Advanced MRI Evaluation of the Hip and Knee: A Comprehensive Surgical Guide

Key Takeaway
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating complex musculoskeletal pathologies of the hip and knee. This comprehensive guide details the radiological interpretation and surgical management of osteonecrosis, transient osteoporosis, occult fractures, and chondral defects. By integrating advanced imaging with evidence-based operative protocols, orthopaedic surgeons can optimize patient outcomes through precise preoperative planning and targeted interventions.
Principles of Advanced Magnetic Resonance Imaging in Orthopaedics
Magnetic Resonance Imaging (MRI) has revolutionized the diagnostic algorithm for complex musculoskeletal pathologies of the lower extremity. With its unsurpassed soft-tissue contrast and ability to image bone marrow at a cellular level, MRI detects a broad spectrum of pathological conditions long before they become apparent on conventional radiography.
For the orthopaedic surgeon, understanding coil selection and sequence parameters is critical for accurate preoperative planning. Examination of the hips can be performed with the main magnetic coil (body coil). This technique allows for the simultaneous evaluation of both hips, which is paramount in patients presenting with potentially bilateral pathological processes, such as osteonecrosis (avascular necrosis) or systemic inflammatory arthropathies.
If unilateral evaluation is sufficient, improved spatial resolution is obtained with the use of dedicated surface coils. When available, torso coils featuring a phased-array design represent the gold standard, combining the improved signal-to-noise ratio required for high-resolution images with a large field-of-view coverage. Standard protocols typically include spin-echo sequences performed in the axial and coronal planes. Sagittal images are mandatory when investigating osteonecrosis to accurately quantify the anterior-posterior extent of the necrotic segment, which directly dictates surgical decision-making.
Clinical Pearl: Always correlate MRI findings with weight-bearing radiographs. MRI is highly sensitive for marrow edema, but plain films remain essential for assessing joint space narrowing, dynamic instability, and overall mechanical alignment.
Soft Tissue and Articular Pathologies of the Knee
While the primary focus of pelvic imaging is the hip, lower extremity MRI frequently captures concurrent knee pathologies that require distinct surgical considerations. MRI is exceptionally well-suited for evaluating synovial pathological conditions, osseous contusions, and occult ligamentous injuries.
Popliteal Fossa Cysts (Baker's Cysts)
Popliteal cysts are the most common synovial cysts of the knee. They arise from fluid distension of the gastrocnemio-semimembranosus bursa, which communicates with the knee joint via a slit-like opening in the posteromedial capsule.

Fig. 2-17 Popliteal fossa cyst. Axial proton density–weighted image shows hyperintense fluid extending from the knee joint into the popliteal fossa between the semimembranosus tendon (straight arrow) and medial gastrocnemius tendon (curved arrow).
Surgical Implications:
A Baker's cyst is rarely an isolated pathology; it is almost universally secondary to an intra-articular derangement, most commonly a medial meniscal tear or advanced osteoarthritis. Surgical excision of the cyst itself is rarely indicated and carries a high recurrence rate. Instead, operative management should focus on addressing the primary intra-articular pathology via knee arthroscopy. Once the meniscal tear is resected or repaired, the one-way valve mechanism is decompressed, and the cyst typically resolves spontaneously.
Patellofemoral Instability and Dislocation
Acute lateral patellar dislocation results in a highly specific pattern of osseous contusion (bone bruising) due to the impaction of the medial patellar facet against the lateral femoral condyle as the patella relocates.
