Arthroscopic Meniscectomy: An Intraoperative Masterclass in Meniscal Pathology and Resection

Key Takeaway
This masterclass provides an exhaustive guide to arthroscopic meniscectomy. We delve into intricate meniscal anatomy, tear classifications, and biomechanics. Fellows will learn preoperative planning, meticulous intraoperative execution from portal placement to precise tissue resection, and critical pearls for avoiding complications. Postoperative care and rehabilitation strategies are also thoroughly discussed, ensuring a comprehensive understanding of this common knee procedure.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are undertaking a masterclass in arthroscopic meniscectomy, a fundamental yet highly nuanced procedure in orthopaedic surgery. While the technical execution of removing meniscal tissue may initially appear straightforward to the uninitiated, the true art of this procedure lies in the rigorous application of meniscal biomechanics and the meticulous preservation of functional tissue. Our overarching objective is never merely the extirpation of a torn fragment; rather, it is the deliberate, architectural sculpting of a stable, smooth meniscal rim designed to mitigate subsequent tibiofemoral contact stresses and delay the inevitable progression of degenerative joint disease. Historically, total meniscectomy was the standard of care, based on the erroneous belief that the meniscus was a vestigial structure. We now recognize that such an approach guarantees early, severe osteoarthritis, famously described as Fairbank's changes.
Before we even consider making a scalpel incision or establishing our arthroscopic portals, we must possess an exhaustive understanding of the pathology we are addressing. Meniscal tears present in a myriad of morphologic patterns, each carrying distinct implications for the patient's symptomatology, the knee's biomechanical integrity, and our ultimate surgical algorithm. The epidemiology of meniscal pathology is broadly bifurcated into acute traumatic tears, typically seen in younger, athletic populations, and chronic degenerative tears, which are ubiquitous in the aging demographic. The etiology dictates the tissue quality; traumatic tears often occur in pristine, robust fibrocartilage, whereas degenerative tears occur in myxoid, structurally compromised tissue that alters our tactile feedback and resection strategy during surgery.
The vascular anatomy of the meniscus is the primary determinant of our treatment algorithm. We categorize tears based on their reparability, which is intrinsically linked to the perimeniscal capillary plexus originating from the genicular arteries. In the adult knee, only the peripheral 10% to 30% of the meniscus is vascularized (the "red-red" zone). Tears located in the central, avascular portion—the "white-white" zone—are incapable of mounting a fibroblastic healing response. These are the classic, irreparable meniscal tears that necessitate meniscectomy. Our surgical intervention may involve removing all or part of the affected tissue, leading to a partial, subtotal, or, in exceedingly rare and catastrophic cases, total meniscectomy.
Our unyielding aim is to perform the most limited resection mathematically possible to restore a stable mechanical environment while preserving meniscal volume. Tears in the white zone typically require partial meniscectomy, involving the inner two-thirds of the meniscus where the blood supply is entirely insufficient to support biological repair. Understanding the precise transition from the avascular inner zone to the vascularized periphery is critical; resecting too far peripherally not only removes functional load-bearing tissue but also risks violating the vascular zone, leading to unnecessary hemarthrosis and compromising the structural hoop integrity of the remaining meniscal rim.
Detailed Surgical Anatomy and Biomechanics
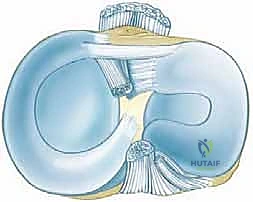
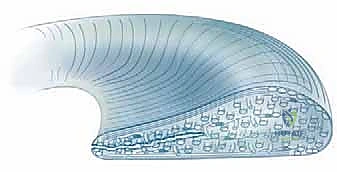
To master arthroscopic meniscectomy, one must possess an encyclopedic knowledge of meniscal anatomy and its profound biomechanical implications. The menisci are crescent-shaped, biphasic fibrocartilaginous structures, roughly triangular in cross-section, that cover approximately one-half to two-thirds of the articulating surface of the corresponding tibial plateaus. They are composed primarily of water (72%) and organic matter (28%), with Type I collagen constituting the vast majority of the dry weight. This dense, tightly woven collagenous framework is embedded within an extracellular matrix of proteoglycans and glycoproteins, providing the meniscus with its unique viscoelastic properties, elasticity, and unparalleled ability to withstand immense compressive loads.

