Advanced MRI and Surgical Management of Elbow Pathologies and Musculoskeletal Tumors
Key Takeaway
Magnetic Resonance Imaging (MRI) is paramount in modern orthopedic surgery, offering unparalleled soft-tissue contrast for evaluating elbow pathologies and musculoskeletal tumors. This guide details the diagnostic imaging, biomechanics, and surgical management of distal biceps ruptures, triceps avulsions, and ulnar collateral ligament tears. Furthermore, it provides an evidence-based framework for the oncological assessment of bone and soft-tissue neoplasms, emphasizing the critical role of advanced imaging in surgical planning and limb salvage.
ADVANCED IMAGING AND SURGICAL MANAGEMENT OF THE ELBOW
In the comprehensive evaluation of the elbow, Magnetic Resonance Imaging (MRI) serves as an indispensable adjunct to clinical examination and standard radiography. It is particularly efficacious in the assessment of the biceps and triceps tendons, as well as the capsuloligamentous stabilizers. Although complete ruptures of these tendinous structures are frequently clinically apparent—often presenting with palpable defects, ecchymosis, and profound weakness—MRI remains critical for precise surgical planning. It delineates the degree of tendon retraction, the quality of the remaining tendon stump, and the presence of concomitant pathology. Furthermore, MRI is the gold standard for detecting partial tears, which may present insidiously and confound clinical diagnosis.
Distal Biceps Tendon Rupture
The distal biceps tendon is the primary supinator of the forearm and a secondary flexor of the elbow. Ruptures typically occur in active middle-aged males following an eccentric load applied to a flexed elbow.
Imaging Characteristics:
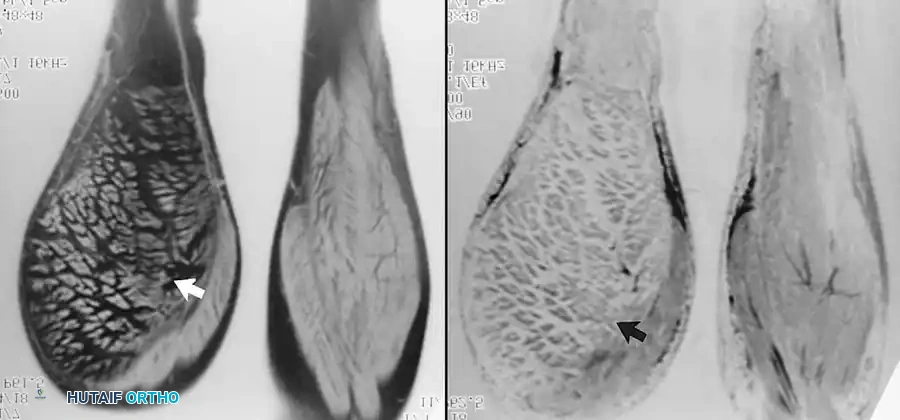
On MRI, a complete rupture is characterized by an abrupt discontinuity of the low-signal tendon fibers, often accompanied by proximal retraction and surrounding fluid or hemorrhage. Sagittal and axial fluid-sensitive sequences (e.g., T2-weighted fat-suppressed or STIR) are optimal for visualizing the retracted stump and the empty radial tuberosity footprint.
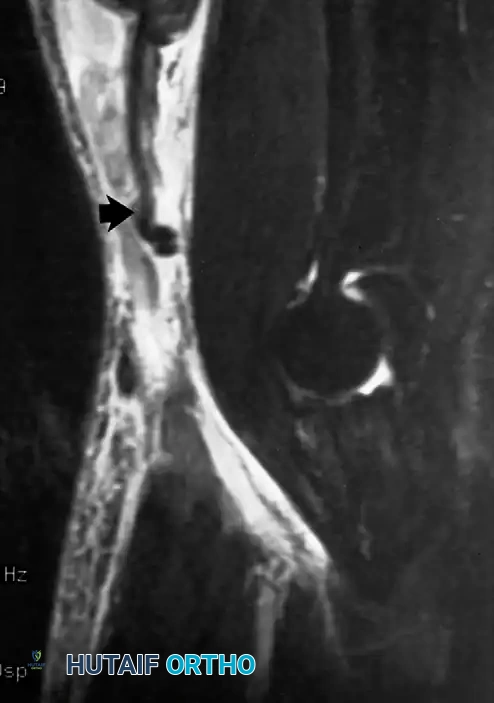
Fig. 2-37 Rupture of distal biceps tendon. Sagittal inversion recovery image of elbow shows ruptured distal biceps tendon. Proximal tendon (arrow) has retracted several centimeters, and edema is present in tissues anterior to brachialis muscle.
