Arthroscopic Microfracture Chondroplasty: A Masterclass in Cartilage Restoration

Key Takeaway
Join us in the OR for an immersive masterclass on arthroscopic microfracture chondroplasty. We'll meticulously cover patient selection, comprehensive knee anatomy, precise surgical execution from portal placement to subchondral drilling, and critical pearls to optimize outcomes. Learn to manage full-thickness chondral defects, emphasizing meticulous débridement, proper awl technique, and essential postoperative rehabilitation protocols for successful cartilage regeneration.
Comprehensive Introduction and Patho-Epidemiology
The management of full-thickness articular cartilage defects remains one of the most formidable challenges in orthopedic surgery. The foundational premise of arthroscopic microfracture chondroplasty—initially popularized by Richard Steadman in the late 1980s and 1990s—is the strategic utilization of the body's intrinsic marrow-derived mesenchymal stem cells to orchestrate a localized healing response. When meticulously executed and properly indicated, this marrow stimulation technique facilitates the formation of a fibrocartilaginous repair tissue matrix. This procedure relies on a fascinating interplay of biology and biomechanics, exploiting the pluripotency of bone marrow elements to bridge a defect in a tissue that is otherwise notoriously recalcitrant to spontaneous regeneration.
Articular cartilage is a highly specialized, isolated connective tissue covering the epiphyseal ends of diarthrodial joints. Its primary functions are to provide a low-friction gliding surface and to distribute applied mechanical loads across the underlying subchondral bone plate, thereby preventing localized stress concentrations. However, its evolutionary design comes with a significant physiological compromise: adult hyaline cartilage is fundamentally avascular, aneural, and alymphatic. This inherent lack of blood supply, innervation, and lymphatic drainage dictates that articular cartilage, once subjected to structural failure, cannot mount a standard inflammatory or reparative physiological response. The chondrocytes, which represent only 1% to 2% of the total tissue volume, are locked within a dense extracellular matrix and possess an exceptionally low mitotic rate, severely limiting their capacity to synthesize new matrix in response to macroscopic injury.

The pathogenesis of chondral defects is broadly categorized into acute traumatic events and chronic degenerative processes. Acute focal lesions are predominantly encountered in the younger, high-demand athletic population. These injuries typically result from a singular, high-energy shearing or impaction force—often sustained during a pivoting maneuver or direct axial load—that exceeds the ultimate tensile strength of the cartilage matrix. This mechanical failure can cause the cartilage to fissure, delaminate, or completely avulse from the tidemark, occasionally taking a fragment of the subchondral bone with it to create an osteochondral defect. Conversely, in the middle-aged demographic, chronic repetitive loading that subtly but persistently exceeds the physiological threshold of the tissue leads to fatigue failure. This microtraumatic cascade initiates structural degradation characterized by matrix swelling, disruption of the collagen fibril network, and a precipitous decline in proteoglycan concentration.

Regardless of the initial etiology, untreated full-thickness articular cartilage defects (Outerbridge or modified ICRS Grade IV lesions) that breach the subchondral bone plate possess an abysmal natural history. The exposed subchondral bone is subjected to unattenuated mechanical stress, leading to subchondral sclerosis, cyst formation, and the release of pro-inflammatory cytokines (such as IL-1β and TNF-α) into the synovial fluid. This biochemical hostility further degrades the surrounding intact cartilage, initiating a relentless degenerative cascade. While a subset of patients may remain transiently asymptomatic due to the aneural nature of the cartilage itself, the vast majority will inevitably develop debilitating mechanical symptoms, progressive joint effusion, and early-onset osteoarthritis. Microfracture intervenes in this cascade by accessing the vascularized marrow space, converting a chronic, non-healing defect into an acute, biologically active wound.
