
The paradigm of meniscal surgery has undergone a profound evolution over the past several decades, shifting unequivocally from the historically ubiquitous total meniscectomy toward a philosophy of meticulous knee preservation. Today, arthroscopic meniscal repair stands as a cornerstone of joint preservation surgery. This procedure is not merely a technical exercise in tissue approximation; it is a fundamental restoration of knee biomechanics designed to halt the inexorable cascade of degenerative changes that inevitably follow the loss of meniscal tissue. Our overarching goal as orthopedic surgeons is to preserve, optimize, and biologically augment meniscal function, thereby ensuring the long-term survivorship of the articular cartilage and the native joint.
Comprehensive Introduction and Patho-Epidemiology
The menisci are indispensable structures within the knee, and their pathology represents one of the most frequently encountered clinical scenarios in orthopedic practice. Understanding the epidemiological landscape and the underlying pathogenesis of meniscal tears is critical for appropriate patient selection and surgical decision-making. A meniscus tear represents a mechanical disruption of the highly organized fibrocartilaginous network, compromising its ability to manage complex multiaxial loads.
Pathogenesis and Etiology
Acute meniscal tears are predominantly observed in the younger, highly active, and athletic patient populations. These injuries typically result from a violent combination of axial compression and rotational forces applied to the knee joint, frequently occurring as the knee transitions dynamically from a flexed, weight-bearing position into sudden extension or rotation. Consider the classic pivot-shift mechanism in pivoting sports such as soccer, basketball, or skiing. The sheer forces generated during these maneuvers can exceed the tensile limits of the meniscal collagen framework, leading to sharp, distinct, and often displaceable tears. These acute traumatic events frequently occur in tandem with ligamentous disruptions, most notably the anterior cruciate ligament (ACL).

Conversely, degenerative tears present a distinctly different clinical and pathophysiological entity. These are chronic in nature, exponentially more common in the middle-aged and elderly demographics, and typically manifest as complex, multi-planar, or horizontal cleavage tears. The etiology here is insidious, rooted in repetitive microtrauma over decades compounded by the natural senescence of the meniscal fibrocartilage. As the meniscus ages, there is a quantifiable decrease in cellularity and a shift in the extracellular matrix composition, leading to reduced viscoelasticity and an increased propensity for mechanical failure under normal physiological loads.
Given the inherent complexity, chronicity, and frequently poor tissue quality associated with degenerative tears, they have historically been considered irreparable. However, the overarching goal of any modern meniscal intervention remains the preservation of function. While partial meniscectomy may be necessary to alleviate acute mechanical symptoms in severely macerated degenerative tissue, the imperative to repair must always be at the forefront of the surgeon's mind when encountering acute, traumatic tears in viable tissue. The failure to do so guarantees a predictable progression toward premature osteoarthritis.
The Imperative for Preservation and Natural History
The seminal work by Fairbank in 1948, and later biomechanical studies by Walker and Erkman in the 1970s, unequivocally established the critical load-bearing function of the menisci. The lateral meniscus bears approximately 70% of the load in the lateral compartment, while the medial meniscus shares roughly 50% of the load with the articulating surfaces of the medial compartment. The menisci achieve this through their unique capability to convert axial compressive loads into circumferential "hoop stresses," effectively dissipating force across a maximized surface area.

