Meniscal Repair Explained: Anatomy, Function, & Treatment

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Meniscal Repair Explained: Anatomy, Function, & Treatment. Meniscal repair meniscal repair addresses a meniscus tear, a mechanical disruption of the medial or lateral meniscus. The goals of meniscal repair are to preserve and optimize meniscus function and to restore joint biomechanics. This procedure is crucial for maintaining the knee's natural shock absorption and stabilization, crucial for overall joint health.
Comprehensive Introduction and Patho-Epidemiology
A meniscal tear represents a profound mechanical disruption of the gross fibrocartilaginous structure of the medial meniscus, lateral meniscus, or both. Historically viewed as an expendable vestige of human evolution, the meniscus is now universally recognized by orthopedic surgeons as an indispensable component of knee biomechanics. The overarching and primary goals of any meniscus repair are to meticulously preserve and optimize meniscal function, restore native joint kinematics, and ultimately prevent the rapid onset of degenerative joint disease. As our understanding of knee joint preservation has evolved, the paradigm has shifted dramatically from routine total meniscectomy to aggressive meniscal preservation whenever technically feasible and biologically appropriate.
The pathogenesis of meniscal lesions is broadly categorized into acute traumatic events and chronic degenerative processes, each presenting distinct clinical and histological profiles. Acute tears typically occur in younger, highly active patient populations and are the direct result of massive compressive forces combined with rotational injury to the knee joint. This highly specific mechanism of injury most frequently occurs as the loaded knee transitions forcefully from a flexed position into terminal extension, trapping the meniscus between the femoral condyle and the tibial plateau. These acute tears often exhibit discrete, identifiable patterns such as longitudinal or radial disruptions and possess a higher intrinsic healing potential due to the relatively healthy state of the surrounding fibrocartilage matrix.

Conversely, degenerative meniscal tears are inherently chronic in nature, predominantly afflicting older patient demographics. These lesions are characterized by a progressive deterioration of the collagenous ultrastructure, leading to complex, multidirectional tear patterns that are frequently deemed irreparable. The fibrocartilage in degenerative tears often exhibits myxoid degeneration, decreased cellularity, and a compromised extracellular matrix. Attempting to repair a severely degenerated meniscus is generally futile, as the tissue lacks the structural integrity to hold sutures and the biological capacity to mount an effective healing response, thereby making partial meniscectomy the more appropriate intervention in symptomatic cases that fail conservative management.

Epidemiologically, the incidence and location of meniscal tears are heavily influenced by the stability of the knee joint. Medial meniscus tears most frequently occur in the setting of a stable knee or, notably, within a chronic anterior cruciate ligament (ACL)-deficient knee where the posterior horn of the medial meniscus acts as a secondary restraint to anterior tibial translation, subjecting it to repetitive microtrauma. Lateral meniscal tears, however, are more commonly associated with acute ACL ruptures in younger patients. The classic "terrible triad" injury—comprising simultaneous tears of the lateral meniscus, the ACL, and the medial collateral ligament (MCL)—is a catastrophic derangement typically sustained from a severe hyperextension force coupled with a violent valgus stress, classically observed during a "clipping" injury in collision sports.

Detailed Surgical Anatomy and Biomechanics
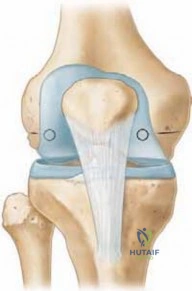
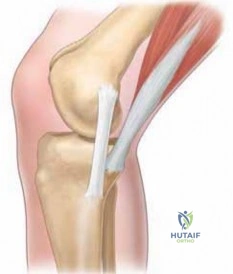
The gross anatomy of the menisci reveals highly specialized, crescent-shaped structures that are distinctly triangular in cross-section, allowing them to perfectly contour to the convex femoral condyles and the relatively flat tibial plateaus. The medial meniscus is distinctly C-shaped and covers approximately 64% of the medial tibial plateau. Its width demonstrates significant variability from the anterior horn to the posterior horn, averaging roughly 10 mm overall, with the posterior horn being substantially wider and more firmly anchored, which contributes to its higher incidence of tearing in ACL-deficient knees. In contrast, the lateral meniscus is far more circular in its morphology, covering a significantly larger portion—approximately 84%—of the lateral tibial plateau, with a more uniform average width of 12 to 13 mm.