Surgical Management:
Early anatomic repair to the radial tuberosity is recommended to restore supination strength and endurance.
- Positioning: Supine with the arm extended on a hand table.
- Approach: A single anterior transverse incision in the antecubital crease or a dual-incision (modified Boyd-Anderson) approach may be utilized. The single-incision technique minimizes heterotopic ossification risks but requires careful protection of the lateral antebrachial cutaneous nerve (LABCN) and the posterior interosseous nerve (PIN).
- Deep Dissection: The lacertus fibrosus is often torn but should be identified. The retracted tendon is retrieved, and the degenerated distal stump is debrided. The radial tuberosity is exposed by maximally supinating the forearm.
- Fixation: Biomechanical studies favor cortical button fixation, often augmented with an interference screw or suture anchor, providing superior load-to-failure strength.
- Postoperative Protocol: The elbow is immobilized in 90 degrees of flexion and neutral rotation for 1-2 weeks, followed by a hinged brace allowing progressive extension. Strengthening commences at 8-12 weeks.
Surgical Warning: When exposing the radial tuberosity via a single anterior approach, the forearm must be maintained in maximal supination to protect the PIN, which wraps around the radial neck within the supinator muscle.
Triceps Tendon Avulsion
Triceps ruptures are exceedingly rare, accounting for less than 1% of all tendon ruptures. They typically result from a deceleration force during elbow extension or a direct blow to the posterior elbow. Systemic risk factors include anabolic steroid use, chronic kidney disease, and fluoroquinolone administration.
Imaging Characteristics:
MRI confirms the diagnosis, showing discontinuity of the triceps tendon at or near its insertion on the olecranon. Fluid fills the gap between the tendon and the bone.

Fig. 2-38 Avulsion of triceps tendon. A, Sagittal fat-suppressed, proton density–weighted image of elbow shows avulsed triceps tendon (long arrow) retracted proximally from olecranon (thick arrow). B, Sagittal fat-suppressed, T2-weighted image shows hyperintense fluid (arrows) in gap between bone and detached tendon.
Surgical Management:
* Positioning: Lateral decubitus or prone, with the arm draped over a bolster to allow 120 degrees of elbow flexion.
* Approach: A direct posterior longitudinal incision, curving slightly lateral to the tip of the olecranon to avoid the bursa.
* Fixation: The tendon is mobilized and secured using heavy non-absorbable sutures in a Krackow fashion. Fixation to the olecranon is achieved via transosseous cruciate tunnels or suture anchors. The repair is tensioned with the elbow in 30-45 degrees of flexion.
* Postoperative Protocol: Immobilization in 30 degrees of flexion for 2 weeks, followed by progressive passive range of motion. Active extension against resistance is delayed until 12 weeks.
Ulnar Collateral Ligament (UCL) Injuries
The anterior bundle of the UCL is the primary restraint to valgus stress at the elbow between 30 and 120 degrees of flexion. Injury is endemic among overhead throwing athletes due to repetitive valgus extension overload.
Imaging Characteristics:
Conventional MRI and MRI arthrography (MRA) play a crucial role in evaluating medial instability. The normal UCL appears as a linear, taut, hypointense structure extending from the medial epicondyle to the sublime tubercle of the ulna. In acute ruptures, fluid is seen within and around the disrupted ligament. MRA is particularly sensitive for partial-thickness undersurface tears, demonstrating contrast tracking deep to the ulnar attachment (the "T-sign").

Fig. 2-39 Partial ulnar collateral ligament tear at MRI arthrography of elbow. Coronal fat-suppressed, T1-weighted image reveals contrast tracking deep to ulnar attachment of ulnar collateral ligament (arrow).