The microstructural organization of these collagen fibers is the secret to meniscal function. The major orientation of collagen fibers is circumferential, running parallel to the peripheral border of the meniscus. These fibers act precisely like the metal hoops bound around a pressurized wooden barrel; their tension keeps the meniscal body in place, dissipating axial loads outward. This is known as "hoop tension." Radial fibers, also known as tie fibers, run perpendicular to the circumferential fibers, acting to bind them together and resist longitudinal splitting. Perforating fibers further interlock the matrix. When subjected to biomechanical testing, meniscal tensile strength decreases by over 90% when force is applied perpendicular to the circumferential fiber direction.
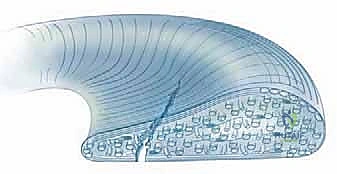

This complex arrangement dictates the characteristic patterns of meniscal tears we observe intraoperatively. A loss of hoop tension—often caused by a single, unaddressed radial cut or a tear extending completely to the capsular margin—functionally equates to a total meniscectomy. The meniscus loses its ability to convert axial tibiofemoral loads into circumferential tension, leading to extrusion of the meniscus and an exponential increase in peak contact stresses on the articular cartilage. Therefore, preserving the continuity of the peripheral circumferential fibers is the single most critical biomechanical objective during partial meniscectomy.

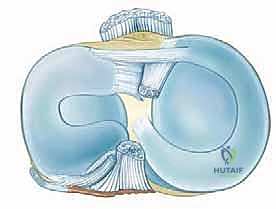
Macroscopically, the medial and lateral menisci exhibit distinct anatomic and kinematic profiles. The medial meniscus is a larger, C-shaped structure with a posterior horn that is significantly wider than its anterior horn. It is firmly anchored to the tibial plateau via the anterior and posterior root attachments, and its entire peripheral border is rigidly attached to the deep medial collateral ligament and the joint capsule via the coronary ligaments. This rigid fixation makes the medial meniscus relatively immobile, rendering it highly susceptible to shear forces and longitudinal tearing during rotational stress, particularly when the knee is flexed and internally rotated. Conversely, the lateral meniscus is more circular, covers a larger percentage of the tibial plateau, and is significantly more mobile. Its peripheral attachment is interrupted by the popliteus hiatus, and it receives dynamic stabilization from the meniscofemoral ligaments (Wrisberg and Humphrey). This mobility allows the lateral meniscus to translate posteriorly during knee flexion, protecting it from being crushed between the condyles, which explains why lateral bucket-handle tears are less common than their medial counterparts.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic meniscectomy requires a rigorous clinical synthesis of the patient's history, physical examination, and advanced imaging. The absolute indication for urgent surgical intervention is mechanical locking of the knee joint. This occurs when a displaced meniscal fragment—most classically a bucket-handle tear or a large, pedunculated flap tear—interposes itself within the intercondylar notch or the tibiofemoral articulation, physically blocking terminal extension. This mechanical block not only causes severe pain but also places the articular cartilage at immediate risk of focal chondral injury and necessitates prompt arthroscopic reduction and resection or repair.
We categorize tears based on their morphologic pattern, which dictates our surgical approach. Longitudinal tears, running parallel to the circumferential fibers, are the most common and often involve the posterior horn. If these displace, they become bucket-handle tears. Complex transverse and longitudinal tears are typically the hallmark of degenerative joint disease or repeated microtrauma. Transverse, radial, or oblique tears disrupt the vital circumferential fibers; if they extend to the periphery, they destroy hoop tension. Horizontal cleavage tears split the meniscus into superior and inferior leaves and are frequently associated with parameniscal cysts, particularly on the lateral side. Symptomatic tears of discoid lateral menisci—congenital anomalies characterized by a thickened, hypermobile, and structurally inferior meniscus—frequently require partial or subtotal saucerization to relieve snapping and pain.

