

Comprehensive Introduction and Patho-Epidemiology
The knee is unquestionably the most frequently studied region of the appendicular skeleton, demanding a rigorous, multifaceted understanding of both its complex biomechanics and the sophisticated advanced imaging modalities required for precise diagnostic evaluation. The intersection of high-resolution magnetic resonance imaging (MRI) and minimally invasive arthroscopic surgical techniques has radically transformed the management algorithms for intra-articular knee pathologies. Standard extremity coils allow for the acquisition of high-resolution images of the commonly injured internal structures of the joint, facilitating a level of preoperative planning that was previously unimaginable. The routine MRI examination of the knee consists of meticulously protocolled spin-echo sequences obtained in sagittal, coronal, and usually axial planes, each tailored to highlight specific anatomical and pathological nuances.
Epidemiologically, knee pathologies represent a massive burden of musculoskeletal disease, encompassing acute traumatic injuries, repetitive microtrauma, and progressive degenerative conditions. Anterior cruciate ligament (ACL) ruptures occur with an estimated incidence of over 200,000 cases annually in the United States alone, predominantly affecting young, active individuals engaged in pivoting and cutting sports. The patho-epidemiology of these injuries often reveals a non-contact, deceleration, or valgus-abduction mechanism, resulting in catastrophic failure of the ligamentous architecture. Concurrently, meniscal tears are ubiquitous, with a bimodal distribution characterizing acute, high-energy tears in the athletic population and insidious, degenerative cleavage tears in the older demographic. A vast percentage of knee pain and mechanical disability is directly caused by these pathological conditions of the menisci, which compromise the joint's critical load-transmission capabilities.
Furthermore, osteochondral lesions and marrow pathologies present a distinct epidemiological challenge, often manifesting as osteochondritis dissecans (OCD) in the pediatric and adolescent populations or as focal chondral defects in adults following focal trauma. Advanced MRI sequences are critical in surgical planning by defining the exact extent of osseous and cartilaginous disease. Certain fat-suppressed sequences are exquisitely sensitive; reactive marrow edema can be visualized well before frank osteomyelitis or structural collapse occurs. Although the sensitivity of MRI for osteomyelitis approaches 100%, the reported specificity is lower. Consequently, it is imperative to rely on T1-weighted marrow replacement rather than isolated T2-weighted signal abnormalities to confirm infection.
These imaging principles apply universally across the lower extremity, providing a diagnostic continuum from the hip to the foot. For instance, osteochondritis dissecans and osteomyelitis in the foot and ankle demonstrate the profound utility of these advanced sequences in guiding surgical decision-making and preventing catastrophic structural collapse.



Fig. 2-6 Osteochondritis dissecans of talus in a college football player. A, Coronal T1-weighted image shows an osteochondral fragment in the medial talar dome. Loss of fat signal suggests sclerosis or fibrosis. B, Coronal fat-suppressed, T2-weighted image shows fluid signal between the lesion and host bone, indicating an unstable fragment. C, Coronal fat-suppressed, spoiled gradient-echo technique reveals abnormal decreased signal in overlying articular cartilage, indicating a defect confirmed by arthroscopy.

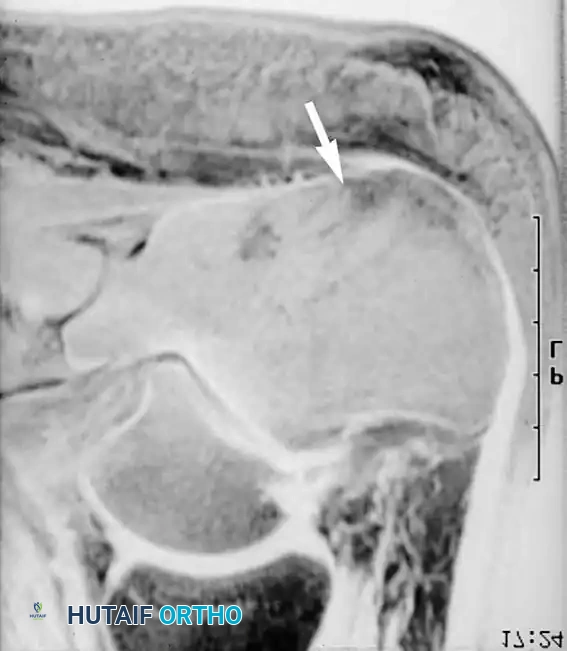
Fig. 2-7 Osteomyelitis in the foot of a diabetic patient. A, Lateral radiograph of the hindfoot reveals no abnormalities. B, Sagittal fat-suppressed, T2-weighted image shows increased signal in calcaneal marrow, indicating osteomyelitis.