Surgical Management (UCL Reconstruction):
* Indications: High-demand throwing athletes with symptomatic valgus instability failing non-operative management (rest, mechanics modification, PRP injections).
* Graft Choice: Ipsilateral palmaris longus (most common), gracilis, or plantaris autograft.
* Approach: Medial elbow incision centered over the medial epicondyle. The ulnar nerve is identified and protected; routine transposition is reserved for patients with preoperative ulnar neuritis.
* Technique: The flexor-pronator mass is split longitudinally. The native ligament is incised to expose the joint. Tunnels are drilled at the sublime tubercle and the medial epicondyle isometric point. The graft is passed using either a figure-of-eight (Jobe) or docking technique. The docking technique is currently favored for its superior tensioning capabilities and reduced bone removal.
* Postoperative Protocol: Splinting at 90 degrees for 1 week. A hinged brace is then applied. A structured throwing program begins at 4-5 months, with return to competitive pitching typically requiring 12-18 months.
Clinical Pearl: The "milking maneuver" and the moving valgus stress test are highly sensitive clinical examinations for UCL insufficiency. Always correlate these findings with MRA to differentiate between adaptive elongation and true structural failure.
WRIST AND HAND PATHOLOGIES: MRI CORRELATES
While the primary focus remains on the elbow and oncology, MRI is equally transformative in the distal upper extremity, particularly for avascular necrosis and tendon ruptures.
Osteonecrosis of the Carpus
Kienböck disease (osteonecrosis of the lunate) and scaphoid osteonecrosis (often post-traumatic) are exquisitely sensitive to MRI evaluation. Loss of the normal high-signal marrow fat on T1-weighted images is the hallmark of ischemia and subsequent necrosis.

Fig. 2-34 Osteonecrosis of lunate (Kienböck disease). Coronal T1-weighted image of wrist shows loss of normal high-signal fat in lunate (arrow), indicating osteonecrosis.

Fig. 2-35 Osteonecrosis of scaphoid after fracture. Coronal T1-weighted image shows reduced signal in proximal (straight arrow) and distal (curved arrow) fragments, indicating osteonecrosis. Normal marrow signal is preserved in distalmost aspect of scaphoid (open arrow).
Flexor Tendon Ruptures
In the hand, MRI can precisely locate the retracted stump of a ruptured flexor digitorum profundus (FDP) tendon, which is critical for planning the surgical incision (e.g., determining if the tendon has retracted into the palm or remains within the digital sheath).
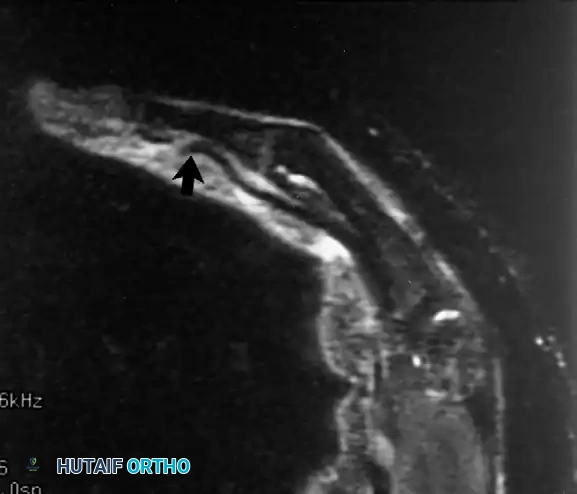
Fig. 2-36 Image of rupture of flexor digitorum profundus tendon in long finger made 2 weeks after repair. Sagittal inversion recovery image shows abrupt discontinuity of flexor tendon (arrow) with laxity of more proximal tendon segment.
MUSCULOSKELETAL TUMOR IMAGING AND SURGICAL ONCOLOGY
Perhaps nowhere in orthopedics has MRI had as profound an impact as in the field of surgical oncology. Exquisite soft-tissue contrast combined with detailed anatomy and multiplanar capability places MRI at the forefront of musculoskeletal tumor imaging. Excellent bone marrow delineation is paramount in defining tumor extent, identifying skip lesions, and planning surgical resection and radiation therapy.
