Vascular Disorders of the Hand: Aneurysm, Thrombosis, and Embolism
Key Takeaway
Ischemic conditions of the hand, including aneurysms, thrombosis, and embolism of the radial, ulnar, and digital arteries, pose significant threats to digital viability. Management requires a thorough understanding of palmar arch hemodynamics, precise clinical evaluation using the Allen test, and advanced imaging. Surgical interventions range from simple arterial ligation to complex microsurgical reversed vein grafting, dictated by the integrity of collateral circulation and the severity of tissue ischemia.
Introduction to Vascular Disorders of the Hand
The vascular network of the hand is a highly specialized and redundant system designed to maintain perfusion across a wide range of functional demands and environmental conditions. Through the continuation of the radial artery into the hand as the deep palmar arch, and the ulnar artery as the superficial palmar arch, circulation to the hand is usually sufficient to allow the digits to remain viable despite significant localized disease or injury.
However, ischemic problems in the hand can and do result from aneurysms, thrombosis, or embolism within the radial, ulnar, or digital arteries. Arterial occlusive ischemia is frequently associated with direct blunt trauma, penetrating injuries, instrumentation of the vascular tree (e.g., arterial cannulation for monitoring or angiography), vascular access procedures, and systemic illnesses such as atherosclerosis and collagen vascular diseases.
This comprehensive guide details the pathophysiology, clinical evaluation, and advanced microsurgical management of aneurysms, thrombosis, and embolic events affecting the upper extremity, providing a rigorous framework for orthopedic surgeons and hand specialists.
Surgical Anatomy and Hemodynamics
A profound understanding of the palmar arches is mandatory before undertaking any vascular intervention in the hand. The arterial supply is characterized by significant anatomical variance, which directly dictates surgical decision-making.
- The Superficial Palmar Arch: Formed primarily by the continuation of the ulnar artery, it anastomoses with the superficial palmar branch of the radial artery. This arch is complete in approximately 80% of hands and incomplete in about 20%.
- The Deep Palmar Arch: Formed primarily by the continuation of the radial artery, it anastomoses with the deep palmar branch of the ulnar artery. The deep arch is highly reliable, being complete in approximately 98% of hands.
- Arterial Dominance: The radial artery usually provides the majority of the blood flow to three or more digits in 57% of hands. The ulnar artery provides dominant flow to three or more digits in almost 22% of hands. Codominance, where flow is provided equally from both arteries, occurs in the remaining 22%.
Clinical Pearl: Because of the high rate of anatomical variance, never assume the presence of a complete superficial arch. Preoperative and intraoperative assessment of collateral flow is the most critical step in preventing iatrogenic digital ischemia during vascular resection.
Clinical Evaluation and Diagnostics
Symptoms of hand ischemia include pain, sensory changes (paresthesias or anesthesia), skin discoloration (pallor, cyanosis, or rubor), ulceration, and frank necrosis. These symptoms are frequently aggravated by smoking, strenuous activity, and exposure to cold.
Physical findings may include:
* Digital pallor or cyanosis.
* Skin ulceration or necrosis distal to areas of occlusion.
* Sensory and motor deficits in the distribution of affected nerves (e.g., ulnar nerve compression in Guyon's canal due to an ulnar artery aneurysm).
* Coolness to palpation.
* Tenderness over an aneurysmal or thrombotic mass.
* A palpable thrill or pulsatile mass (indicative of an aneurysm or arteriovenous fistula).
The Allen Test
The Allen test is the fundamental physical examination maneuver for assessing the patency of the radial and ulnar arteries and the integrity of the palmar arches. Because distal vessel spasm can mimic structural occlusion (e.g., Raynaud's disease), the test must be performed meticulously.