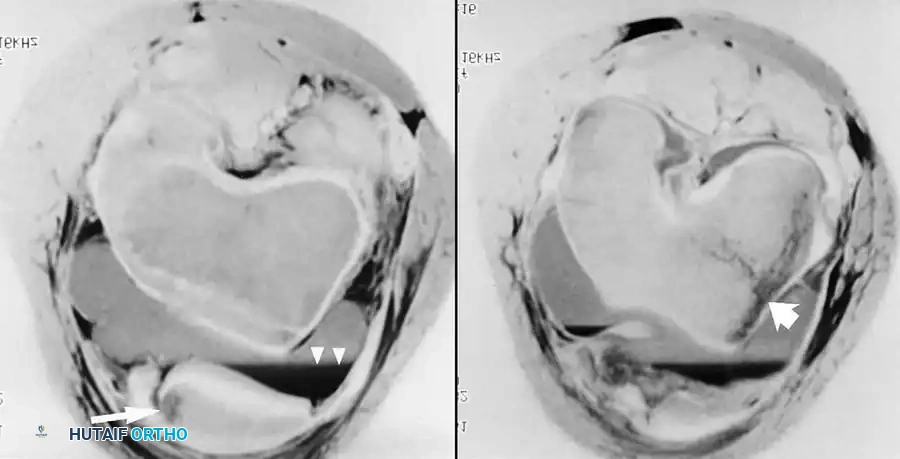
Fig. 2-18 Patellar dislocation. Axial fat-suppressed, proton density–weighted images through the patellofemoral joint show regions of increased signal, representing marrow edema beneath the medial facet of the patella and in the lateral aspect of the lateral femoral condyle. Note the hematocrit level in the joint effusion.
Biomechanics and Surgical Management:
The Medial Patellofemoral Ligament (MPFL) is the primary restraint to lateral patellar translation at early flexion angles (0° to 30°). In the setting of an acute dislocation with a large osteochondral fracture or recurrent instability, surgical intervention is warranted.
* Positioning: Supine with a lateral post to allow free knee flexion.
* Procedure: MPFL reconstruction using an autograft (e.g., gracilis) or allograft. The femoral attachment is localized fluoroscopically at Schöttle's point (anterior to the posterior femoral cortex line, proximal to the Blumensaat line, and distal to the medial epicondyle).
* Postoperative Protocol: Hinged knee brace locked in extension for ambulation, with progressive range of motion (ROM) initiated immediately to prevent arthrofibrosis.
Chondral Lesions
Focal chondral defects are accurately sized and graded using fat-suppressed proton density or T2-weighted mapping sequences.

Fig. 2-21 Chondral lesion. Fat-suppressed proton density–weighted sagittal image of the knee reveals a small, well-defined, fluid-filled, full-thickness defect in the articular cartilage of the posteromedial femoral condyle.
Surgical Management:
Treatment depends on the lesion size and patient age.
* < 2 cm²: Microfracture or marrow stimulation techniques.
* 2 - 4 cm²: Osteochondral Autograft Transfer System (OATS) or mosaicplasty.
* > 4 cm²: Matrix-Induced Autologous Chondrocyte Implantation (MACI) or osteochondral allograft.
Pediatric Knee Trauma and Physeal Complications
Direct coronal and sagittal MRI is invaluable in assessing complications of physeal injuries in the pediatric population, particularly when plain radiographs are equivocal.
Occult Salter-Harris Fractures
Fig. 2-19 Occult Salter II fracture of the distal femur in a 14-year-old boy. Coronal T1-weighted image reveals ill-defined reduced signal in the medial distal femoral metaphysis. Fat-suppressed, T2-weighted image shows an irregular hypointense fracture surrounded by hyperintense marrow edema extending along the lateral physis.
Surgical Management:
Undisplaced Salter-Harris II fractures can often be managed with cast immobilization. However, if displacement occurs, closed reduction and percutaneous pinning (CRPP) or cannulated screw fixation parallel to the physis is required to prevent growth arrest.
Physeal Bars
A severe complication of physeal trauma is the formation of an osseous bridge (physeal bar) across the growth plate, leading to angular deformity or limb length discrepancy.

Fig. 2-20 Physeal bar in a 12-year-old boy. Gradient-echo sagittal image of the knee shows interruption of the posterior extent of the distal femoral physis. An osseous bridge has resulted in posterior angulation of the articular surface.
Surgical Management:
If the physeal bar involves less than 50% of the cross-sectional area of the physis and the child has at least 2 years of growth remaining, surgical resection of the bar with interposition of a fat graft or cranioplast is indicated. If the bar exceeds 50%, a completion epiphysiodesis combined with a corrective osteotomy is the treatment of choice.
Osteonecrosis (Avascular Necrosis) of the Femoral Head
The most frequent indication for hip MRI is the evaluation of osteonecrosis. Early diagnosis is imperative because joint-preserving operative treatments are highly time-sensitive. While initial radiographs are usually normal (Ficat Stage I), MRI is the most sensitive modality for detecting early ischemia and delineating the extent of marrow necrosis.