Detailed Surgical Anatomy and Biomechanics
Biomechanically, the knee is an inherently unstable modified hinge joint (ginglymus) that relies heavily on its robust soft-tissue envelope—comprising ligaments, menisci, and the joint capsule—for static and dynamic stability. The bony architecture, consisting of the relatively flat tibial plateaus articulating with the convex femoral condyles, provides minimal intrinsic osseous constraint. Therefore, the integrity of the menisci and the cruciate-collateral ligamentous complex is paramount. The menisci are vital for load transmission, shock absorption, joint lubrication, and secondary joint stability. Composed primarily of Type I collagen organized in a highly specific ultrastructure, the menisci feature circumferential fibers that resist hoop stresses and radial tie fibers that prevent longitudinal splitting.
Best evaluated in cross-section on sagittal MRI images, the normal menisci appear as dark, uniformly hypointense triangles in the central portion of the joint and assume a characteristic “bow tie” configuration at the periphery. Regions of increased signal often can be seen within the normally dark fibrocartilage and are classified into three distinct grades. Grade 1 represents globular areas of increased signal, while Grade 2 denotes linear areas of increased signal. Grades 1 and 2 signal changes do not extend to the articular surface, do not represent tears, and correspond to areas of mucoid degeneration that are invisible arthroscopically. Follow-up examinations have not shown a definitive progression from Grade 1/2 to meniscal tears. Conversely, a Grade 3 signal abnormality, which extends to the superior or inferior articular surface, represents a true meniscal tear.
Diagnostic Pitfall: Signal abnormalities seen on only a single MRI slice should not be definitively considered tears unless there is associated anatomical distortion of the meniscus. Elderly patients often exhibit greatly increased intrameniscal signal due to advanced mucoid degeneration that can be easily mistaken for a tear by an inexperienced reader.
The cruciate ligaments are the primary intra-articular stabilizers, dictating the complex roll-and-glide kinematics of the knee. The anterior cruciate ligament (ACL) is the primary restraint to anterior tibial translation and a secondary restraint to internal rotation. It is composed of two functional bundles: the anteromedial (AM) bundle, which is tight in flexion, and the posterolateral (PL) bundle, which is tight in extension. The posterior cruciate ligament (PCL) is the primary restraint to posterior tibial translation and consists of a larger anterolateral (AL) bundle and a smaller posteromedial (PM) bundle. In extension, the normal PCL is a gently curving band of fibrous tissue, appearing as a homogeneously hypointense structure of uniform thickness on sagittal MRI. Discontinuity of the ligament or fluid signal within its substance indicates a macroscopic tear.
The collateral ligaments and the posterolateral corner (PLC) provide essential coronal and rotational stability. In the coronal imaging plane, the medial collateral ligament (MCL) appears as a thin dark band of tissue closely applied to the periphery of the medial meniscus. The superficial MCL is the primary restraint to valgus stress, while the deep MCL provides secondary meniscal stabilization. Injuries of the lateral supporting structures—including the fibular collateral ligament (LCL), the iliotibial band, the biceps femoris tendon, and the popliteus musculotendinous complex—comprise the PLC. MRI depiction of PLC injuries is highly critical, as missed or unaddressed PLC tears are a primary cause of subsequent ACL or PCL reconstruction failure due to unmitigated varus and dial rotational instability.

Fig. 2-8 Meniscal tear. Sagittal proton density–weighted image shows linear increased signal traversing the posterior horn of the medial meniscus, indicating an oblique tear.

Fig. 2-9 Meniscal tear. Sagittal proton density–weighted image reveals a small defect in the free edge of the body of the lateral meniscus, indicating a radial tear.