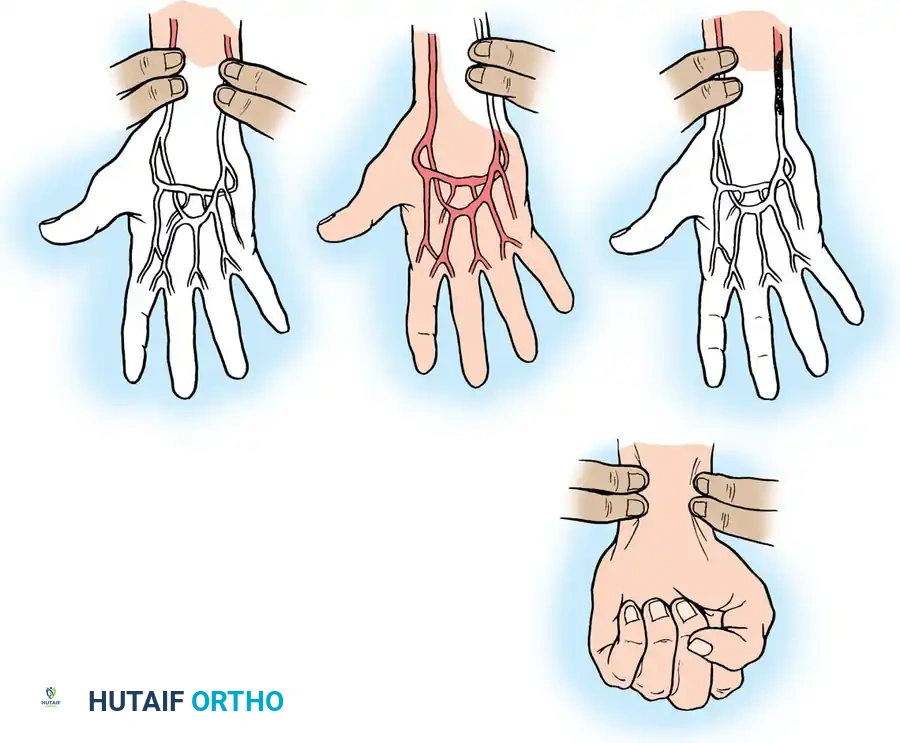
Fig. 67-1 Allen test for patency of radial and ulnar arteries. A, Patient elevates hand and makes a fist while the examiner occludes radial and ulnar arteries. B, Patient extends fingers, and blanching of the hand is seen. C, Radial artery alone is released, and the color of the hand returns to normal. D, In thrombosis of the ulnar artery, the test is positive (hand remains blanched) when this artery alone is released.
The same physiological principles apply to the digital arteries, where localized thrombosis can threaten a single digit.
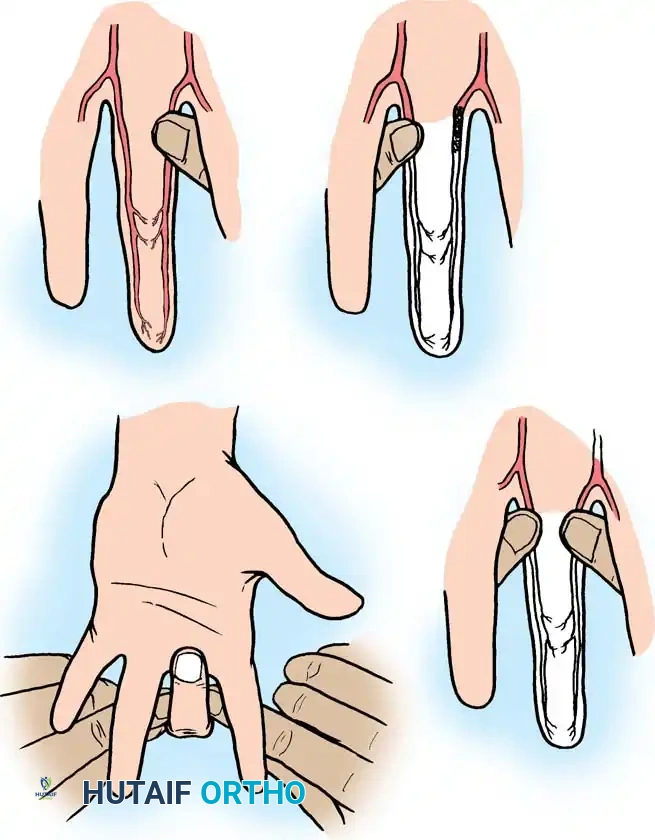
Fig. 67-2 Allen test applied to digital arteries. A, Examiner occludes both digital arteries, and patient flexes finger. B, Patient extends finger, and blanching of finger is seen. C, When either artery is patent, and it alone is released, color of finger returns to normal. D, When either artery is thrombosed, and it alone is released, finger remains blanched.