The biomechanical consequences of meniscectomy are well-documented, reproducible, and catastrophic to the joint. A partial meniscectomy of just 15% to 30% of the meniscus can decrease the femoral-tibial contact area by over 10%, subsequently increasing peak local contact stresses (PLCS) by up to 65%. A total meniscectomy is biomechanically devastating, decreasing contact areas by 75% and driving PLCS up by an astonishing 235%. These exponentially elevated stresses overload the underlying articular cartilage, leading to chondrocyte apoptosis, matrix degradation, and accelerated osteoarthritis.
Fortunately, contemporary literature demonstrates that successful meniscal repair restores peak local contact stresses and contact areas to near-normal physiological levels. By achieving stable fixation and promoting biological healing, we can dramatically alter the natural history of the injured knee, decreasing chondral wear and delaying or preventing the onset of degenerative joint disease. This overwhelming biomechanical evidence forms the absolute rationale for prioritizing meniscal repair whenever technically and biologically feasible.
Detailed Surgical Anatomy and Biomechanics
Before a surgeon introduces a trocar into the knee, a profound, three-dimensional understanding of meniscal anatomy, ultrastructure, and regional neurovascular relationships is non-negotiable. The menisci are not simply inert spacers; they are dynamic, living tissues with complex architectural and biological properties.
Meniscal Ultrastructure and Function
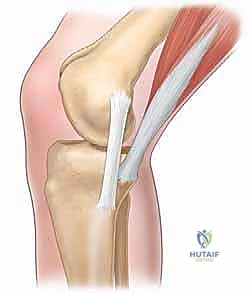
Macroscopically, the menisci are crescent-shaped, fibrocartilaginous discs that are triangular in cross-section. Microscopically, their composition is a marvel of biological engineering. They are composed primarily of water (up to 72% of their total weight) and an intricate extracellular matrix. The dry weight is dominated by collagen, with Type I collagen constituting roughly 90% of the matrix, providing the meniscus with its extraordinary tensile strength. The remaining matrix comprises minor collagens (Types II, III, V, and VI), proteoglycans (predominantly aggrecan), non-collagenous proteins, and specialized fibrochondrocytes.

The collagen fibers are highly organized to manage specific mechanical loads. In the peripheral third of the meniscus, the thick Type I collagen bundles are arranged strictly in a circumferential pattern. This architecture is specifically designed to resist the "hoop stresses" generated during axial loading. In the inner two-thirds, the collagen organization becomes more complex, featuring a combination of radial and circumferential fibers, allowing the thinner, central portion of the meniscus to resist shear forces and provide a smooth gliding surface for the femoral condyles.
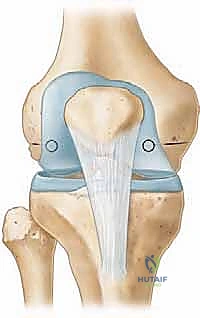
Functionally, the menisci serve multiple critical roles. They deepen the articular surface of the relatively flat tibial plateau, vastly enhancing congruity with the spherical femoral condyles. They act as dynamic joint stabilizers, compensating for gross incongruity, particularly in the ACL-deficient knee where the posterior horn of the medial meniscus acts as the primary secondary restraint to anterior tibial translation. Furthermore, they facilitate joint lubrication, maintain synovial fluid distribution, and assist in providing vital nutrition to the avascular articular cartilage.
Medial and Lateral Meniscal Anatomy
The medial meniscus is distinctly C-shaped, covering approximately 60% to 64% of the medial tibial plateau. Its width varies significantly, being narrower anteriorly and widest at its posterior horn. Crucially, the medial meniscus is firmly anchored to the joint capsule and the deep fibers of the medial collateral ligament (MCL) via the meniscotibial (coronary) ligaments. This rigid attachment limits its excursion during knee flexion, rendering it highly susceptible to shear and rotational forces. Consequently, medial meniscus tears frequently occur in conjunction with ACL injuries, classically presenting as the "terrible triad" (ACL, MCL, and medial meniscus tear).

