Advanced MRI Evaluation and Surgical Management of Shoulder Pathology

Key Takeaway
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating complex shoulder pathology, including rotator cuff tears, labral instability, and impingement syndromes. By utilizing specific oblique imaging planes, surface coils, and arthrographic contrast, orthopaedic surgeons can accurately diagnose full-thickness tears, tendinosis, and superior labral anteroposterior (SLAP) lesions. This comprehensive guide details the radiological interpretation, surgical indications, and clinical correlation required for optimal operative planning and postoperative management.
ADVANCED EVALUATION OF THE SHOULDER: IMAGING, BIOMECHANICS, AND SURGICAL MANAGEMENT
The indications for Magnetic Resonance Imaging (MRI) evaluation of the shoulder primarily encompass three interrelated clinical domains: rotator cuff tears, impingement syndromes, and glenohumeral instability. The shoulder is a highly mobile, complex diarthrodial joint that relies heavily on dynamic soft-tissue stabilizers rather than intrinsic osseous congruity. Consequently, evaluating its complex anatomy requires sophisticated imaging techniques, specifically utilizing oblique imaging planes and dedicated surface coil technology to achieve high spatial resolution.
The typical MRI shoulder examination includes axial spin-echo or gradient-echo sequences to meticulously evaluate the glenoid labrum and capsular structures. Oblique coronal images, prescribed parallel to the plane of the supraspinatus tendon, are the gold standard for detecting pathological conditions of the rotator cuff. Furthermore, oblique sagittal images are essential to confirm abnormalities of the cuff tendons and to evaluate the rotator cuff muscle bellies in cross-section, allowing for the assessment of muscle atrophy and fatty infiltration.
While conventional arthrography can detect complete full-thickness tears of the rotator cuff and remains a less expensive procedure, MRI provides significantly more comprehensive information in a noninvasive fashion. Although arthrography is capable of demonstrating full-thickness tears and partial tears along the articular (inferior) surface, it fails to evaluate the bursal surface, the tendon substance, or the quality of the muscle belly—factors that are critical for preoperative planning.
PATHOLOGICAL CONDITIONS OF THE ROTATOR CUFF
Biomechanics and Pathophysiology
The rotator cuff functions as a dynamic stabilizer of the glenohumeral joint through a mechanism known as "concavity compression." The supraspinatus, infraspinatus, teres minor, and subscapularis work in concert to compress the humeral head into the shallow glenoid fossa during arm elevation, counteracting the superior shear forces generated by the deltoid muscle. Disruption of this force couple, either through acute trauma or chronic degenerative tendinopathy, leads to superior migration of the humeral head, secondary impingement, and progressive joint dysfunction.
MRI Interpretation of Rotator Cuff Tears
Oblique coronal spin-echo imaging with T2 weighting optimally detects most pathological conditions of the rotator cuff. With the humerus positioned in neutral to external rotation, the oblique coronal plane is aligned parallel to the supraspinatus tendon. Normally, the tendons of the supraspinatus, infraspinatus, and teres minor maintain a uniformly low signal intensity on all pulse sequences.
Rotator cuff tears manifest as areas of increased T2-weighted signal, representing fluid interposing within the tendon substance. If this hyperintense signal traverses the entire superior-to-inferior thickness of the tendon, it indicates a full-thickness tear.

Figure 2-28A: Oblique coronal T1-weighted image poorly differentiates normal tendon from pathological condition. The lack of fluid sensitivity makes identifying the exact margins of the tear challenging.