Principles of Oncological Imaging
While MRI frequently helps differentiate aggressive from indolent processes, the contribution of routine radiographs cannot be overemphasized. Interpreting MRI studies without correlating them with orthogonal radiographs is fraught with risk. Most oncological MRI examinations are performed after radiographic detection of an osseous lesion or the discovery of a clinically palpable soft-tissue mass.
Technical Considerations:
* Coil Selection: If the lesion is sufficiently small (< 20 cm) and superficial, a surface coil technique is preferred for high resolution. Larger masses, or lesions in the pelvis and thigh, are best imaged using a body coil or a phased-array torso coil.
* Imaging Planes: Imaging must be performed in at least two planes, one of which must be axial (transverse). The axial plane is critical for defining the relationship of the neoplasm to compartmental boundaries, nearby muscle groups, and major neurovascular bundles. It best demonstrates the extraosseous extension of primary bone tumors. Sagittal and coronal images define the proximal and distal intramedullary extent of the disease.
* Sequences:
* T1-Weighted: Highly sensitive for identifying areas of marrow replacement. Normal fatty marrow is bright; tumor infiltration appears dark.
* T2-Weighted: Delineates soft-tissue extension. Most neoplasms are hyperintense (bright) relative to surrounding muscle and fat due to high water content.
* Fat-Suppression (STIR or T2 Fat-Sat): Invaluable for defining subtle foci of tumor or peritumoral edema by nullifying the bright signal of normal fat.
The Role of Intravenous Gadolinium
The role of intravenous gadolinium in musculoskeletal oncology is nuanced. In the evaluation of soft-tissue masses, contrast-enhanced T1-weighted images can differentiate solid from cystic lesions and assist in biopsy planning by distinguishing viable, actively perfusing tumor from central necrosis.
However, because active tumor, peritumoral edema, and reactive granulation tissue all exhibit enhancement, gadolinium cannot reliably separate the microscopic tumor margin from surrounding reactive changes. While dynamic contrast enhancement (evaluating the rate of contrast uptake) shows promise in distinguishing tumor from edema, it is not universally available. Currently, the routine use of intravenous gadolinium in the initial evaluation of a primary neoplasm is often unnecessary if standard sequences are high quality.
Conversely, in the postoperative setting, gadolinium is mandatory. In a patient who has undergone marginal or wide excision, the presence of nodular areas of contrast enhancement in the surgical bed strongly suggests recurrent or residual neoplasm. Furthermore, preoperative MR angiography with gadolinium can provide critical vascular mapping for highly vascular lesions (e.g., renal cell carcinoma metastases, aneurysmal bone cysts).
Surgical Warning: Biopsy tracts must be meticulously planned. The biopsy incision and tract must be placed perfectly in line with the planned definitive surgical resection so that the entire tract can be excised en bloc with the tumor. Trans-compartmental biopsies are strictly contraindicated.
Soft-Tissue Neoplasms: Specific Pathologies
The detection of soft-tissue masses relies heavily on history and physical examination, as routine radiographs are frequently normal (unless the lesion contains calcification or ossification, such as synovial sarcoma or myositis ossificans). Most soft-tissue lesions have a non-specific MRI appearance: isointense to muscle on T1 and hyperintense on T2. However, certain lesions exhibit tissue-specific signal patterns.
Lipomatous Tumors
Soft-tissue lipomas reveal homogeneous fat signal intensity on all sequences—bright on T1 and T2, and completely dark on fat-suppressed sequences. Subcutaneous lipomas can be difficult to delineate due to a lack of contrast with surrounding normal subcutaneous fat.
Fig. 2-43 Intramuscular lipoma of soleus muscle. A, Coronal T1-weighted image through calf shows marked fatty infiltration of soleus muscle (arrow). B, Coronal inversion recovery image shows complete suppression of fat signal within mass. Muscle fibers exhibit slightly more signal than dark fat (arrow).
The diagnosis of a benign lipoma should be restricted to lesions containing only fat with almost imperceptible, thin fibrous septa. The presence of thick, nodular septa, non-adipose soft-tissue components, or heterogeneous signal demands the consideration of liposarcoma. Myxoid liposarcomas, for instance, often lack macroscopic fat signal entirely, presenting as cystic-appearing, highly water-rich masses.