Microscopically, the menisci are complex fibrocartilaginous tissues composed predominantly of water and a highly organized extracellular matrix. The dry weight of the meniscus is dominated by collagen, with Type I collagen constituting 90% of the structural framework, supplemented by trace amounts of Types II, III, V, and VI. The spatial orientation of these collagen fibers is critical to meniscal biomechanics: the peripheral third is defined by a dense arrangement of circumferential fibers designed to dissipate hoop stresses, whereas the inner two-thirds feature a sophisticated interweaving of both radial and circumferential fibers. This matrix is sparsely populated by specialized fibrochondrocytes responsible for synthesizing and maintaining the extracellular environment.
The vascular anatomy of the meniscus is the single most critical determinant of its healing capacity and dictates surgical decision-making. Blood supply is derived exclusively from the perimeniscal capillary plexus, which is fed by the medial and lateral inferior and superior geniculate arteries. This plexus penetrates the peripheral meniscal rim, but its arborization decreases precipitously as it progresses centrally toward the free edge. This stark vascular gradient creates three distinct anatomical zones: the highly vascularized red-red zone at the periphery, the transitional red-white zone in the middle third, and the avascular white-white zone at the inner margin. Furthermore, the peripheral meniscus is heavily innervated with free nerve endings and corpuscular mechanoreceptors, which provide essential nociceptive feedback and proprioceptive data to the knee joint.

Biomechanically, the menisci are indispensable for joint preservation. They function to deepen the articular surface of the tibial plateau, providing critical shock absorption and compensating for the gross osseous incongruity between the articulating surfaces. Walker and Erkman (1975) demonstrated that under loads up to 150 kg, the lateral meniscus bears the vast majority of the weight-bearing load in the lateral compartment, whereas the medial meniscus shares approximately 50% of the load with the articular cartilage. The deleterious effects of meniscectomy are profound: partial meniscectomy decreases femoral-tibial contact areas by about 10% while increasing peak local contact stresses (PLCS) by 65%. Catastrophically, total meniscectomy decreases contact areas by 75% and skyrockets PLCS by an astonishing 235%, virtually guaranteeing the rapid onset of osteoarthritis, whereas successful meniscal repair normalizes both PLCS and contact areas.

Exhaustive Indications and Contraindications
The decision to proceed with meniscal repair versus partial meniscectomy requires a highly nuanced, multifactorial analysis by the operating surgeon. The primary indication for meniscal repair is a symptomatic, unstable tear located in the vascularized red-red or red-white zones in a patient who is compliant and possesses a reasonable healing capacity. The potential long-term benefit of repairing the meniscus is profound chondroprotection; therefore, every effort must be made to preserve the meniscosynovial junction, where the circumferential collagen fibers generate the predominant amount of essential "hoop stresses." The surgeon must rigorously evaluate the tear location, morphological pattern, chronicity, and the presence of associated ligamentous pathology before committing to a repair strategy.
Tear patterns play a pivotal role in determining repairability. Acute, longitudinal tears greater than 1 cm in length that displace into the joint (such as classic bucket-handle tears) are prime candidates for repair, particularly when they occur within the peripheral vascular zones. Conversely, radial tears that transect the circumferential fibers disrupt the meniscus's ability to dissipate hoop stresses; while peripheral radial tears can occasionally be repaired, deep radial tears extending into the white-white zone are generally resected. Horizontal cleavage tears and complex, multi-planar degenerative tears in older patients typically lack the structural integrity required for suture fixation and are universally considered contraindications for repair, necessitating judicious partial meniscectomy.
Patient-specific factors are equally critical when weighing indications and contraindications. The surgeon must thoroughly discuss the patient's age, functional demands, athletic goals, and willingness to adhere to a strict, prolonged postoperative rehabilitation protocol. A highly elite athlete may sometimes opt for a partial meniscectomy over a repair to facilitate an accelerated return to competitive sport, despite the known long-term risks of early-onset osteoarthritis. This represents a complex ethical and clinical conversation regarding short-term functional gains versus long-term joint preservation. Furthermore, a stable longitudinal tear in the extreme periphery measuring less than 10 mm is often left in situ, as it possesses a high intrinsic capacity to heal spontaneously without surgical intervention.