In contrast, the lateral meniscus is more circular, covering a much larger portion—up to 84%—of the lateral tibial plateau. It maintains a relatively uniform width of 12 to 13 mm throughout its circumference. The lateral meniscus lacks a firm capsular attachment posterolaterally due to the presence of the popliteal hiatus, through which the popliteus tendon passes. This anatomic feature affords the lateral meniscus significantly greater mobility (up to 11 mm of anteroposterior excursion compared to the medial meniscus's 5 mm), offering it a degree of protection against rotational trauma.
However, the lateral meniscus is not immune to injury, particularly in acute ACL ruptures where lateral compartment bone bruising and associated lateral meniscal tears are highly prevalent. The surgeon must also be intimately familiar with the meniscofemoral ligaments—the ligament of Humphry (anterior to the posterior cruciate ligament) and the ligament of Wrisberg (posterior to the PCL)—which connect the posterior horn of the lateral meniscus to the medial femoral condyle. These structures are critical for lateral meniscal stability and must not be misidentified as tears during arthroscopy.
Vascularity and Neurovascular Danger Zones
The vascular supply to the menisci dictates their healing potential and forms the basis for our surgical indications. The blood supply originates from the perimeniscal capillary plexus, derived from the superior and inferior medial and lateral geniculate arteries. This plexus penetrates the peripheral capsular attachment of the meniscus. At birth, the entire meniscus is vascularized, but by adulthood, this vascularity recedes dramatically.

This recession creates three distinct zones: the "Red-Red" zone (the peripheral 3 mm, rich in blood supply and possessing excellent healing potential), the "Red-White" zone (the middle 3-5 mm, with diminishing vascularity and moderate healing potential), and the "White-White" zone (the central avascular region, relying entirely on synovial fluid diffusion for nutrition, with virtually zero intrinsic healing capacity). Surgical repair is primarily directed at tears within the Red-Red and Red-White zones.
Equally critical is the regional neurovascular anatomy, which represents the "danger zones" during inside-out and outside-in repair techniques. On the medial side, the saphenous nerve and its infrapatellar branch, along with the great saphenous vein, run superficially in the posteromedial aspect of the knee. Deep to these lie the medial geniculate vessels. When creating a posteromedial safety incision for inside-out suture retrieval, meticulous blunt dissection down to the capsule is mandatory to protect these structures. On the lateral side, the common peroneal nerve is the paramount structure at risk. It courses posteriorly to the biceps femoris tendon and wraps around the fibular neck. Posterolateral safety incisions must remain strictly anterior to the biceps tendon and superior to the joint line to avoid catastrophic denervation of the anterior and lateral compartments of the leg.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic meniscal repair versus partial meniscectomy requires a nuanced synthesis of patient-specific factors, tear morphology, and concomitant joint pathology. Not all tears can be repaired, and not all patients are appropriate candidates for the rigorous postoperative rehabilitation required following a repair.
Patient Selection and Tear Morphology
Ideal candidates for meniscal repair are young, active patients with acute, traumatic tears located in the vascularized peripheral zones (Red-Red or Red-White). The chronicity of the tear plays a significant role; acute tears (less than 6-8 weeks old) exhibit a more robust healing response compared to chronic tears, which often feature rounded, avascular edges and degraded tissue quality. However, chronicity alone is not an absolute contraindication if the tissue quality remains robust upon arthroscopic probing.
Tear morphology is the most critical technical determinant of repairability. Longitudinal (vertical) tears, which run parallel to the circumferential collagen fibers, are highly amenable to repair as sutures can effectively compress the tear edges without pulling through the tissue. Bucket-handle tears, which are essentially displaced longitudinal tears, are classic indications for repair. Radial tears, which perpendicularly transect the hoop fibers, are biomechanically devastating and technically challenging to repair, often requiring complex cross-stitching or novel tie-grip techniques to prevent suture pull-through. Horizontal cleavage tears, traditionally viewed as degenerative and treated with meniscectomy, are increasingly being repaired in younger patients using circumferential compression techniques, provided the superior and inferior leaflets maintain structural integrity.
Concomitant Pathology and Biological Augmentation
The status of the knee ligaments, particularly the ACL, profoundly influences meniscal healing. It is a well-established clinical axiom that meniscal repairs performed concurrently with ACL reconstruction demonstrate significantly higher healing rates compared to isolated meniscal repairs. This phenomenon is attributed to the "biological boost" provided by the hemarthrosis, bone marrow elements, and growth factors released during the creation of the femoral and tibial tunnels for the ACL graft.
For isolated meniscal repairs, surgeons increasingly employ biological augmentation techniques to simulate this healing environment. Techniques such as trephination (creating vascular channels from the peripheral blood supply into the tear), rasping the synovium and perimeniscal capsule to stimulate a hyperemic response, and marrow venting (microfracture of the intercondylar notch) are routinely utilized. More advanced biological adjuncts, including the application of platelet-rich plasma (PRP) or exogenous fibrin clots directly into the tear site, are also employed to optimize the biochemical milieu for fibrochondrocyte proliferation and matrix synthesis.
Indications and Contraindications Table
| Parameter | Indications for Meniscal Repair | Contraindications for Meniscal Repair |
|---|---|---|
| Patient Factors | Young age (< 40 years ideally, but biological age is key), highly active, compliant with complex rehab. | Advanced age with low functional demands, inability to comply with non-weight-bearing protocols. |
| Tear Location | Peripheral (Red-Red zone), Mid-substance (Red-White zone). | Central (White-White zone) without biological augmentation, Root avulsions in advanced OA. |
| Tear Morphology | Longitudinal vertical tears, reducible bucket-handle tears, acute radial tears in young patients. | Complex multi-planar degenerative tears, severely macerated tissue, extensive flap tears. |
| Chronicity | Acute tears (< 8 weeks), symptomatic chronic tears with excellent tissue quality. | Chronic tears with severe plastic deformation that cannot be anatomically reduced. |
| Joint Status | Stable knee, or unstable knee undergoing concurrent ligamentous reconstruction. | Uncorrected ligamentous instability, advanced osteoarthritis (Kellgren-Lawrence Grade III/IV). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful intraoperative execution. The diagnostic journey begins with a comprehensive history and a systematic physical examination, culminating in advanced imaging to define the precise pathoanatomy.
Clinical Evaluation and Advanced Imaging
The patient history often reveals a specific mechanism of injury, typically involving a twisting motion on a weight-bearing, flexed knee. Mechanical symptoms such as catching, locking, or the inability to achieve full extension are hallmark signs of a displaced meniscal fragment, such as a bucket-handle tear. On physical examination, joint line tenderness is the most sensitive clinical indicator. Provocative maneuvers, including the McMurray test, Apley compression test, and Thessaly test, are utilized to reproduce mechanical impingement and confirm the diagnosis. Crucially, the knee must be rigorously assessed for concomitant ligamentous laxity, particularly utilizing the Lachman and pivot-shift tests for the ACL.