The Biological Imperative of Articular Cartilage
To master the technique of microfracture, the surgeon must possess a granular understanding of articular cartilage microanatomy. The tissue is hierarchically organized into four distinct zones: superficial (tangential), transitional (middle), deep (radial), and calcified. The superficial zone, characterized by densely packed collagen fibrils aligned parallel to the articular surface, provides the primary resistance to shear forces. As one progresses deeper, the collagen fibrils become thicker and orient perpendicularly to anchor into the calcified cartilage layer, an arrangement designed to resist compressive loads. The extracellular matrix is predominantly water (up to 80% by wet weight), Type II collagen, and large aggregating proteoglycans (primarily aggrecan) that generate a massive osmotic swelling pressure, giving the cartilage its unique viscoelastic properties.
When performing a microfracture, the biological goal is not the regeneration of true hyaline cartilage—which remains a holy grail of orthopedics—but rather the induction of a functional fibrocartilaginous substitute. True hyaline cartilage is defined by its high concentration of Type II collagen and specific proteoglycan architecture. In contrast, the repair tissue generated by marrow stimulation is predominantly composed of Type I collagen. While Type I collagen lacks the optimal compressive stiffness and wear characteristics of native Type II collagen, a well-integrated fibrocartilage clot provides a mechanically competent biological seal over the exposed subchondral bone. This seal mitigates pain by shielding the highly innervated subchondral plate and alters the intra-articular biochemical milieu by reducing the shedding of wear debris.
Pathogenesis of Chondral Defects
The biomechanical failure of articular cartilage is heavily influenced by the specific loading environment of the joint. In the knee, the medial femoral condyle is the most frequent site of focal chondral defects, largely due to the physiological varus alignment of the lower extremity that disproportionately loads the medial compartment during the stance phase of gait. When a shearing force is applied to a loaded, flexed knee, the superficial zone of the cartilage can be sheared off, or a deep cleavage plane can propagate down to the tidemark—the metabolically active boundary between the uncalcified deep zone and the calcified cartilage layer.
Once a fissure reaches the calcified layer or subchondral bone, the mechanical integrity of the entire functional unit is compromised. Synovial fluid, driven by high intra-articular pressures during weight-bearing, is forced into the defect. This hydrostatic pressure acts as a wedge, progressively delaminating the adjacent healthy cartilage from the underlying bone, much like a pothole expanding in a roadway. This phenomenon explains why small, neglected lesions often rapidly progress into massive geographic defects. The underlying subchondral bone, stripped of its protective shock absorber, undergoes a hypermetabolic response characterized by marrow edema, microtrabecular fractures, and eventual sclerosis, which critically alters the compliance of the joint surface.
Natural History and the Degenerative Cascade
The clinical trajectory of an untreated Grade IV chondral lesion is almost uniformly progressive, though the rate of deterioration varies based on patient age, body mass index, baseline alignment, and activity level. The initial presentation is often insidious; because the cartilage itself is aneural, early partial-thickness lesions (Grade I-III) may be completely painless. Pain typically manifests only when the lesion progresses to involve the richly innervated subchondral bone, or when detached chondral flaps cause mechanical impingement and secondary synovial inflammation.
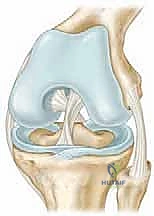
As the degenerative cascade accelerates, the joint enters a state of chronic synovitis. The inflamed synovium produces high levels of matrix metalloproteinases (MMPs) and aggrecanases (ADAMTS), enzymes that actively dismantle the collagen and proteoglycan framework of the remaining healthy cartilage. This creates a vicious cycle of mechanical wear leading to biological degradation, which in turn causes further mechanical failure. Microfracture aims to halt this cycle. By penetrating the subchondral plate, the surgeon intentionally induces localized bleeding, allowing mesenchymal stem cells, growth factors, and platelets to populate the defect. This "superclot" matures into fibrocartilage, effectively resurfacing the defect, restoring a measure of mechanical continuity, and silencing the inflammatory crosstalk between the subchondral bone and the joint space.
Detailed Surgical Anatomy and Biomechanics
The success of a microfracture chondroplasty is inextricably linked to the surgeon's respect for the complex microanatomy of the osteochondral unit. The osteochondral unit is not merely cartilage sitting on top of bone; it is a highly integrated, functionally graded material transition from compliant articular cartilage to rigid subchondral bone. Understanding this transitional anatomy is critical, particularly regarding the calcified cartilage layer. The calcified layer acts as a mechanical buffer, reducing the stiffness gradient between the uncalcified deep zone cartilage and the subchondral bone plate.