Exhaustive Indications and Contraindications
Surgical decision-making in knee pathology requires a nuanced integration of clinical examination findings, patient-specific functional demands, and high-resolution MRI data. The indications for operative intervention are rarely absolute and must be weighed against the inherent risks of surgery and the natural history of the specific lesion. For meniscal pathology, the paradigm has dramatically shifted from routine total meniscectomy to aggressive meniscal preservation whenever anatomically and biologically feasible. Partial meniscectomy is strictly indicated for complex, degenerative, or radial tears located exclusively in the avascular (white-white) zone where healing potential is negligible. Conversely, meniscal repair is strongly indicated for longitudinal vertical tears situated in the vascularized (red-red or red-white) zones, particularly in young patients or in conjunction with an ACL reconstruction, which enhances the biological healing milieu via intra-articular hemarthrosis.
The indications for ACL reconstruction are primarily dictated by the patient's desire to return to high-level pivoting, cutting, or jumping sports, or the presence of persistent symptomatic instability with activities of daily living despite rigorous physical therapy. Relative contraindications to acute ACL reconstruction include profound knee stiffness, an active intra-articular infection, or an open physis in a very young patient (which necessitates specialized physeal-sparing or partial transphyseal techniques). For osteochondral defects (OCD), surgical intervention is definitively indicated when MRI demonstrates fluid behind the fragment—a hallmark of mechanical instability—when the articular cartilage is breached, or when prolonged conservative management fails to yield osseous integration.
Contraindications to advanced cartilage restoration procedures, such as autologous chondrocyte implantation (ACI) or osteochondral allograft transplantation, include uncorrected mechanical malalignment (e.g., profound varus or valgus deformity), concurrent unaddressed ligamentous instability, or diffuse "kissing" bipolar osteoarthritic changes. In these scenarios, isolated cartilage procedures are doomed to biomechanical failure. The table below delineates the comprehensive indications and contraindications for common surgical interventions in the knee.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Partial Meniscectomy | Symptomatic avascular zone tears; mechanical locking; failed conservative therapy. | Red-red zone longitudinal tears in young patients; diffuse severe osteoarthritis. | Mild degenerative tears without mechanical symptoms; asymptomatic MRI findings. |
| Meniscal Repair | Red-red / red-white zone tears; root avulsions; bucket-handle tears; concurrent ACL reconstruction. | Complex macerated tears; white-white zone tears; severe generalized osteoarthritis. | Chronic tears (>6 months) with significant tissue retraction; older, low-demand patients. |
| ACL Reconstruction | Symptomatic instability; desire to return to pivoting sports; combined multiligamentous injury. | Active joint infection; profound arthrofibrosis (lack of full extension). | Advanced symptomatic osteoarthritis; sedentary lifestyle; non-compliant patient. |
| OCD Fixation / OATS | Unstable fragments (fluid on MRI); failed conservative management; large focal defects (>2cm²). | Diffuse degenerative joint disease; uncorrected malalignment; active infection. | Asymptomatic stable lesions in skeletally immature patients; bipolar kissing lesions. |
| PLC Reconstruction | Grade III PLC injury with varus/rotational instability; combined with ACL/PCL tears. | Active infection; severe neurovascular compromise precluding safe surgical approach. | Isolated Grade I/II injuries (often heal conservatively); severe medial compartment OA. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative surgical planning relies heavily on defining the exact anatomical extent of disease through precise, protocol-driven imaging. The orthopedic surgeon must not merely read the radiologist's report but must systematically interrogate the MRI sequences. Most examiners prefer to evaluate the menisci on sagittal proton (spin) density–weighted images, which offer superior spatial resolution and contrast between the dark fibrocartilage and the intermediate signal of synovial fluid. To optimize visualization of the cruciate ligaments, sagittal images are prescribed in a plane parallel to the course of the ACL, which is approximately 15 degrees internally rotated relative to the true sagittal plane. Coronal images are indispensable for evaluating the medial and lateral supporting structures, while the patellofemoral joint and its tracking biomechanics are best seen in the axial plane.