Conversely, the contraindications to meniscectomy are equally critical to understand. The most significant contraindication is a tear that is amenable to primary repair. Tears located in the vascular red-red or red-white zones, particularly in young, active patients or those with concomitant anterior cruciate ligament (ACL) reconstructions, should be meticulously repaired rather than resected. Furthermore, asymptomatic degenerative meniscal tears discovered incidentally on MRI should never be subjected to prophylactic meniscectomy. Performing a meniscectomy in a knee with advanced, bone-on-bone osteoarthritis (Kellgren-Lawrence Grade 3 or 4) is generally contraindicated, as the removal of the remaining meniscal tissue will only exacerbate the mechanical overload and accelerate the patient's symptoms, often leading to a rapid decline requiring arthroplasty.
Table of Indications and Contraindications
| Category | Specific Clinical Scenarios | Rationale / Surgical Implications |
|---|---|---|
| Absolute Indications | Mechanical locking (e.g., displaced bucket-handle tear) | Immediate risk to articular cartilage; physical block to range of motion requires urgent mechanical resolution. |
| Relative Indications | Symptomatic avascular tears failing conservative therapy | Pain and effusion driven by unstable flaps in the white-white zone; requires partial resection to stable rim. |
| Specific Indications | Symptomatic Discoid Meniscus, Parameniscal Cysts | Requires saucerization to restore normal morphology and decompression of the cyst via intra-articular ostium. |
| Absolute Contraindications | Reparable tears in the red-red / red-white zone | Biological healing is possible; preservation of meniscal volume is paramount to prevent early-onset osteoarthritis. |
| Relative Contraindications | Advanced Osteoarthritis (KL Grade 3-4) | Meniscectomy removes the last remaining shock absorber, often severely worsening the patient's arthritic pain. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning begins with a meticulous physical examination. We rely on provocative maneuvers such as the McMurray test, Apley's grind test, and the Thessaly test to localize the pathology. Joint line tenderness remains one of the most sensitive indicators of a meniscal tear. Following the clinical assessment, high-resolution Magnetic Resonance Imaging (MRI) is the gold standard for evaluating meniscal pathology. We carefully scrutinize the T1, T2, and proton density (PD) fat-suppressed sequences in the sagittal, coronal, and axial planes. We must differentiate a true meniscal tear—defined as high signal unequivocally communicating with an articular surface—from intrasubstance myxoid degeneration, which does not require surgical intervention.
In the operating room, patient positioning and setup are foundational to a flawless execution. The procedure is typically performed under general or regional anesthesia. The patient is positioned supine on the operating table. A non-sterile tourniquet is applied to the proximal thigh of the operative leg, though its inflation is often reserved for cases where visualization is compromised by excessive bleeding. The leg is either placed in a specialized circumferential leg holder, which allows for the application of valgus and varus stress to open the medial and lateral compartments respectively, or a lateral post is utilized. The contralateral leg is carefully padded and placed in a well-leg support to prevent deep vein thrombosis and nerve compression.
The surgical equipment must be meticulously organized before the first incision. A standard 30-degree, 4.0-mm arthroscope is utilized for the majority of the procedure, though a 70-degree scope should be readily available for visualizing the posterior horns and the meniscal roots. A comprehensive array of arthroscopic instruments must be on the Mayo stand, including straight and angled arthroscopic biters (punches), grasping forceps, a calibrated arthroscopic probe, and motorized shavers (typically 4.0 mm or 4.5 mm oscillating blades). Radiofrequency (RF) wands are also prepared for achieving hemostasis and performing final, delicate contouring of the meniscal rim.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with the establishment of precise arthroscopic portals. The standard anterolateral (AL) and anteromedial (AM) portals are the workhorses of knee arthroscopy. The AL portal is typically established first, located adjacent to the lateral border of the patellar tendon and approximately 1 cm above the joint line. After insufflating the knee with normal saline, the arthroscope is introduced, and a systematic, eight-point diagnostic sweep of the joint is performed. This includes the suprapatellar pouch, the patellofemoral articulation, the medial gutter, the medial compartment, the intercondylar notch, the lateral compartment, and the lateral gutter. The AM portal is then established under direct intra-articular visualization, utilizing a spinal needle to ensure the optimal trajectory for instrument access to the targeted meniscal pathology.