Radiological Interpretation
The percentage of involvement of the weight-bearing cortex of the femoral head, as defined by MRI, is the most reliable predictor of subchondral collapse and the success of joint-preserving surgery.
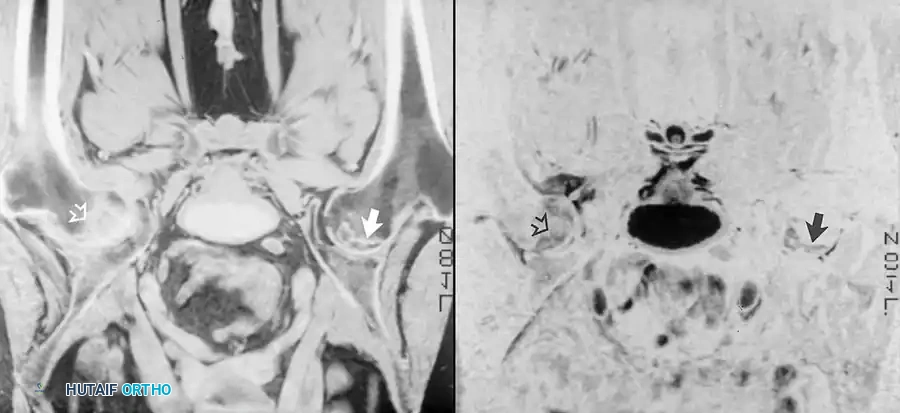
Fig. 2-22 Osteonecrosis of the femoral head. T1-weighted images show a geographical region of decreased marrow signal within the normally bright fat of the femoral head.
On T1-weighted images, the classic appearance is a geographical region of decreased marrow signal within the normally bright fat of the femoral head. This area is frequently surrounded by a low-signal band representing ischemic, sclerotic bone.
On T2-weighted images, a second inner band of bright signal is revealed. This resulting appearance is termed the "double-line" sign, which is pathognomonic for osteonecrosis. The central necrotic bone exhibits various signal patterns depending on the degree of hemorrhage, fat necrosis, edema, or fibrosis. In late stages, flattening of the femoral head (crescent sign), cartilage loss, and joint effusion become apparent.
Surgical Management Protocols
1. Core Decompression (Pre-Collapse: Ficat Stages I & IIA)
* Indications: Symptomatic AVN prior to subchondral collapse, ideally with < 30% involvement of the weight-bearing surface.
* Positioning: Supine on a fracture table.
* Technique: Under fluoroscopic guidance, a guide pin is advanced from the lateral subtrochanteric cortex into the necrotic lesion in the anterosuperior femoral head. A reamer (typically 8-10 mm) is passed over the pin to decompress the intraosseous pressure and stimulate angiogenesis. Biologic adjuvants (e.g., bone marrow aspirate concentrate) may be injected into the tract.
2. Free Vascularized Fibular Grafting
* Indications: Young patients with larger pre-collapse lesions.
* Technique: Involves harvesting the fibula with its vascular pedicle (peroneal artery) and anastomosing it to the lateral femoral circumflex artery, providing structural support and a live blood supply to the necrotic head.
3. Total Hip Arthroplasty (THA) (Post-Collapse: Ficat Stages III & IV)
* Indications: Subchondral collapse, secondary osteoarthritis, or failed core decompression.
* Technique: Standard THA utilizing uncemented components. Care must be taken to ensure adequate fixation in the proximal femur, as the bone quality may be compromised.
Surgical Warning: Core decompression in lesions occupying > 50% of the weight-bearing surface carries a high failure rate and an increased risk of iatrogenic subtrochanteric fracture. Proceed with caution and consider prophylactic restricted weight-bearing postoperatively.
Transient Osteoporosis of the Hip (TOH)
Transient osteoporosis of the hip is a self-limited condition characterized by sudden onset hip pain and profound bone marrow edema. Initially described in pregnant women during their third trimester, it is now most commonly diagnosed in middle-aged men.
Pathophysiology and Imaging
The etiology remains uncertain, though it is hypothesized to be related to complex regional pain syndrome (CRPS) or regional migratory osteoporosis. Initial radiographs may be normal or reveal diffuse osteopenia of the femoral head with strict preservation of the joint space.