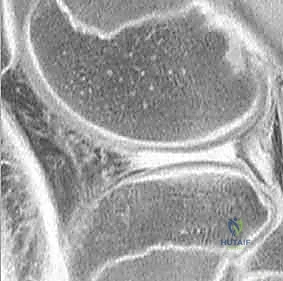
While a clinical diagnosis is often highly accurate, Magnetic Resonance Imaging (MRI) is the gold standard for preoperative templating. MRI provides invaluable details regarding tear location, length, depth, and morphology. Tears are classified on MRI into three grades: Grade I (globular increased signal), Grade II (linear increased signal not extending to an articular surface), and Grade III (linear signal extending to the superior or inferior articular surface). Only Grade III signals represent true, clinically relevant meniscal tears. The surgeon must meticulously review the sagittal, coronal, and axial sequences to plan the optimal repair strategy, anticipate the need for specific instrumentation (e.g., curved vs. straight delivery cannulas), and identify associated pathology such as chondral defects or subchondral bone bruising.
Patient Positioning and Operating Room Setup
Proper patient positioning is critical to achieving the necessary joint access and visualization required for complex meniscal repairs. The procedure is typically performed under general or regional anesthesia. A well-padded high-thigh tourniquet is applied but often left uninflated unless visualization becomes compromised, as the bleeding from the capsule and synovium provides valuable biological factors for healing.
The patient is positioned supine on the operating table. Two primary setups are utilized: the leg holder technique and the lateral post technique. The leg holder firmly secures the proximal thigh, allowing the surgeon to apply varus or valgus stress dynamically while flexing and extending the knee. This is particularly advantageous for opening the posterior compartments. Alternatively, a lateral post allows the leg to hang freely over the edge of the bed, which is excellent for hyperflexion maneuvers and figure-of-four positioning to access the lateral compartment. Regardless of the setup, the contralateral leg must be carefully padded and protected to prevent neuropraxia or compartment syndrome.
Step-by-Step Surgical Approach and Fixation Technique
The execution of an arthroscopic meniscal repair demands technical precision, a deep understanding of spatial relationships within the joint, and mastery of multiple fixation techniques. The surgeon must be prepared to utilize a combination of inside-out, outside-in, and all-inside techniques depending on the specific location and morphology of the tear.
Diagnostic Arthroscopy and Biological Preparation
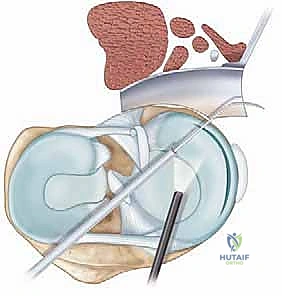
The procedure commences with a standard diagnostic arthroscopy utilizing standard anterolateral and anteromedial portals. A systematic evaluation of the patellofemoral joint, medial and lateral gutters, medial and lateral compartments, and the intercondylar notch is performed. Once the meniscal tear is identified, it is rigorously probed to assess its length, depth, stability, and tissue quality. Displaced fragments, such as bucket-handle tears, must be anatomically reduced to ensure they can be repaired without tension.