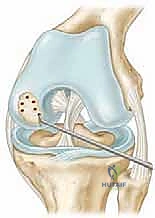
During the preparation of a chondral defect for microfracture, the complete removal of this calcified cartilage layer is the most critical, yet frequently under-executed, step of the procedure. If the calcified layer is left intact, the marrow-derived superclot will fail to adhere securely to the base of the defect, leading to early delamination of the repair tissue. The calcified layer is relatively avascular and presents a hostile, smooth surface for clot integration. The surgeon must meticulously use ring curettes to scrape the base of the lesion until the rough, punctate vascularity of the true subchondral bone plate is exposed, ensuring not to aggressively burr into the bone, which can cause thermal necrosis and destroy the delicate microvasculature necessary for the healing response.
Microanatomy and Matrix Composition
The extracellular matrix of normal hyaline cartilage is a marvel of biological engineering. The structural backbone is a three-dimensional arcade-like network of Type II collagen fibrils, which provides the tissue with its remarkable tensile strength. Entangled within this collagen meshwork are massive proteoglycan aggregates, primarily aggrecan, which are highly negatively charged due to their chondroitin sulfate and keratin sulfate side chains. These negative charges repel each other and attract cations, drawing water into the matrix via the Donnan osmotic effect. This creates a massive internal swelling pressure that is resisted by the tensile strength of the collagen network.
When a microfracture is performed, the resulting fibrocartilage repair tissue lacks this sophisticated architectural arrangement. Fibrocartilage is dominated by Type I collagen, which forms thick, disorganized bundles rather than the fine, highly organized arcade structure of Type II collagen. Furthermore, the proteoglycan concentration in fibrocartilage is significantly lower, meaning it cannot generate the same internal osmotic swelling pressure. Consequently, fibrocartilage is biomechanically inferior; it is more permeable, less stiff in compression, and more susceptible to shear forces. This fundamental biological limitation dictates the strict postoperative rehabilitation protocols required to protect the maturing clot and explains why microfracture is generally reserved for smaller lesions (typically less than 2 to 3 square centimeters) where the surrounding healthy native cartilage can shield the repair tissue from excessive loads.
Biomechanical Load Distribution
The knee joint is subjected to extraordinary mechanical demands, routinely experiencing contact pressures that exceed several multiples of body weight during normal ambulation, and exponentially more during athletic activities. The distribution of these loads is critically dependent on the integrity of the menisci and the articular cartilage, as well as the overall coronal and sagittal alignment of the lower extremity. In a normally aligned knee, the mechanical axis passes through the center of the joint, distributing loads relatively evenly between the medial and lateral compartments.
When a focal full-thickness defect occurs, the local biomechanics are drastically altered. The area of the defect no longer supports load, transferring the stress to the rim of the adjacent healthy cartilage. This phenomenon, known as rim stress concentration, leads to accelerated breakdown of the surrounding native tissue. The primary biomechanical objective of the microfracture-induced fibrocartilage clot is to fill this void, re-establishing a continuous articular surface that can participate in load sharing, thereby relieving the pathological stress concentrations on the adjacent healthy cartilage margins. If the defect is left uncontained (i.e., lacking a vertical wall of healthy cartilage on all sides), the fibrocartilage clot will lack the necessary mechanical support to withstand physiological shear forces, leading to premature failure.
The Subchondral Bone Plate Interface
The subchondral bone plate is a dense, highly mineralized layer of bone immediately deep to the calcified cartilage. It is perforated by microscopic vascular channels that allow for limited metabolic exchange between the marrow space and the deep layers of the cartilage. In the setting of a chronic Grade IV lesion, this bone plate undergoes significant pathological changes. In response to unattenuated mechanical loading, the bone becomes highly sclerotic, thickening and losing its normal porosity. This sclerotic bone is exceptionally hard and relatively avascular, presenting a significant barrier to marrow stimulation.