Clinical Pearl: When evaluating the ACL, always ensure the sagittal cuts are angled 15 degrees internally. Failure to align the imaging plane with the anatomical axis of the ACL can result in severe volume averaging artifacts, mimicking a partial tear, mucoid degeneration, or a graft failure in the postoperative setting.
Patient positioning and operating room setup are foundational to the success of arthroscopic knee surgery. General or regional anesthesia (spinal or epidural) is administered based on patient comorbidities and anesthesiologist preference. The patient is placed supine on the operating table. A lateral post or a circumferential leg holder is applied to the proximal thigh. The choice between a post and a leg holder is surgeon-dependent; a leg holder allows for excellent valgus stress to open the medial compartment, while a lateral post often facilitates a deeper flexion angle and easier access to the posteromedial and posterolateral compartments. The contralateral leg is placed in a well-padded gynecologic stirrup to prevent deep vein thrombosis and to provide the surgeon with unencumbered access to the operative knee.
A pneumatic tourniquet is routinely placed proximally on the operative thigh. However, in modern practice, it is often left uninflated unless intra-articular visualization is severely compromised by bleeding that cannot be controlled with epinephrine-infused irrigation fluid and radiofrequency ablation. Avoiding routine tourniquet inflation significantly reduces postoperative quadriceps inhibition, tourniquet site pain, and the risk of venous thromboembolism. Prior to prepping and draping, a meticulous examination under anesthesia (EUA) is performed to document the exact degree of laxity (Lachman, pivot shift, varus/valgus stress at 0 and 30 degrees, and dial test) without the confounding variable of patient guarding.


Fig. 2-14 Acute ACL tear. A, Conventional proton density–weighted sagittal image shows abnormal, more horizontal orientation of the distal portion of the torn ACL. B, T2-weighted image at the same location displays fluid at the site of the avulsed femoral attachment.

Fig. 2-15/16 Coronal/Sagittal imaging demonstrating cruciate and collateral ligamentous integrity, essential for preoperative multiligamentous planning.
Step-by-Step Surgical Approach and Fixation Technique
The arthroscopic approach begins with the establishment of standard viewing and working portals. The anterolateral (AL) portal is the primary viewing portal, established adjacent to the lateral border of the patellar tendon, approximately 1 cm above the joint line. The anteromedial (AM) portal serves as the primary working portal and must be established under direct intra-articular visualization using a spinal needle to ensure optimal trajectory toward the pathology, typically adjacent to the medial border of the patellar tendon. Accessory portals, such as the superolateral portal for outflow or the posteromedial/posterolateral portals for posterior horn meniscal repairs and PCL reconstructions, are established as dictated by the specific pathology.
For meniscal pathology, the surgical technique is dictated by the tear pattern. Partial meniscectomy aims to resect unstable fragments while preserving a stable, contoured peripheral rim. Meniscal repair, conversely, is a technically demanding procedure requiring meticulous biological preparation of the tear site using a rasp or motorized shaver to stimulate bleeding and subsequent fibrovascular healing. The Inside-Out Technique remains the gold standard for body and posterior horn tears. Long, flexible needles are passed from inside the joint, capturing the torn meniscus, and exiting through a protective posterior incision where the sutures are tied directly over the joint capsule. The All-Inside Technique utilizes specialized, low-profile deployment devices (e.g., FasT-Fix) for posterior horn tears, delivering anchors and pre-tied sliding knots entirely arthroscopically, thereby avoiding the morbidity of a posterior incision. The Outside-In Technique is particularly ideal for anterior horn tears, where needles are passed from the skin into the joint.
Surgical Warning: When performing an inside-out repair of the medial meniscus, the saphenous nerve and its infrapatellar branch are at extremely high risk during the posterior approach. When repairing the lateral meniscus, the common peroneal nerve must be rigorously protected via careful retractor placement anterior to the lateral gastrocnemius head.