Advanced Diagnostic Modalities
When clinical examination suggests vascular compromise, advanced imaging and physiological testing are required to delineate the lesion:
1. Doppler Flow Assessment & Ultrasonography: Useful for initial non-invasive screening to detect flow velocity and structural anomalies.
2. Pulse Volume Recordings (PVR) & Segmental Arterial Measurement: Quantifies the severity of ischemia. A digital-brachial index (DBI) is calculated; a DBI < 0.7 indicates significant vascular compromise.
3. Magnetic Resonance Angiography (MRA): Provides excellent soft-tissue contrast and vascular mapping without ionizing radiation.
4. Contrast Angiography: The gold standard. It provides definitive information regarding the location and extent of the principal lesion, the status of the collateral circulation, and the peripheral "runoff."
Arterial Aneurysms of the Hand and Wrist
Although aneurysms may have atherosclerotic, mycotic, metabolic, or congenital origins, those seen in the hand and wrist are overwhelmingly the result of trauma.
* True Aneurysms: Involve all three layers of the arterial wall (intima, media, adventitia) and are typically caused by repetitive blunt trauma.
* False Aneurysms (Pseudoaneurysms): Result from penetrating trauma that breaches the arterial wall, leading to a contained hematoma that eventually forms a fibrous pseudocapsule.
Surgical Management of Aneurysms
The decision between simple aneurysm excision and excision followed by arterial reconstruction (reversed vein grafting) depends entirely on the anatomy of the palmar arch and the quality of distal circulation.
- Excision and Ligation: If the palmar arterial arch is complete and distal circulation is adequate (evidenced by pink distal skin color after tourniquet release, brisk backflow, or a DBI > 0.7), simple resection and ligation of the artery is sufficient. Reconstruction is unnecessary and introduces unwarranted surgical risk.
- Excision and Reconstruction: If the palmar arch is incomplete or distal circulation is inadequate, the artery must be reconstructed using a reversed segmental vein graft to restore perfusion and prevent digital loss.
Ulnar Artery Thrombosis (Hypothenar Hammer Syndrome)
Arterial thrombosis in the wrist, palm, and fingers is usually related to occupational or recreational trauma. The ulnar artery is the vessel most commonly affected by trauma-related thrombosis. This vulnerability is due to its superficial course over the hook of the hamate in Guyon's canal, where it lacks protective overlying muscle. Repeated forceful impacts—such as using the hypothenar eminence as a hammer—crush the artery against the carpal bones, leading to intimal damage, vasospasm, and eventual thrombosis.
Patients typically present with severe pain, cold intolerance, and occasionally loss of sensibility over the ulnar nerve distribution due to concomitant nerve compression or ischemia.
The Koman and Urbaniak Treatment Protocol
The management of ulnar artery thrombosis must be individualized. The protocol established by Koman and Urbaniak provides an evidence-based algorithm:
- Initial Diagnosis: Established via history, physical examination, and a positive Allen test.
- Confirmation: If the Allen test is positive, utilize thermography, temperature probes, Doppler studies, and PVR to confirm the diagnosis.
- Sympathetic Blockade: Administer a stellate ganglion or brachial plexus block. This relieves vasospasm in acute thrombosis that may be threatening digital survival.
- If symptoms are relieved: Proceed with conservative observation and lifestyle modification.
- If symptoms are NOT relieved: Proceed to arteriography.