Penetrating this sclerotic subchondral plate is the mechanical crux of the microfracture procedure. The surgeon must use specialized, sharp surgical awls to breach this dense bone and access the underlying cancellous marrow cavity. The depth of penetration is critical; it must be deep enough (typically 2 to 4 millimeters) to reliably access the vascular marrow and release mesenchymal stem cells, but not so deep as to severely compromise the structural integrity of the subchondral plate, which could lead to subchondral cyst formation or structural collapse. The microfracture holes must be placed close enough together to ensure confluent bleeding across the entire defect bed, yet far enough apart (typically 3 to 4 millimeters) to prevent the holes from coalescing and fracturing the bone bridge between them.
Exhaustive Indications and Contraindications
The clinical success of arthroscopic microfracture is profoundly dependent on meticulous patient selection. Microfracture is not a panacea for all knee pain, nor is it an appropriate treatment for generalized osteoarthritis. It is a highly specific, biologically demanding procedure designed for a narrow subset of pathology: the symptomatic, isolated, full-thickness articular cartilage defect in a well-aligned, stable joint. The ideal candidate is a younger, active patient with an acute or subacute focal traumatic lesion, surrounded by robust, healthy native cartilage that can provide a protective "shoulder" for the regenerating fibrocartilage clot.
Conversely, applying microfracture to inappropriately selected patients—such as those with uncorrected malalignment, ligamentous instability, or diffuse degenerative joint disease—will invariably lead to early clinical failure and accelerated joint destruction. The biological potential of marrow-derived stem cells cannot overcome a hostile biomechanical environment. Therefore, a rigorous, algorithmic approach to indications and contraindications is the absolute foundation of successful cartilage restoration surgery.
Patient Selection Criteria
Patient selection must synthesize clinical, radiographic, and patient-specific variables. The primary indication is a symptomatic, full-thickness (Outerbridge Grade IV or ICRS Grade IV) chondral defect of the femoral condyle, trochlea, or patella. The lesion should ideally be focal and contained, meaning it is surrounded on all sides by a rim of healthy, normal-thickness cartilage. Lesion size is a critical determinant of success; while there is no absolute cutoff, outcomes are significantly superior for lesions smaller than 2.5 to 3.0 square centimeters. Larger lesions have a higher failure rate because the biomechanically inferior fibrocartilage cannot sustain widespread load-bearing without the protective shielding of adjacent native cartilage.
Patient age is a significant, though relative, factor. The pluripotency and concentration of bone marrow mesenchymal stem cells decline with advancing age. Consequently, microfracture yields the most robust and durable results in patients under the age of 40. While the procedure can be performed in older patients, particularly those with traumatic lesions rather than degenerative wear, the surgeon must counsel these patients that the quality of the repair tissue and the longevity of the clinical benefit may be reduced. Furthermore, the patient must possess the psychological resilience and logistical capacity to adhere strictly to a demanding, multi-month postoperative rehabilitation protocol, which often involves prolonged periods of restricted weight-bearing and continuous passive motion.
Absolute and Relative Contraindications
The contraindications to microfracture are primarily biomechanical and biological. The most critical absolute contraindication is uncorrected axial malalignment. If the mechanical axis of the lower extremity passes through the compartment containing the chondral defect, the excessive compressive and shear forces will rapidly destroy the delicate fibrocartilage clot. For example, a medial femoral condyle defect in a patient with significant varus alignment will fail unless a concurrent or staged high tibial osteotomy (HTO) is performed to unload the medial compartment. Similarly, untreated ligamentous instability (e.g., an ACL-deficient knee) introduces pathological shear forces that are lethal to maturing repair tissue; stability must be restored prior to or concurrently with cartilage restoration.