In the surgical management of the ACL, anatomical graft placement is the singular most critical factor for success. Graft options include Bone-Patellar Tendon-Bone (BTB) autograft, Hamstring (Gracilis/Semitendinosus) autograft, Quadriceps tendon autograft, or various allografts. Tunnel preparation has evolved significantly; the femoral tunnel is now predominantly drilled via an independent anteromedial portal rather than transtibially. This allows for anatomical placement in the native ACL footprint—posterior and proximal in the intercondylar notch—which is critical for restoring rotational stability and eliminating the pivot shift. The tibial tunnel is drilled using a specialized guide set at approximately 55 degrees, exiting at the native ACL footprint anterior to the PCL and posterior to the anterior horn of the lateral meniscus. Fixation is achieved via interference screws (titanium or biocomposite) for bone plugs, or suspensory cortical buttons for soft-tissue grafts, ensuring rigid initial fixation to allow for aggressive early rehabilitation.

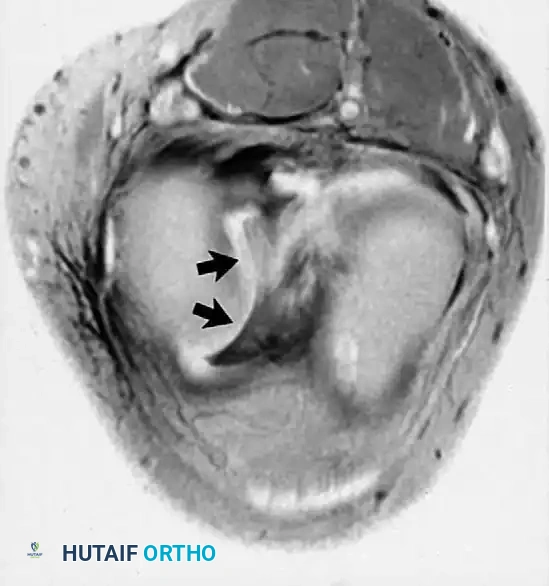
Fig. 2-11 Bucket-handle tear of medial meniscus. Coronal (A) and axial (B) fat-suppressed, proton density–weighted images show a centrally displaced portion of the medial meniscus.

Fig. 2-12 Inferiorly displaced medial meniscal fragment. Fat-suppressed, proton density–weighted image shows a portion of the medial meniscus displaced inferiorly and deep to the medial collateral ligament.
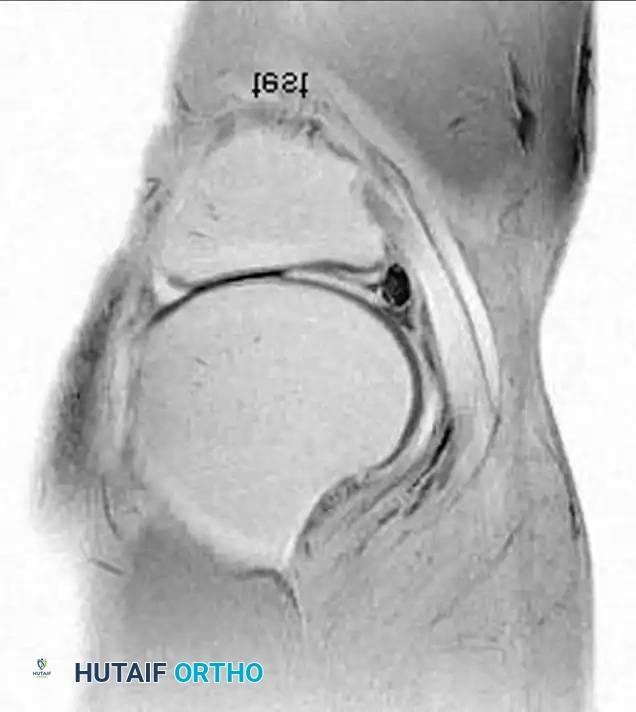
Fig. 2-10 Meniscal cyst. Coronal fat-suppressed, proton density–weighted image of the knee shows a large hyperintense meniscal cyst adjacent to the medial meniscus. An associated tear is present in the inferior articular surface.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced preoperative imaging, complications following arthroscopic knee surgery and ligamentous reconstruction do occur. Intraoperative complications frequently involve iatrogenic neurovascular injury, particularly during inside-out meniscal repairs or posteromedial portal placement. The popliteal artery is at risk during posterior capsular work and tibial tunnel drilling if the posterior cortex is breached without adequate protection. Postoperatively, arthrofibrosis represents one of the most debilitating complications, characterized by a profound loss of extension and flexion, often necessitating aggressive physical therapy, oral corticosteroids, or eventual arthroscopic lysis of adhesions and manipulation under anesthesia.