- Arteriography and Intraarterial Medications: Arteriography establishes the extent of thrombosis and evaluates peripheral runoff. Concurrently, intraarterial vasodilators (e.g., reserpine, tolazoline, or papaverine) are administered.
- Surgical Intervention: Indicated if symptoms persist despite the above measures, or if digital survival is acutely in question.
Surgical Technique: Resection and Vein Grafting
When surgery is indicated, the primary goal is the complete removal of the thrombogenic source to eliminate sympathetically mediated vasospasm, followed by restoration of flow if collateral circulation is insufficient.
Surgical Warning: Contraindications to vein grafting include severe erythrocytosis, inadequate peripheral "runoff" on the arteriogram, and absolute patient refusal to discontinue smoking or modify their occupational environment. In such cases, graft failure is almost certain.
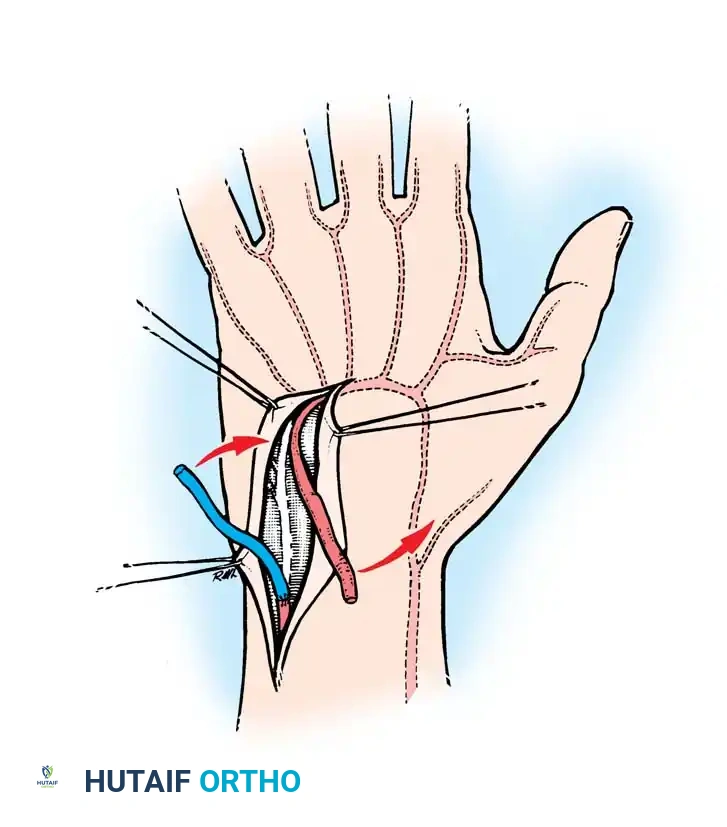
Fig. 67-3 Resection of thrombosed segment and replacement with reversed vein graft. The thrombosed segment is excised completely until healthy intima is visualized under the microscope. A reversed vein graft is then interposed to restore continuity.
Step-by-Step Microsurgical Reconstruction:
1. Exposure: Under tourniquet control and loupe magnification, a zig-zag incision is made over the hypothenar eminence, extending proximally across the wrist crease. The ulnar nerve is identified and carefully protected.
2. Resection: The thrombosed segment of the ulnar artery is mobilized. The artery is resected proximally and distally until normal, healthy, glistening intima is visualized under the operating microscope.
3. Assessment of Backflow: The proximal clamp is maintained, and the tourniquet is released.
* If backflow from the distal stump is brisk and pulsatile, and PVR of the ulnar digits normalizes, the vessel may simply be ligated.
* If backflow is poor, reconstruction is mandatory.
4. Graft Harvest: A suitable superficial vein (typically from the volar forearm) is harvested. The vein must be handled atraumatically to preserve its endothelial lining.
5. Reversal and Anastomosis: The vein graft is reversed to ensure that venous valves do not impede arterial flow. Using 8-0 or 9-0 non-absorbable monofilament suture, end-to-end anastomoses are performed under the microscope using standard microsurgical triangulation techniques.