Other absolute contraindications include partial-thickness defects (Grade I-III), as the intact deep layers of cartilage prevent access to the marrow space, and attempting microfracture would only damage functional tissue. Global degenerative joint disease or inflammatory arthropathies (like rheumatoid arthritis) represent a biologically hostile environment where isolated marrow stimulation is futile. Relative contraindications include advanced patient age (typically over 50-55 years), morbid obesity (which exponentially increases joint contact forces), and a history of smoking, which severely compromises the microvascular response essential for clot formation and maturation.
| Category | Specific Criteria / Condition | Rationale |
|---|---|---|
| Absolute Indications | Focal, symptomatic Grade IV defect | Requires exposed subchondral bone to access marrow elements. |
| Intact meniscus and stable ligaments | Prevents pathological shear and excessive contact pressures. | |
| Normal axial alignment | Ensures physiological load distribution away from the repair site. | |
| Relative Indications | Lesions < 3.0 cm² in size | Fibrocartilage cannot support massive loads without native cartilage shielding. |
| Patient age < 40-45 years | Higher concentration and viability of mesenchymal stem cells. | |
| Absolute Contraindications | Uncorrected malalignment (>50% deviation) | Mechanical overload guarantees rapid destruction of the fibrocartilage clot. |
| Uncorrected ligamentous instability | Pathological anterior/posterior or rotational shear destroys the repair tissue. | |
| Inflammatory arthropathy or diffuse OA | Hostile biochemical milieu and lack of contained borders for the clot. | |
| Relative Contraindications | Morbid Obesity (BMI > 35) | Exponentially increased joint reactive forces exceed fibrocartilage capacity. |
| Smoking / Nicotine use | Impairs angiogenesis and the critical initial biological healing response. |
Pre-Operative Planning, Imaging, and Patient Positioning
The clinical diagnosis of an isolated chondral defect is notoriously challenging, as the presentation often mimics, or coexists with, other common intra-articular pathologies such as meniscal tears or plica syndrome. A meticulous preoperative evaluation is mandatory to confirm the diagnosis, accurately size the lesion, and critically evaluate the entire joint ecosystem—including alignment, stability, and meniscal volume. This comprehensive assessment ensures that all concomitant pathologies that could compromise the microfracture are identified and addressed in the surgical plan.
The physical examination must be systematic and exhaustive. Patients typically report a deep, poorly localized aching pain that is exacerbated by weight-bearing activities, stair climbing, or prolonged sitting with the knee flexed (the "theater sign," highly indicative of patellofemoral lesions). Mechanical symptoms such as catching, clicking, or true locking are common, often caused by unstable, delaminated cartilage flaps acting as a loose body within the joint articulation. The presence of a chronic, low-grade effusion is frequently noted, representing the synovium's inflammatory response to cartilage wear debris.
Clinical Evaluation and Physical Examination
During the physical examination, precise palpation is essential. While point tenderness along the joint line is classically associated with meniscal tears, tenderness directly over the femoral condyles when the knee is flexed can indicate a focal chondral lesion. The examiner must assess the patellofemoral joint meticulously; pain elicited with active patellar compression against the trochlea strongly suggests chondral damage in this compartment. Range of motion (ROM) must be documented; a mechanical block to full extension may indicate a displaced osteochondral fragment or a bucket-handle meniscal tear requiring immediate attention.
Crucially, the integrity of all major ligamentous structures must be verified. A Lachman test, anterior drawer, and pivot shift test are mandatory to rule out anterior cruciate ligament (ACL) insufficiency. Varus and valgus stress testing at 0 and 30 degrees of flexion assesses the collateral ligaments. Any identified instability is a major red flag; performing a microfracture in an unstable knee is an exercise in futility, as the abnormal kinematics will shear the healing clot off the subchondral bone. Concomitant stabilization procedures must be integrated into the surgical plan if instability is present.
Advanced Imaging and Alignment Assessment
Radiographic evaluation begins with a standard, high-quality knee series: weight-bearing anteroposterior (AP), 45-degree flexion weight-bearing posteroanterior (Rosenberg view), lateral, and Merchant (patellofemoral) views. These basic films are essential for ruling out gross osteoarthritis, joint space narrowing, and large osteochondral loose bodies. However, the most critical radiographic study in the preoperative planning of any cartilage restoration procedure is the full-length, 51-inch standing hip-to-ankle radiograph. This film allows for the precise calculation of the mechanical axis of the lower extremity.
