely cause of long-term functional impairment.
RECOMMENDED READINGS
Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. PubMed PMID: 15292407. View Abstract at PubMed
Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 10 THROUGH 12

10A

10B

10C
Figure 10a is the radiograph of a 30-year-old man who sustained an injury in a motor vehicle collision.
Question 74
-A 32-year-old man who is a smoker sustained an open tibial fracture and underwent a staged treatment with placement of an intramedullary nail. Four weeks after surgery, he developed a pseudomonas deepwound infection. What is the strongest predictor of persistent infection if implants are retained until fracture union?
Explanation

Question 75
An 8-year-old sustains the injury shown in Figures A and B. Postoperative radiographs are shown in Figures C and D. After cast removal and in-office k-wire removal, elbow range of motion is found to be between 20-80 degrees of flexion. How soon after surgery is range of motion expected to be >90% of normal? Review Topic

Explanation
Displaced pediatric supracondylar elbow fractures are often treated with closed reduction and percutaneous pinning. Risk of stiffness is low considering the extra-articular nature of the injury. Utility of physical therapy to improve range of motion after operative treatment of this injury is not supported in the literature.
Zionts et al. retrospectively evaluated elbow stiffness after treatment for pediatric supracondylar fractures. Ninety-four percent of normal range of motion was restored by 6 months after the operative procedure. Further improvement occurs up to one-year postoperatively
Lee et al. surveyed 76 orthopaedic surgeons on their treatment of pediatric supracondaylar injuries. They noted that general orthopaedic surgeons used passive exercises to assist with elbow stiffness after operative management of pediatric supracondylar fractures. In contrast, pediatric orthopaedists used active range of motion to improve elbow motion.
Keppler et al. retrospectively reviewed patients who had sustained supracondaylar fractures to ascertain the effect of postoperative physical therapy. At one year follow up, there was no difference in motion between patients who had received physical therapy and those who had not.
Figures A and B demonstrate the AP and lateral radiographs of a pediatric supracondylar fracture. Figures C and D are the postoperative radiographs after closed reduction and percutaneous pinning of the elbow injury.
Incorrect Answers:
(SBQ13PE.13) A 17-month-old boy is referred to your clinic by his pediatrician for a workup of "bowed legs." The patient's mother states that she has other children that grew out of it by age 3 or 4. Examination of the patient reveals a child whose measurements reside in the 75% percentile for height and weight. His gait appears appropriate for a toddler without varus thrust. Supine measurements show 10-degrees of symmetric, bilateral genu varus. Appropriate workup includes: Review Topic
Longterm clinical and radiographic monitoring to plan for guided growth until skeletal maturity
X-rays today and at age 4 to assure resolution of his genu varum
Genetic screening for metabolic causes of Rickets
Vitamin D levels drawn today and weekly 50,000 IU vitamin D injections assuming the value is low
Clinical observation and follow up to monitor resolution of genu varum
This patient has physiologic genu varum or tibia vara, which is common in toddlers less than 2 years of age. The mainstay of treatment is simple observation, as there is predictable resolution of this alignment as children
There are numerous etiologies of genu varum in children. Most common in the children under age 2 is a predictable pattern of genu varum and internal torsion in the first year or so after beginning to walk. Persistence of genu varum, severe (>20 degrees) or worsening deformity, limb asymmetry or varus thrust gait, and low height and weight percentiles should trigger further workup with x-rays and metabolic or genetic screening. A family history of genu varum is non-specific, and in isolation, does not indicate heritable causes of genu varum.
Kling and Hensinger's review article highlights normal angular and torsional deviations in growing children, including genu varum and genu valgum as well as hip and hind foot deformities. They emphasize that understanding the natural history of these deformities in growing children helps the treating physician identify those who need more than simple observation of their malalignment.
Staheli et al. published normal values of rotational profile physical exam maneuvers (including thigh foot axis, transmalleolar axis, prone internal and external hip rotation) to better understand the predictable changes in different age groups.
Birch provides an update on current treatment of Blount's disease. He suggests further radiographic evaluation in ambulatory infants with asymmetric varus deformity or varus deformity that persists after age 18 months. If these findings are present, radiographs are recommended. If the X-rays reveal metaphyseal-diaphyseal angle
>16° on AP radiographs and confirm the diagnosis of infantile Blount disease, he recommends anti-varus long leg bracing during ambulation for patients aged <=3 years with progressive deformity, clear radiographic evidence of infantile Blount disease, or lateral thrust with ambulation.