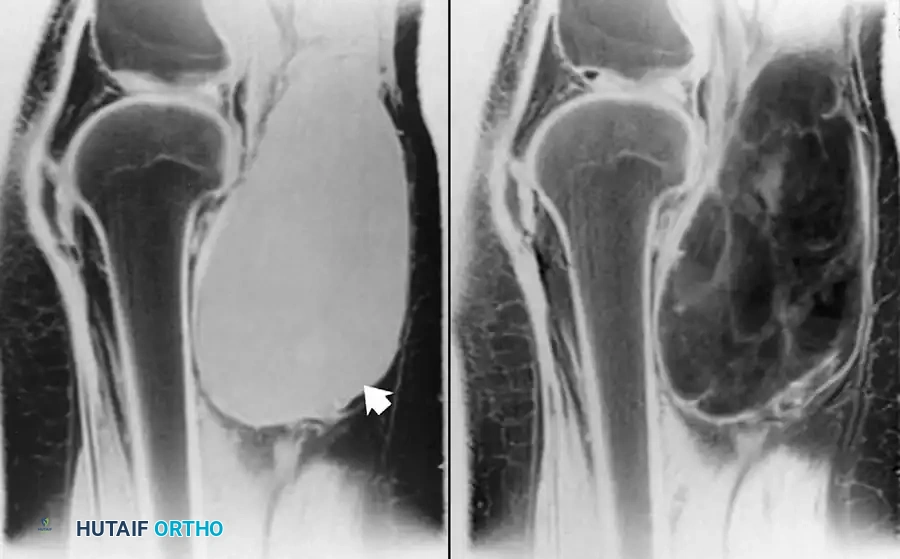
Fig. 2-42 Myxoid liposarcoma of popliteal fossa. A, T1-weighted sagittal image shows well-defined homogeneous mass of intermediate signal intensity (arrow). B, Sagittal T2-weighted image reveals heterogeneous increased signal within lesion. In contrast to well-differentiated liposarcoma, fat signal generally is not seen in this tumor subtype.
Vascular Anomalies (Hemangiomas)
Similar to their intraosseous counterparts, soft-tissue hemangiomas exhibit areas of bright signal on both T1- and T2-weighted studies. This unique signature results from the presence of interspersed adipose tissue and large, cavernous spaces containing slow-flowing blood. Phleboliths (calcified thrombi) may be visible as signal voids.
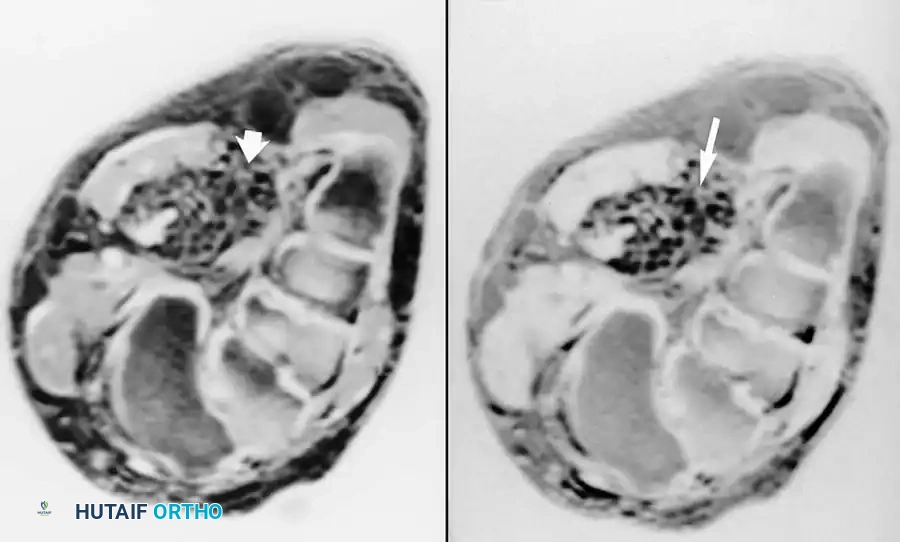
Fig. 2-44 Soft-tissue hemangioma of foot. A, Coronal T1-weighted image of midfoot shows infiltrating mass of heterogeneous increased signal (arrow). B, Corresponding fat-suppressed, T2-weighted image shows markedly increased signal within mass (arrow). Morphology and signal characteristics of this lesion (hyperintense T1 and T2 weighted signal) are typical of hemangiomas.