| Variable | Indications for Meniscal Repair | Contraindications for Meniscal Repair |
|---|---|---|
| Tear Location | Red-red zone, Red-white zone | White-white zone (avascular inner third) |
| Tear Pattern | Longitudinal, Bucket-handle, peripheral capsular | Complex, degenerative, deep radial, horizontal cleavage |
| Tissue Quality | Excellent, acute, robust fibrocartilage | Poor, myxoid degeneration, chronic fraying |
| Patient Age/Profile | Younger, active, compliant with rehab | Older, sedentary, non-compliant |
| Associated Injuries | Concomitant ACL reconstruction (enhances healing) | Advanced unicompartmental osteoarthritis |
| Tear Stability | Unstable (displaces >7mm, able to "roll") | Stable, asymptomatic, <10mm peripheral tear |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with an exhaustive patient history and a meticulous physical examination. The history must elucidate the precise location of pain—specifically noting joint line tenderness—the mechanism of recent traumas, prior surgical interventions, and the presence of mechanical symptoms such as locking, catching, or giving way. A complete examination of the knee is mandatory to rule out concomitant ligamentous pathology. This includes assessing the ACL and PCL via the Lachman test, anterior/posterior drawer, and pivot shift tests. The posterolateral corner must be evaluated for asymmetry using the dial test at 30 and 90 degrees of flexion, while the collateral ligaments require varus and valgus stress testing in both full extension and 30 degrees of flexion.

Specific meniscal provocation tests are heavily relied upon to confirm the diagnosis clinically. The McMurray test is performed by applying varus and valgus stress coupled with internal and external rotation during knee flexion and extension; a palpable clunk or reproducible pain indicates a positive result. The Apley grind test differentiates between ligamentous and meniscal pathology by applying axial compression and rotation to the prone patient's knee. The Childress test (duck walk) will elicit pain or mechanical blocking in the presence of a significant posterior horn tear. Furthermore, the Merkel sign demonstrates that pain with internal rotation of the tibia is consistent with a medial meniscus tear, whereas pain with external rotation implicates the lateral meniscus.

Imaging modalities are critical for preoperative templating and confirming the clinical diagnosis. Standard plain radiographs—including a 45-degree posteroanterior flexion weight-bearing view, a true lateral, a notch view, and a patella skyline view—are required to evaluate for underlying osteoarthritis, chondrocalcinosis, osteochondritis dissecans (OCD) lesions, or a Segond fracture indicative of an ACL tear. Magnetic Resonance Imaging (MRI) remains the gold standard for non-invasive evaluation, boasting a sensitivity of 96% and a specificity of 97%. MRI pathology is classified into three grades, with Grade 3 representing a linear area of increased signal unequivocally extending to the articular surface on two consecutive images, confirming a true tear.

Advanced MRI findings, such as the "double PCL" sign, are pathognomonic for a displaced medial bucket-handle tear resting in the intercondylar notch. A discoid meniscus, more commonly lateral, appears as a rectangular, block-like structure on multiple consecutive sagittal slices rather than the normal wedge shape. Preoperative planning also involves coordinating with the anesthesia team; while general anesthesia is common, regional anesthesia or a laryngeal mask airway (LMA) combined with local surgeon-administered anesthetic is often preferred. The patient is typically positioned supine on the operating table with a lateral post or leg holder deployed to allow for the application of valgus and varus forces, which are essential for opening the respective compartments during arthroscopy.

Step-by-Step Surgical Approach and Fixation Technique
The surgical intervention commences with a systematic, comprehensive diagnostic arthroscopy to evaluate all compartments of the knee. The surgeon must meticulously probe the meniscus to assess tear morphology, tissue quality, and stability. A critical intraoperative decision-making step is evaluating the ability of the meniscus to "roll" or displace. An unstable tear will be easily mobilized and displaced by at least 7 mm under arthroscopic probing. If resection is deemed necessary for irreparably damaged tissue, all efforts must be directed toward preserving as much viable meniscus as possible, strictly avoiding damage to the meniscosynovial junction to maintain the integrity of the circumferential collagen fibers.
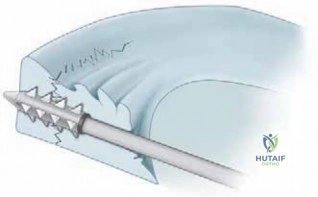
Biological preparation of the tear site is arguably as important as the mechanical fixation itself. To stimulate a robust healing response, the surgeon must perform aggressive synovial abrasion, meniscal rasping, and trephination. A meniscal rasp is used to excoriate the perimeniscal synovium and the edges of the tear, releasing chemotactic factors and creating a vascular access channel. Trephination involves passing a spinal needle multiple times through the vascular periphery into the avascular tear site to create vascular channels. In isolated meniscal repairs without concomitant ACL reconstruction, the introduction of a localized fibrin clot or the creation of a microfracture in the intercondylar notch is highly recommended to introduce bone marrow elements and essential growth factors into the joint space.
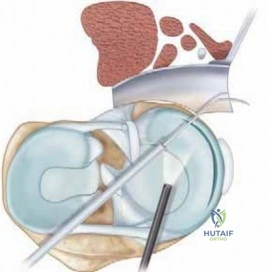