Illustration A shows pathologic metaphyseal beaking common in Blount's disease. There are no pathognomonic x-ray findings in physiological bowing as presented in this question.
Incorrect Answers:
Question 76
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 77
Arthrodesis of which of the following joints has the greatest cumulative effect on midfoot/hindfoot motion?
Explanation
REFERENCES: Astion DJ, Deland JT, Otis JC, et al: Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 1997;79:241-246.
Savory KM, Wülker N, Stukenborg C, et al: Biomechanics of the hindfoot joints in response to degenerative hindfoot arthrodeses. Clin Biomech 1998;13:62-70.
Question 78
A 48-year-old woman reports bilateral thigh pain that is limiting her function as a librarian. A radiograph and a bone scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, pp 956-957.
Wheeless’ Textbook of Orthopaedics: Acetabular Protrusio. www.wheelessonline.com/ortho/acetabular_protrusio
Question 79
- The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to
Explanation
Question 80
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Cracchiolo A: Surgical procedures of the lateral metatarsals, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1269-1283.
Question 81
Figures 10a through 10c show the radiographs of an 85-year-old man who underwent a revision total knee arthroplasty for loosening of the tibial component 6 months ago. He now reports a mildly uncomfortable mass on the anterior part of the knee joint. Examination reveals 95 degrees of motion and good quadriceps strength, and he can ambulate with minimal pain with a walker. History reveals chronic lymphocytic leukemia for which he is taking antineoplastic medication. Culture of the mass aspirate grew Candida albicans on two separate occasions. The patient and the family strongly prefer nonsurgical management. If long-term suppression is chosen as treatment, what advice should be given to the patient and family?
Explanation
REFERENCE: Mulvey TJ, Thornhill TS: Infected total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2,
pp 1857-1890.
Question 82
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.
Question 83
A 25-year-old athlete presents with symptoms attributed to injury to ligament D in Figure A. Which of the following symptoms and signs is characteristic of this injury? Review Topic
Explanation
PLRI can be diagnosed using the lateral pivot shift or posterolateral drawer. According to O’Driscoll, the elbow dislocates in 3 stages from lateral to medial (circle of Horii). Stage 1 involves disruption of the LUCL and partial/total disruption of the LCL complex (creating PLRI). Patients have pain with varus stress. Stage 2 includes disruption of the anterior capsule from incomplete elbow posterolateral dislocation. Stage 3 is divided into:
(a) Disruption of all soft tissues surrounding/ including the posterior MCL except for the anterior bundle. This bundle forms the pivot around which the elbow dislocates in a posterior direction by way of a posterolateral rotatory mechanism; and (b) complete disruption of the MCL.
O'Driscoll et al. describe PLRI diagnosed in 5 patients who had elbow dislocation using the posterolateral rotatory instability test, which they describe as being analogous to the test for lateral rotatory instability of the knee after ACL rupture. They believed the condition was laxity of the LUCL, which allowed transient rotatory subluxation of the ulnohumeral joint and secondary dislocation of the radiohumeral joint, without radio-ulnar joint dislocation. They recommended repair of the LUCL to eliminate PLRI.
Sanchez-Sotelo et al. retrospectively described 12 cases of direct repair and 33 ligamentous reconstructions for PLRI. 86% were satisfied with the procedure. Better results were obtained with patients with post-traumatic etiology, instability at presentation, and those with augmented reconstruction with tendon graft (compared with ligament repair alone).
Figure A shows structures on the lateral side of the elbow. The corresponding labels are seen in Illustration A. Illustration B shows the lateral pivot shift (also known as the posterolateral rotatory instability test).
Incorrect Answers:
Question 84
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include Review Topic
Explanation
(SBQ13PE.60) If a child develops dynamic supination after treatment of idiopathic clubfoot with Ponseti casting, at what age would it be appropriate to consider transfer of the tibialis anterior tendon to the lateral dorsum of the foot? Review Topic
In the first six months of life, immediately following failed cast treatment
12 months
4 years
12 years
15 years
Tibialis tendon transfer to the dorsum of the foot should be performed to address dynamic supination when the lateral cuneiform has ossified. This is typically after at least 2 years of age and usually not before age 3.
Question 85
Up to what time frame are the risks minimized in anterior revision disk replacement surgery?
Explanation
REFERENCE: Tortolani JP, McAfee PC, Saiedy S: Failures of lumbar disc replacement. Sem Spine Surg 2006;18:78-86.
Question 86
Which of the following patients is more likely to have an overall poorer outcome following a lower extremity amputation?
Explanation
Question 87
A 32-year-old male sustains a posterior wall acetabulum fracture as the result of a high-speed motor vehicle collision. Improved patient-reported outcomes after surgical treatment are associated with which of the following variables?