6. Reperfusion: Clamps are released (distal first, then proximal). The anastomoses are inspected for leaks, and distal perfusion is confirmed.
In rare instances, the thrombosed mass may extend proximally into the forearm, but it rarely extends distally across the palmar arch. Complete resection relieves the spasm of the distal vessels, and circulation is subsequently maintained by the radial artery.
Arterial Embolism in the Upper Extremity
Arterial emboli in the upper extremity account for approximately 15% to 20% of all peripheral emboli. The etiology is predominantly systemic rather than local.
- Cardiac Origin (70%): The vast majority of emboli originate from the heart, secondary to atrial fibrillation, post-myocardial infarction mural thrombi, or valvular disease.
- Proximal Arterial Origin: The remainder typically originate from proximal aneurysms or atherosclerotic plaques in the subclavian or axillary arteries.
Clinical Presentation
Acute arterial embolism presents as a sudden, dramatic event characterized by the classic "6 Ps" of acute limb ischemia:
1. Pallor
2. Pain (sudden onset, severe ischemic pain)
3. Paresthesia
4. Paralysis (a late and ominous sign)
5. Pulselessness (loss of palpable or Doppler-sensed pulses)
6. Poikilothermia (cold sensation)
Management of Acute Embolism
Acute embolic ischemia is a surgical emergency. Time is tissue, and irreversible muscle and nerve necrosis can occur within 4 to 6 hours of complete occlusion.
- Medical Management: Immediate systemic anticoagulation with intravenous heparin is initiated to prevent propagation of the thrombus.
- Surgical Embolectomy: The gold standard treatment is a Fogarty catheter embolectomy. Under local or regional anesthesia, the artery is exposed (often at the brachial bifurcation or wrist, depending on the level of occlusion), a transverse arteriotomy is made, and a balloon-tipped Fogarty catheter is passed distally and proximally to extract the embolus.
- Thrombolytic Therapy: If the embolus significantly obstructs flow in distal vessels where a catheter cannot reach, intraarterial administration of thrombolytic agents (such as tissue plasminogen activator [tPA] or reteplase) can be highly effective. This is generally indicated if administered within 36 hours of the acute event and if the patient has no absolute contraindications to thrombolysis (e.g., recent surgery, intracranial hemorrhage).
- Long-term Management: Following successful revascularization, patients require long-term anticoagulation (e.g., Warfarin or direct oral anticoagulants) and a thorough cardiovascular workup to identify and treat the embolic source.
Postoperative Protocol and Rehabilitation
Following any vascular reconstruction or embolectomy in the hand, strict adherence to postoperative protocols is essential to ensure graft patency and maximize functional recovery.
- Environment and Positioning: The hand is kept elevated to minimize edema but should not be elevated above the level of the heart to avoid decreasing arterial perfusion pressure. The patient's room must be kept warm to prevent cold-induced vasospasm.
- Anticoagulation: Depending on the surgeon's preference and the caliber of the reconstructed vessel, postoperative regimens may include systemic heparinization, low-molecular-weight heparin, aspirin, or Dextran 40.
- Monitoring: Hourly monitoring of digital color, capillary refill, turgor, and temperature (using surface temperature probes) is mandatory for the first 24 to 48 hours. A drop in digital temperature of >2°C compared to adjacent digits is an early warning sign of graft thrombosis.
- Lifestyle Modification: Absolute cessation of smoking is non-negotiable. Nicotine is a potent vasoconstrictor and significantly increases the risk of graft failure. Biofeedback techniques and calcium channel blockers (e.g., nifedipine) may be utilized to manage persistent vasospastic symptoms.
- Therapy: Gentle, supervised active range of motion exercises are initiated early to prevent tendon adhesions, particularly if the surgical approach involved extensive dissection around the flexor tendons or Guyon's canal.
By combining a rigorous understanding of vascular anatomy with precise microsurgical technique and strict postoperative care, the orthopedic surgeon can successfully navigate the complexities of hand vascular disorders, preserving both the viability and function of the upper extremity.
You Might Also Like