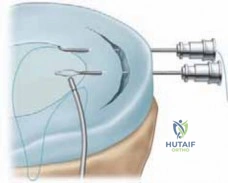
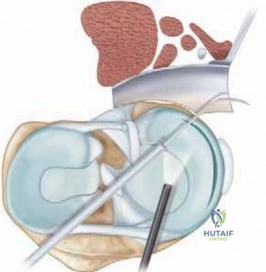
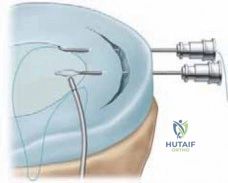
The inside-out repair technique remains the gold standard for tears located in the middle and posterior thirds of the meniscus due to its unparalleled biomechanical strength and versatility. This technique requires the precise placement of zone-specific, curved cannulas through the anterior portals. Long, flexible needles carrying non-absorbable or slowly absorbable sutures are passed through the meniscus and captured via a meticulously planned posterior safety incision. For medial repairs, a posteromedial incision is made posterior to the medial collateral ligament, carefully dissecting down to the capsule while strictly protecting the saphenous nerve and vein. For lateral repairs, a posterolateral approach requires interval dissection anterior to the biceps femoris and posterior to the iliotibial band, with absolute vigilance to protect the common peroneal nerve.

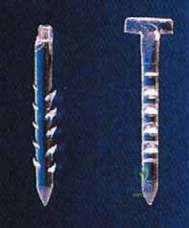
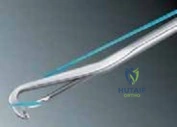
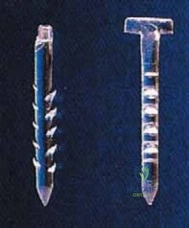
Alternatively, the outside-in technique is highly effective for anterior third tears, utilizing a spinal needle passed from the exterior of the knee through the capsule and into the meniscal tear. A suture is relayed through the needle, retrieved arthroscopically, and tied over the joint capsule using a Mulberry knot. In recent years, all-inside repair devices have gained massive popularity for posterior horn tears due to their ease of use and avoidance of accessory incisions. These devices utilize specialized deployment guns to place anchors behind the capsule, connected by a sliding, self-locking suture knot. Regardless of the technique chosen, sutures should be placed vertically whenever possible to capture the circumferential hoop fibers, and care must be taken to avoid over-tensioning, which can cause meniscal puckering and subsequent failure.



Complications, Incidence Rates, and Salvage Management
Complications following meniscal repair, while relatively infrequent, can be devastating to joint function and require prompt, decisive management. The most feared complications are iatrogenic neurovascular injuries, which are highly dependent on the surgical technique utilized. During medial inside-out repairs, the saphenous nerve and its infrapatellar branch are at significant risk if the posteromedial safety incision is poorly executed or if retractors are improperly placed. Conversely, lateral inside-out repairs place the common peroneal nerve in extreme jeopardy. Meticulous blunt dissection, appropriate use of a popliteal retractor, and keeping the knee flexed past 70 degrees during lateral needle passage are mandatory steps to mitigate these catastrophic risks.

The most common complication is the failure of the meniscal repair to heal, with non-healing rates ranging from 10% to 25% depending on the tear zone, chronicity, and the biological environment of the knee. Repairs performed concurrently with an ACL reconstruction demonstrate significantly higher healing rates due to the hemarthrosis and bone marrow elements released during tunnel drilling. Evaluating a suspected failed repair postoperatively presents a unique diagnostic challenge, as the repair site routinely fills with fibrous scar tissue that produces an abnormal, high-signal artifact on standard MRI. Currently, the most accurate non-invasive method for evaluating a symptomatic post-operative meniscus is a
Clinical & Radiographic Imaging Archive