The mechanical axis is determined by drawing a line from the center of the femoral head to the center of the tibial plafond. In a neutrally aligned knee, this line should pass through the central 25% of the tibial plateau. If the axis deviates significantly into the compartment harboring the chondral defect, the joint reactive forces in that area are pathologically elevated.

As a strict rule, if the mechanical axis falls greater than 50% into the affected compartment (e.g., severe varus with a medial condyle defect), isolated microfracture is absolutely contraindicated. The mechanical overload must be corrected via a realignment osteotomy to shift the weight-bearing axis away from the regenerating tissue.
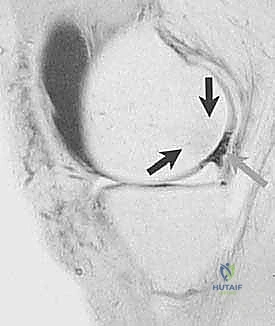
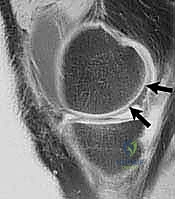
Magnetic Resonance Imaging (MRI) is the gold standard for non-invasive evaluation of articular cartilage. High-resolution, fast spin-echo (FSE) proton density sequences or specialized cartilage-sensitive sequences (like 3D SPGR or dGEMRIC) provide exquisite detail of the cartilage morphology. MRI allows the surgeon to accurately measure the length and width of the defect, assess the integrity of the opposing articular surface ("kissing lesions" are a poor prognostic sign), and evaluate the underlying subchondral bone for reactive edema or cystic changes, which dictate the depth of debridement required during surgery.
Operating Room Setup and Patient Positioning
Optimal patient positioning is paramount for achieving the precise instrument angles required for a successful microfracture. The procedure is performed under general or regional anesthesia. Prior to standard sterile prepping and draping, a comprehensive Examination Under Anesthesia (EUA) is performed to verify ligamentous stability and range of motion without the confounding variable of patient guarding. The patient is positioned supine on the operating table. A non-sterile tourniquet is applied to the proximal thigh, though it is often left uninflated unless visualization becomes compromised by bleeding, as a tourniquet-free environment allows for immediate visual confirmation of marrow bleeding during the awl penetration step.

For the initial diagnostic arthroscopy and treatment of concomitant meniscal pathology, the leg is typically held in a standard leg holder or positioned over a post with the foot resting on the table. However, for the definitive microfracture of the femoral condyles or trochlea, hyperflexion and unhindered manipulation of the joint are often required. To achieve this, the distal portion of the operating table is dropped, allowing the operative leg to hang freely at 90 degrees of flexion.
This dependent position opens the anterior joint space, vastly improving access to the posterior aspects of the femoral condyles and allowing the surgeon to approach the defect perpendicularly with the microfracture awls—a geometric necessity for creating clean, cylindrical holes in the subchondral plate without skiving or fracturing the surrounding bone.
Step-by-Step Surgical Approach and Technique
The execution of an arthroscopic microfracture chondroplasty is an exercise in meticulous surgical discipline. The procedure can be conceptually divided into three critical phases: defect preparation (debridement and containment), marrow stimulation (awl penetration), and biological verification (clot visualization). Failure at any of these stages compromises the entire biological cascade, leading to a high probability of clinical failure. The surgeon must utilize standard anterolateral and anteromedial arthroscopic portals, frequently employing accessory portals to ensure that instruments can approach the defect at a perpendicular angle, which is essential for proper debridement and awl placement.
The initial phase involves a comprehensive diagnostic arthroscopy to catalog all intra-articular pathology. The entire joint is systematically probed, evaluating the menisci, cruciate ligaments, and all articular surfaces. Any unstable meniscal tears are addressed first, typically via partial meniscectomy or repair, to eliminate mechanical impingement. Once the joint is cleared of secondary pathology, attention is focused on the focal chondral defect. The lesion is carefully probed to define its true extent; often, visually intact cartilage at the periphery of the defect is actually delaminated from the subchondral bone and must be considered part of the functional lesion.

Diagnostic Arthroscopy and Lesion Preparation
The preparation of the
Clinical & Radiographic Imaging Archive