Explanation
The reference by Borrelli et al evaluated muscle strength and outcomes after acetabular surgery via an anterior approach. They report that hip extension strength was affected least(6%), whereas abduction, adduction, and flexion strength was affected to a greater degree. They note that hip muscle strength after operative treatment of a displaced acetabular fracture directly influences patient outcome.
The reference by Engsberg et al is a review of patients that underwent ORIF of acetabular fractures through anterior or posterior approaches. They report that maximizing hip muscle strength may improve gait, and improvement in hip muscle strength and gait is likely to improve functional outcome. Worsening functional outcomes were correlated with decreased gait kinematics and stride length.
Question 88
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 89
When counseling a patient with hypophosphatemic rickets, which of the following scenarios will always result in a child with the same disorder?
Explanation
REFERENCES: Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Greene WB, Kahler SG: Hypophosphatemic rickets: Still misdiagnosed and inadequately treated. South Med J 1985;78:1179-1184.
Question 90
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.
Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 91
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 92
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of
Explanation
REFERENCES: Lipscomb AB: Baseball pitching injuries in growing athletes. J Sports Med 1975;3:25-34.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
Barnett LS: Little league shoulder syndrome: Proximal humeral epiphysis in adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 93
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
REFERENCES: Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Richards DP, Burkhart SS: A biomechanical analysis of two biceps tenodesis fixation techniques. Arthroscopy 2005;21:861-866.
Question 94
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient? Review Topic
Explanation
Question 95
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4°F (37.4°C), and examination reveals that abduction of the left hip is limited to 30°. Laboratory studies show a WBC of 11,000/mm 3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of
Explanation
REFERENCE: Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 505-513.
Question 96
A 16-year-old boy who is a competitive basketball player (Figure 43)
Explanation

Question 97
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 176.
Question 98
A 35-year-old man sustained an injury to his lower extremity after falling 10 feet from a ladder; initial management was nonsurgical. He now reports chronic hindfoot and anterior ankle pain. Radiographs are shown in Figures 22a and 22b. Surgical reconstruction of this painful process should consist of
Explanation
REFERENCES: Carr JB, Hansen ST , Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Romash MM: Reconstructive osteotomy of the calcaneus with subtalar arthrodesis for malunited calcaneal fractures. Clin Orthop 1993;290:157-167.
Question 99
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?
Explanation
REFERENCES: Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96.
Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Tile M: Management, in Tile M: Fractures of the Pelvis and Acetabulum, ed 2. Philadelphia, PA, Williams and Wilkins, 1995, pp 108-134.
Question 100
A 52-year-old man has had back pain radiating to the left leg for the past 5 weeks. A radiograph, MRI scans, and biopsy specimens are shown in Figures 23a through 23f. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, vol 1, ch 8.