Pigmented Villonodular Synovitis (PVNS)
PVNS (now formally termed Tenosynovial Giant Cell Tumor) is a benign but locally aggressive proliferative disorder of the synovium. Situated within or around joints, it is characterized by extensive hemosiderin deposition. On MRI, hemosiderin causes magnetic susceptibility artifact, resulting in marked, nodular hypointensity (dark signal) on both T1 and T2-weighted sequences.
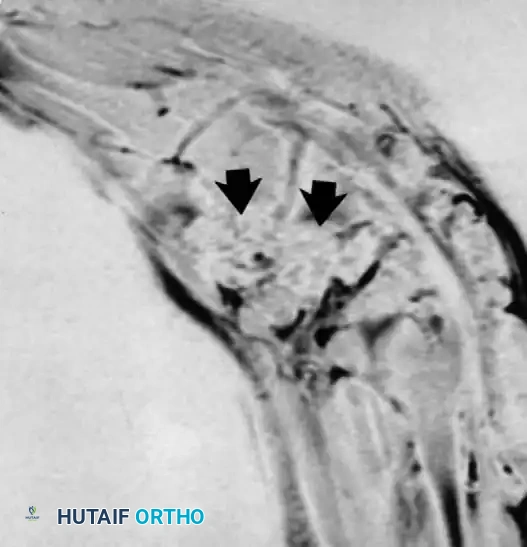
Fig. 2-45 Pigmented villonodular synovitis. A, Sagittal T1-weighted image of foot shows abnormal decreased signal intensity tissue surrounding midfoot (arrows).
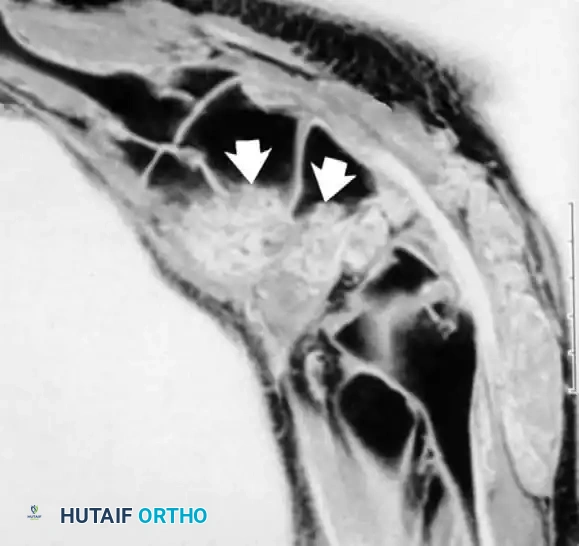
Fig. 2-45 Pigmented villonodular synovitis. B, Sagittal T2-weighted image reveals persistent signal hypointensity resulting from hemosiderin deposition (arrows).
Surgical Management of PVNS:
Treatment requires meticulous, complete synovectomy. In major joints like the knee or elbow, this is often performed arthroscopically, though open synovectomy is required for extensive extra-articular extension. Recurrence rates are high; thus, postoperative external beam radiation or targeted systemic therapies (e.g., CSF1R inhibitors like pexidartinib) may be indicated for diffuse, refractory disease.
Conclusion
The integration of advanced MRI techniques into orthopedic practice has fundamentally altered the surgical approach to both sports-related injuries and musculoskeletal oncology. For elbow pathologies, MRI dictates the necessity and technique of ligamentous and tendinous reconstruction. In the realm of oncology, it provides the anatomic roadmap essential for achieving negative oncologic margins while maximizing limb salvage and functional outcomes. Mastery of these imaging principles is an absolute prerequisite for the modern orthopedic surgeon.