Infection, though relatively rare in elective arthroscopy (incidence <1%), is a catastrophic complication when it occurs following ACL reconstruction or meniscal repair. Septic arthritis presents with severe pain, swelling, and elevated inflammatory markers (CRP, ESR). Immediate management involves emergent arthroscopic irrigation and debridement, retention of the graft if it remains structurally sound and the infection is caught early, and prolonged culture-directed intravenous antibiotic therapy. Graft failure in ACL reconstruction occurs in approximately 5-10% of cases, stemming from technical errors (non-anatomical tunnel placement), biological failure of incorporation, or recurrent high-energy trauma.
Salvage management for failed knee procedures requires a comprehensive diagnostic workup, often including computed tomography (CT) to assess tunnel widening and precise bony anatomy. Revision ACL reconstruction may necessitate a two-stage approach with initial bone grafting of widened tunnels followed by definitive reconstruction months later. For patients with failed meniscal repairs or post-meniscectomy syndrome leading to rapid unicompartmental degeneration, meniscal allograft transplantation (MAT) combined with corrective osteotomy (e.g., high tibial osteotomy for varus malalignment) serves as a critical salvage pathway to delay the need for arthroplasty in the young, active patient.
| Complication | Estimated Incidence | Primary Etiology / Risk Factor | Salvage / Management Strategy |
|---|---|---|---|
| Arthrofibrosis | 3 - 10% | Surgery in acute inflamed phase; poor early ROM rehab. | Aggressive PT; Corticosteroids; Arthroscopic lysis of adhesions & MUA. |
| Septic Arthritis | 0.5 - 1% | Contamination; prolonged operative time; allograft use (rare). | Emergent arthroscopic I&D; graft retention if early; IV antibiotics. |
| ACL Graft Failure | 5 - 10% | Non-anatomical tunnel placement; missed PLC injury; early return to sport. | Revision ACLR (single vs. two-stage); concurrent PLC reconstruction. |
| Iatrogenic Nerve Injury | 1 - 2% | Inside-out meniscal repair; posteromedial portal placement. | Observation for neuropraxia; surgical exploration for sharp transection. |
| DVT / PE | 1 - 3% | Tourniquet use; prolonged immobilization; hypercoagulable state. | Chemical anticoagulation (LMWH, DOACs); early mobilization protocols. |
Phased Post-Operative Rehabilitation Protocols
The success of any advanced surgical intervention in the knee is inextricably linked to the execution of a meticulously designed, biologically respectful, phased postoperative rehabilitation protocol. Rehabilitation is not merely an afterthought; it is an active, dynamic process that must balance the mechanical protection of the healing tissues with the prevention of joint stiffness and muscular atrophy. Protocols are generally divided into four distinct phases, customized to the specific procedure performed, the fixation strength achieved, and the biological timeline of tissue healing.
Phase I: Immediate Postoperative Phase (Weeks 0-4)
The primary goals of Phase I are the protection of the surgical repair, the control of postoperative inflammation and effusion, the restoration of full, symmetric knee extension, and the re-establishment of quadriceps control. For isolated ACL reconstructions, immediate weight-bearing as tolerated in a hinged knee brace locked in extension is generally permitted. Conversely, for meniscal repairs or osteochondral procedures, weight-bearing is strictly limited (touch-down or non-weight-bearing) to prevent deleterious shear forces across the healing site. Range of motion (ROM) exercises emphasize prone hangs and heel props to achieve terminal extension, while flexion is progressively advanced. Neuromuscular electrical stimulation (NMES) combined with isometric quadriceps sets is critical to overcome arthrogenic muscle inhibition.