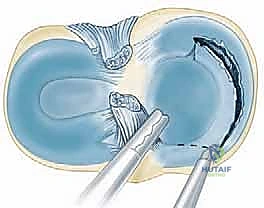

Once the tear is identified and probed to confirm its irreparability, the resection phase commences. The fundamental principle of partial meniscectomy is to resect the unstable, torn fragments while leaving a perfectly contoured, stable peripheral rim. We employ a "bite-and-pull" or "punch" technique using arthroscopic biters. For a standard flap tear, the base of the flap is identified, and the biter is used to amputate the fragment. It is imperative to avoid taking excessively large bites, which can lead to inadvertent damage to the adjacent articular cartilage or the creation of iatrogenic radial tears in the remaining meniscal rim.
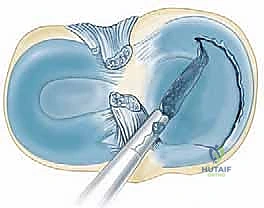

Handling complex tear patterns requires advanced spatial awareness and technical dexterity. For a displaced bucket-handle tear that cannot be repaired, the fragment is often amputated en bloc. This involves detaching the anterior horn attachment of the displaced fragment, then carefully transitioning to the posterior attachment, ensuring the fragment is securely held with a grasper before the final cut is made to prevent it from floating away into the posterior compartment. For horizontal cleavage tears, the superior or inferior leaf (whichever is more unstable or thinner) is resected, while the more robust leaf is preserved to maintain some degree of shock absorption.

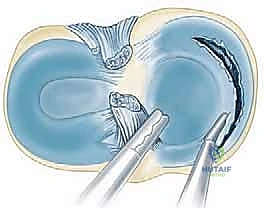
Following the macroscopic resection with biters, the motorized shaver is introduced to meticulously contour the remaining meniscal rim. The goal is to eliminate any sharp transitions or sudden step-offs, which can act as stress risers and propagate future tears. The shaver is used in an oscillating mode, lightly sweeping across the meniscal edge to create a smooth, gently tapering profile. Throughout this process, the surgeon must constantly balance the need to remove unstable tissue against the absolute necessity of preserving the peripheral circumferential fibers to maintain hoop tension.
In cases of a discoid lateral meniscus, the procedure is termed a "saucerization." The objective here is to reshape the abnormal, block-like meniscus into a functional, crescentic shape. This requires extensive resection of the central portion of the meniscus, carefully tapering the tissue from the thick periphery down to a thin, unattached central edge. Great care must be taken during saucerization to avoid destabilizing the peripheral attachments, as discoid menisci frequently have anomalous or deficient peripheral capsular fixation, which may require concomitant repair if unmasked during the resection.
Complications, Incidence Rates, and Salvage Management
Despite being one of the most commonly performed orthopaedic procedures worldwide, arthroscopic meniscectomy is not without significant risks and potential complications. Intraoperative complications are primarily related to iatrogenic injury. The most frequent of these is scuffing or gouging of the articular cartilage, typically occurring during the insertion of instruments through tight portals or when navigating the posterior compartments in a tight knee. The incidence of clinically significant iatrogenic chondral injury is estimated at 1-2%, but minor scuffing is likely underreported. Neurovascular injuries are exceedingly rare but catastrophic; the popliteal artery is at risk during aggressive posterior horn resections, and the saphenous nerve (specifically its infrapatellar branch) can be injured during the establishment of the anteromedial portal.