Before any sutures are passed, meticulous biological preparation of the tear site is mandatory. This is arguably the most critical step in ensuring a successful outcome. A meniscal rasp or motorized shaver is used to aggressively debride the fibrotic edges of the tear, exposing healthy, bleeding tissue. The perimeniscal synovium and capsule adjacent to the tear are also rasped to stimulate a profound hyperemic response. In cases of chronic or avascular tears, trephination may be performed using an 18-gauge spinal needle to create vascular access channels from the periphery into the tear site. If the repair is performed in isolation (without concurrent ACL reconstruction), marrow venting via microfracture of the intercondylar notch is strongly recommended to release mesenchymal stem cells and growth factors into the joint fluid.
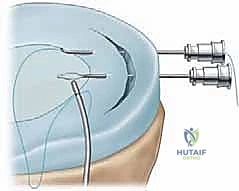
The Inside-Out Technique: The Gold Standard
The inside-out technique remains the gold standard for meniscal repair, particularly for extensive longitudinal tears involving the middle and posterior thirds of the meniscus. It offers unparalleled biomechanical strength and the versatility to place sutures precisely where needed. This technique requires the use of long, flexible needles swaged to non-absorbable or slowly absorbable sutures (e.g., 2-0 FiberWire or PDS), delivered through zone-specific cannulas.

Crucially, the inside-out technique mandates the creation of a posterior safety incision to protect neurovascular structures and retrieve the needles. For a medial repair, a posteromedial incision is made posterior to the medial collateral ligament. Blunt dissection is carried down to the posteromedial capsule, carefully retracting the saphenous nerve and medial head of the gastrocnemius posteriorly. A retractor (such as a Henning retractor or a simple tablespoon) is placed anterior to the gastrocnemius to protect the popliteal vessels and catch the exiting needles.
Under direct arthroscopic visualization, the delivery cannula is advanced to the tear. The needles are passed sequentially across the tear, capturing the superior and inferior leaflets, and driven through the capsule. The needles are retrieved through the safety incision. Sutures are typically placed in a vertical or horizontal mattress configuration, spaced approximately 5 mm apart. Once all sutures are passed, they are tied directly over the capsule through the safety incision while the knee is held in extension to ensure anatomical tensioning.