Phase II: Intermediate Rehabilitation Phase (Weeks 4-12)
As the biological scaffold begins early incorporation and the inflammatory phase subsides, Phase II focuses on progressing to full weight-bearing, restoring normal gait mechanics, and achieving full, painless ROM. Strengthening exercises transition from closed kinetic chain (CKC) exercises, such as mini-squats and leg presses, to carefully monitored open kinetic chain (OKC) exercises. For ACL grafts, particularly during the "ligamentization" phase (weeks 6-12) where the graft is biologically at its weakest, excessive anterior tibial translation forces must be avoided. Proprioceptive training is initiated using balance boards and unstable surfaces to retrain the mechanoreceptors disrupted during the injury and surgical approach.
Phase III: Advanced Strengthening and Agility (Months 3-6)
Phase III bridges the gap between basic functional recovery and the demands of athletic activity. The emphasis shifts heavily toward dynamic stabilization, plyometrics, and sport-specific agility drills. Isokinetic testing is frequently employed to objectively quantify quadriceps and hamstring strength deficits compared to the contralateral uninjured limb. Straight-line running is typically initiated between months 3 and 4, provided the patient demonstrates a quiescent joint (no effusion), full ROM, and at least 70-80% limb symmetry index (LSI) on strength testing. Cutting, pivoting, and deceleration drills are introduced late in this phase under the strict supervision of a physical therapist or athletic trainer.
Phase IV: Return to Sport and Maintenance (Months 6-12+)
The final phase is the most critical and often the most psychologically challenging for the athlete. Return to unrestricted play is not dictated by time alone but by the successful completion of a battery of rigorous functional tests. The criteria for return to sport typically require an LSI of >90% on isokinetic strength testing and a suite of functional hop tests (single hop, triple hop, crossover hop, and 6-meter timed hop). Furthermore, qualitative assessment of movement mechanics (e.g., avoiding dynamic valgus upon landing) is paramount to prevent secondary injuries. The patient is transitioned to a maintenance program designed to sustain strength, flexibility, and neuromuscular control indefinitely.

Fig. 2-13 Discoid meniscus in a 3-year-old boy. A, Sagittal proton density–weighted image reveals an abnormally thick lateral meniscus. B, Coronal fat-suppressed, proton density–weighted image shows extension of the discoid meniscus centrally into the weight-bearing portion of the lateral compartment.
Summary of Landmark Literature and Clinical Guidelines
The contemporary surgical management of knee pathologies is deeply rooted in a robust foundation of evidence-based medicine, guided by landmark prospective cohort studies, randomized controlled trials, and consensus statements from major orthopedic societies. The Multicenter Orthopaedic Outcomes Network (MOON) cohort has been instrumental in defining the predictors of success and failure in ACL reconstruction. Their extensive longitudinal data have unequivocally demonstrated that anatomical graft placement, the use of autograft tissue in young active patients, and the concurrent treatment of meniscal and chondral pathology are critical determinants of long-term patient-reported outcomes and the mitigation of post-traumatic osteoarthritis.
Similarly, the Multicenter ACL Revision Study (MARS) group has provided invaluable insights into the complexities of revision ACL surgery, highlighting that clinical outcomes following revision are universally inferior to primary reconstructions. The MARS data emphasize the necessity of identifying the specific etiology of primary failure—whether it be technical error, biological failure, or missed concomitant ligamentous injury (such as a PLC tear)—to optimize the surgical strategy for the revision setting. These findings have catalyzed a paradigm shift toward more comprehensive preoperative imaging and meticulous intraoperative anatomical precision.
Current clinical practice guidelines published by the American Academy of Orthopaedic Surgeons (AAOS) and the American Orthopaedic Society for Sports Medicine (AOSSM) strongly advocate for joint preservation strategies. The guidelines emphasize that meniscal repair should be attempted for all repairable tears, particularly in the setting of concurrent ACL reconstruction, given the synergistic effect on healing rates. Furthermore, the literature strongly supports the use of advanced cartilage restoration techniques (OATS, ACI) for symptomatic, full-thickness osteochondral defects that have failed conservative management, provided the mechanical alignment and ligamentous stability of the knee are concurrently addressed. As advanced MRI diagnostics continue to evolve—with the advent of quantitative compositional mapping (T2 mapping, dGEMRIC) to assess early biochemical cartilage degradation—the surgical indications and timing of intervention will undoubtedly become even more precise,
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding knee