The most profound long-term complication of meniscectomy is the development of post-meniscectomy syndrome and accelerated osteoarthritis. The removal of meniscal tissue exponentially increases the contact stresses across the tibiofemoral joint. Studies have shown that even a 10% reduction in contact area can increase peak contact stresses by over 60%. Over time, this mechanical overload leads to the breakdown of the articular cartilage, subchondral sclerosis, and osteophyte formation. The incidence of post-operative osteoarthritis is directly proportional to the volume of meniscus removed and the status of the underlying cartilage at the time of surgery.
Other post-operative complications include hemarthrosis, deep vein thrombosis (DVT), and surgical site infection. Hemarthrosis usually results from aggressive resection into the vascularized red zone without adequate hemostasis, or from a post-operative tear of a capsular vessel. Infection in knee arthroscopy is rare, occurring in less than 0.5% of cases, but requires emergent arthroscopic irrigation and debridement if septic arthritis develops. DVT prophylaxis is generally not mandated for routine, brief meniscectomies in healthy patients but should be considered in patients with known hypercoagulable states or a history of venous thromboembolism.
When a patient develops severe, unremitting pain following a subtotal or total meniscectomy—a condition termed post-meniscectomy syndrome—salvage options must be considered. In young, active patients with normal mechanical alignment and minimal diffuse chondral damage, Meniscal Allograft Transplantation (MAT) is the gold standard salvage procedure. MAT aims to restore joint biomechanics, reduce pain, and potentially delay arthroplasty. If the patient has concomitant malalignment (e.g., varus alignment with a medial meniscectomy), a corrective osteotomy (such as a High Tibial Osteotomy) must be performed, either in isolation or concurrently with MAT, to offload the affected compartment.
Table of Complications and Salvage Management
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Iatrogenic Cartilage Injury | 1% - 3% | Use meticulous portal placement; avoid leveraging instruments; salvage via chondroplasty or microfracture if full-thickness. |
| Post-Meniscectomy Osteoarthritis | 20% - 40% (Long-term) | Strict adherence to maximal tissue preservation; salvage via Meniscal Allograft Transplantation (MAT) or Osteotomy. |
| Surgical Site Infection / Septic Arthritis | < 0.5% | Pre-operative weight-based antibiotics; sterile technique; salvage requires emergent arthroscopic I&D and targeted IV antibiotics. |
| Neurovascular Injury (Popliteal / Saphenous) | < 0.1% | Maintain safe zones during posterior horn resection; avoid plunging; vascular surgery consultation for arterial repair. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following an isolated partial meniscectomy is generally rapid, but it must be structured and phased to ensure optimal recovery and prevent early joint effusion. Phase 1, the immediate post-operative phase (Days 1 to 7), focuses on controlling inflammation, restoring full terminal knee extension, and re-establishing quadriceps control. Patients are typically allowed to bear weight as tolerated with crutches, transitioning to full weight-bearing as their quadriceps strength permits. Cryotherapy and compression are utilized aggressively to manage the inevitable post-operative hemarthrosis and effusion. Early range of motion (ROM) exercises, such as heel slides and prone hangs, are initiated immediately.
Phase 2, the intermediate phase (Weeks 1 to 3), begins when the patient has minimal effusion, full or near-full ROM, and the ability to perform a straight leg raise without an extensor lag. The focus shifts to progressive strengthening of the quadriceps, hamstrings, and gluteal musculature. Closed kinetic chain exercises, such as mini-squats, leg presses, and stationary cycling, are introduced to stimulate proprioception and muscular endurance while minimizing shear forces across the joint. Balance and neuromuscular control exercises are also incorporated to prepare the lower extremity for more dynamic loads.
Phase 3, the advanced strengthening and return-to-sport phase (Weeks 3 to 6+), is tailored to the patient's specific athletic or occupational demands. This phase introduces plyometrics, agility drills, and sport-specific functional movements. Running and high-impact activities are gradually reintroduced only when the patient demonstrates symmetrical lower extremity strength (typically >85% compared to the contralateral limb on isokinetic testing) and exhibits no reactive effusions following strenuous workouts.
It is