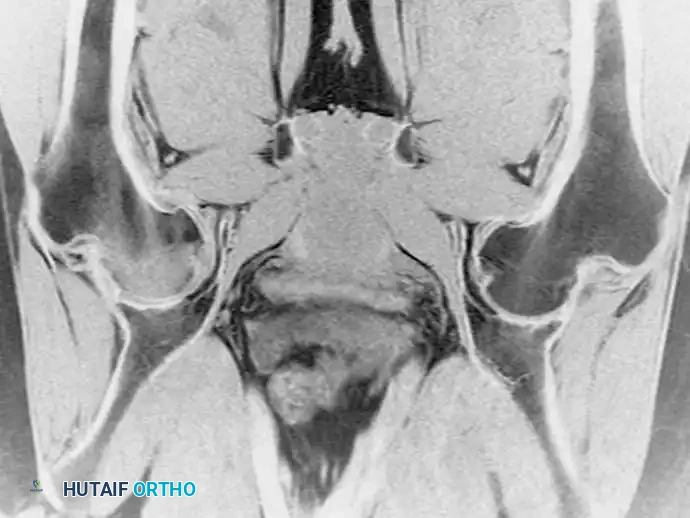
Fig. 2-23A Transient osteoporosis of the hip in a 30-year-old man. Coronal T1-weighted image reveals diminished signal intensity within the right femoral head and neck.
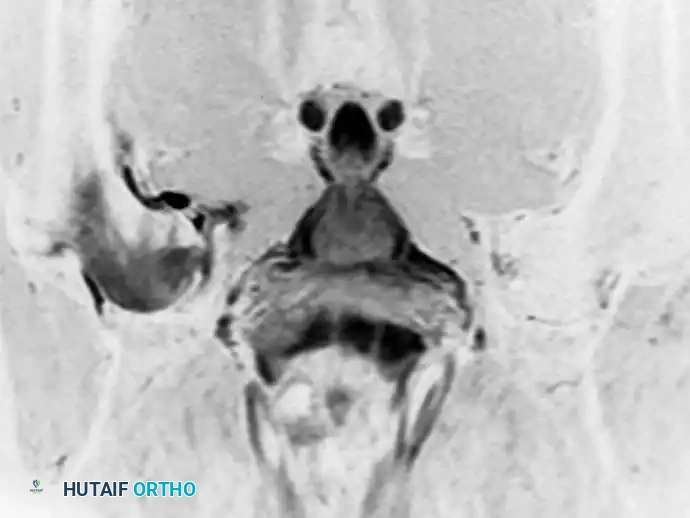
Fig. 2-23B Coronal inversion recovery sequence shows hyperintense bone marrow edema in a more diffuse pattern than seen in osteonecrosis.
The MRI appearance is defined by diffuse edema in the femoral head extending down into the intertrochanteric region. Crucially, the focal geographic signal abnormalities and the "double-line" sign seen in osteonecrosis are absent. T1-weighted sequences depict diffuse edema as a relative low signal against background fatty marrow. On T2-weighted and STIR sequences, the edema becomes intensely hyperintense—a presentation termed the bone marrow edema pattern.
Clinical Management
Rarely, a tiny focal linear lesion in the subcortical marrow indicates an insufficiency fracture within the demineralized bone. If initial radiographs are normal, repeat films at 6 to 8 weeks will show characteristic osteopenia.
Treatment is strictly non-operative. Management consists of protected weight-bearing (crutches) to prevent insufficiency fractures, analgesia, and occasionally the off-label use of bisphosphonates to reduce osteoclastic activity. The condition generally resolves spontaneously within 6 to 12 months, with complete normalization of both clinical symptoms and MRI appearance.
Occult Proximal Femur Fractures
In the geriatric population, patients frequently present with hip pain and an inability to bear weight following a low-energy fall. When initial radiographs are negative or equivocal, MRI is the diagnostic modality of choice.
Diagnostic Superiority of MRI
While bone scintigraphy (bone scanning) was historically used, it can yield false-negative results in elderly patients during the first 48 to 72 hours post-injury due to delayed osteoblastic response. MRI abnormalities, however, are apparent immediately.