The Outside-In and All-Inside Techniques
The outside-in technique is primarily utilized for tears involving the anterior horn and the anterior portion of the middle third of the meniscus. In this technique, an 18-gauge spinal needle is passed from the outside of the knee, through the capsule, and across the meniscal tear into the joint space. A looped shuttle suture (e.g., a PDS loop) is passed through the needle. A second needle is passed adjacently, and a free suture is fed through it and retrieved via the shuttle loop, creating a mattress configuration. The knot is tied subcutaneously over the joint capsule. This technique is highly effective for anterior tears where inside-out cannulas cannot be easily maneuvered.
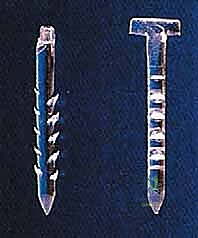
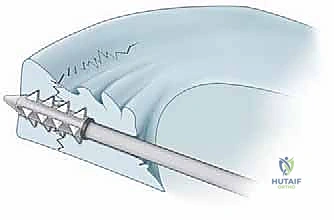
The all-inside technique has revolutionized meniscal repair, particularly for posterior horn tears, by eliminating the need for posterior safety incisions. Modern all-inside devices utilize pre-tied sliding knots and low-profile anchors (e.g., PEEK or suture-based anchors). The device is introduced through standard anterior portals. The needle penetrates the meniscus and capsule, deploying the first anchor. The device is withdrawn slightly, repositioned, and fired again to deploy the second anchor, spanning the tear. The pre-tied suture is then tensioned, compressing the tear edges, and cut flush with the meniscus.

While technically elegant and time-saving, all-inside devices must be used judiciously. The surgeon must ensure the anchors are deployed deep into the capsule to avoid intra-articular prominence, which can cause severe chondral damage. Furthermore, care must be taken not to over-tension the construct, which can cause the suture to cut through the meniscal tissue ("cheese-wiring").


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, meniscal repair is not without risks. Complications can range from minor postoperative stiffness to catastrophic neurovascular injuries or complete failure of the repair. A thorough understanding of these potential pitfalls is essential for prompt recognition and appropriate salvage management.
Iatrogenic Neurovascular and Chondral Injuries
The most feared complications during meniscal repair are iatrogenic injuries to the regional neurovascular structures. During inside-out medial repairs, the saphenous nerve and its infrapatellar branch are at highest risk. Injury can result in painful neuromas or sensory deficits along the medial aspect of the leg. During lateral inside-out or outside-in repairs, the common peroneal nerve is highly vulnerable. A transection or severe traction injury to the peroneal nerve results in a devastating foot drop. Meticulous adherence to anatomical landmarks and the proper use of posterior safety incisions and retractors are the only ways to mitigate these risks.
Chondral injury is another significant concern, primarily associated with the use of all-inside devices. If the anchors are not deployed sufficiently deep into the capsule, or if they migrate postoperatively, the hard plastic or PEEK components can act as an abrasive body against the femoral condyle, leading to rapid and severe iatrogenic chondromalacia. Additionally, aggressive maneuvering of arthroscopic instruments within a tight joint space can cause scuffing of the articular cartilage.

Repair Failure and Arthrofibrosis
The most common complication following meniscal repair is failure of the tissue to heal, leading to a recurrent or persistent tear. Clinical failure rates vary widely in the literature, ranging from 10% to 25%, depending on the tear type, location, chronicity, and concurrent ACL status. Failure typically presents as recurrent mechanical symptoms, joint line pain, and recurrent effusions. Diagnosis is confirmed via MRI or second-look arthroscopy. Salvage management for a failed repair typically involves a partial meniscectomy, although a revision repair may be attempted in highly selected, young patients with excellent remaining tissue quality.

Arthrofibrosis, or severe postoperative stiffness, is a risk whenever the knee joint is operated upon and subsequently immobilized. While early motion is generally encouraged, excessive protection of the repair can lead to capsular contracture and loss of motion, particularly extension. Management involves aggressive physical therapy, judicious use of oral corticosteroids, and, in refractory cases, arthroscopic lysis of adhesions and manipulation under anesthesia.
Complications and Incidence Table
| Com
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding meniscal-repair