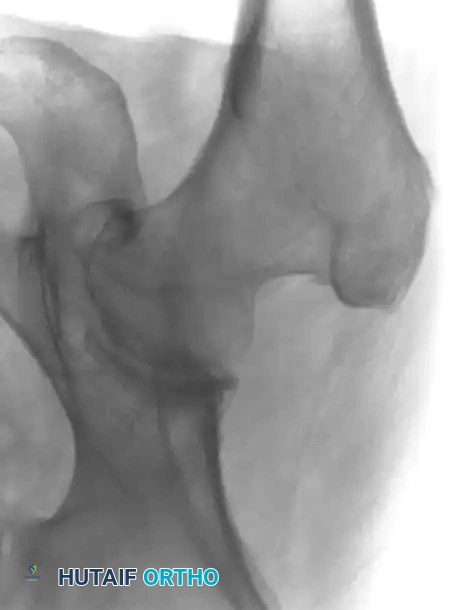
Fig. 2-24A Occult fracture evaluation.
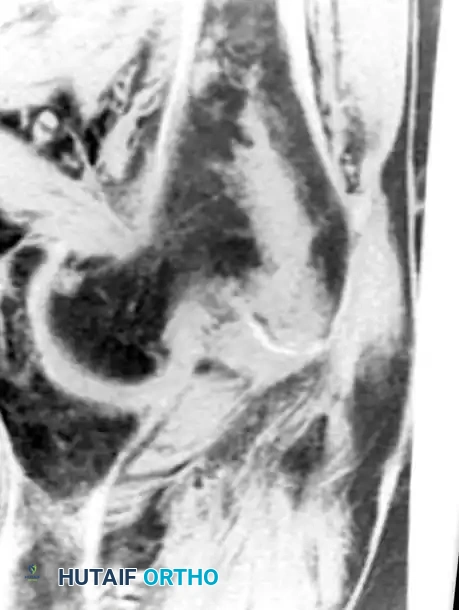
Fig. 2-24B Linear areas of low signal are easily seen in the fatty marrow on T1-weighted images.
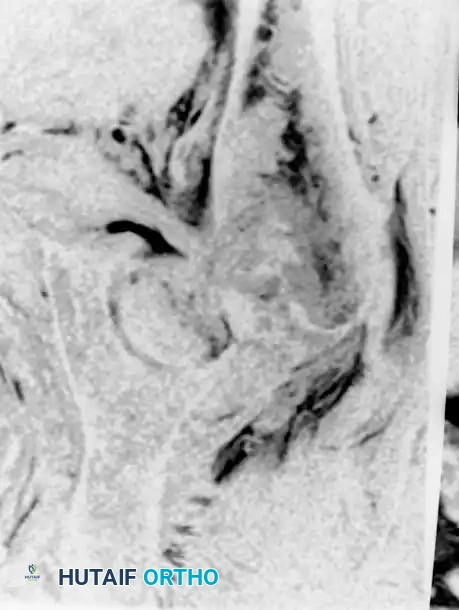
Fig. 2-24C Surrounding edema is clearly visualized with T2-weighted images, confirming the fracture line.
Surgical Decision Making
The anatomical information provided by MRI directly dictates the surgical fixation strategy:
* Greater Trochanteric Fractures: If the fracture is strictly confined to the greater trochanter without extension into the intertrochanteric line, conservative management with protected weight-bearing is appropriate.
* Incomplete/Non-displaced Femoral Neck Fractures: Treated urgently with in-situ fixation using three cannulated cancellous screws placed in an inverted triangle configuration to prevent displacement.
* Occult Intertrochanteric Fractures: Require stabilization with a sliding hip screw (SHS) or a cephalomedullary nail to allow early mobilization and prevent the catastrophic complications of prolonged bed rest.
Acetabular Labral Tears and MR Arthrography
The evaluation of the acetabular labrum has evolved significantly. Early reviews of conventional MRI accuracy for labral pathology were disappointing due to large field-of-view images lacking adequate resolution. Today, MR Arthrography (MRA) of the hip is the gold standard.
Diagnostic Technique
The advent of MRA has greatly improved the visualization of the cartilaginous labrum. The procedure involves the fluoroscopically guided intra-articular injection of dilute gadolinium. The fluid distends the joint capsule, outlining labral tears, chondral delamination, and ligamentum teres injuries.
**Clinical