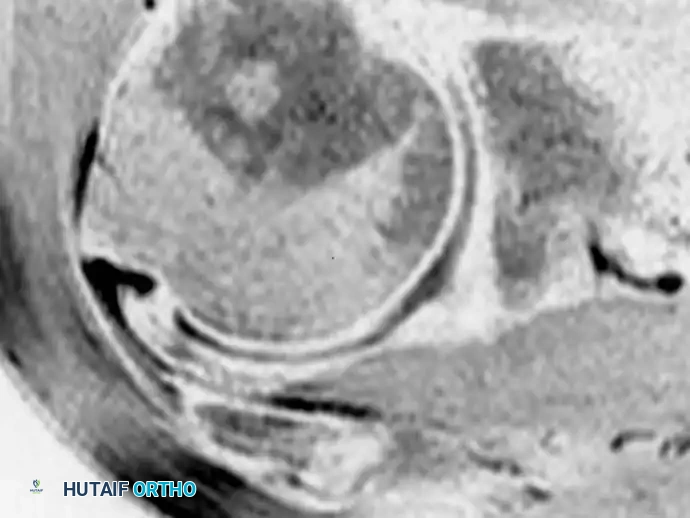
Figure 2-28B: At the same location, an oblique coronal fat-suppressed, T2-weighted image clearly shows a fluid-filled, full-thickness tear (arrow) in the supraspinatus tendon. Fat suppression dramatically increases the conspicuity of the fluid signal.
Alternatively, intact cuff fibers may persist along the articular surface, bursal surface, or both, which is diagnostic of a partial-thickness tear. In the presence of a tear, fluid is frequently identified pooling in the subacromial-subdeltoid bursa.
Clinical Pearl: In patients with massive or chronic tears, the rotator cuff may be so severely retracted and atrophied that its identification over the humeral head is impossible. In these advanced cases, fluid freely communicates between the glenohumeral joint and the subacromial bursa, and the humeral head migrates superiorly, articulating directly with the acromion (acetabularization of the acromion).
Excessive retraction of the cuff tendons (Patte classification) and fatty atrophy of the cuff musculature (Goutallier classification) portend a poor surgical result and high retear rates.
Tendinosis vs. True Tears
Many radiologists and orthopaedic surgeons use the term tendinosis or tendinopathy to describe focal signal abnormalities within the cuff that do not achieve the high signal intensity of fluid on T2-weighted images. Because the "magic angle" artifact frequently occurs within tendons on T1-weighted and gradient-echo images (specifically when the tendon is oriented at 55 degrees to the main magnetic field), the definitive diagnosis of a rotator cuff tear should not be made in the absence of discrete foci of T2-weighted fluid signal abnormalities.
Typically, areas of normal joint fluid can be appreciated elsewhere in the glenohumeral joint to serve as an internal reference for fluid signal intensity. Diffuse or focal signal abnormalities that are less intense than this reference fluid should be considered tendinosis.
Using conventional spin-echo techniques, MRI demonstrates an 80% to 97% sensitivity in detecting full-thickness rotator cuff tears. For the assessment of partial tears, the sensitivity drops to 67% to 89%. However, the addition of fat suppression techniques (such as STIR or fat-saturated T2) has been shown to significantly improve the detection of partial-thickness tears by eliminating the high signal of adjacent peribursal fat.
Postoperative MRI Evaluation
MRI assessment of a previously repaired rotator cuff must be approached with extreme caution.
Surgical Warning: Increased T2-weighted signal can normally be seen within a healing tendon for up to 12-24 months postoperatively. This represents areas of vascularized granulation tissue and remodeling collagen, not necessarily a retear.
For this reason, diagnosing partial-thickness tears in the postoperative shoulder using standard MRI should be avoided. However, larger, fluid-filled, full-thickness defects accompanied by tendon retraction correlate highly with failed repairs or retears. In complex postoperative cases, MRI arthrography is the modality of choice to definitively evaluate the integrity of the repaired rotator cuff.
Surgical Approach: Arthroscopic Rotator Cuff Repair
When conservative management fails and MRI confirms a repairable tear, arthroscopic intervention is indicated.
1. Positioning: The patient is placed in either the beach-chair or lateral decubitus position. The beach-chair position allows for easier conversion to an open approach and better anatomical orientation, while the lateral decubitus position provides excellent joint distraction.
2. Diagnostic Arthroscopy: A standard posterior portal is established. The glenohumeral joint is inspected for concomitant labral or biceps pathology.
3. Subacromial Decompression: The arthroscope is redirected into the subacromial space. A lateral portal is established for instrumentation. A thorough bursectomy is performed to visualize the bursal surface of the cuff and the undersurface of the acromion.
4. Footprint Preparation: The greater tuberosity footprint is decorticated using a motorized burr to create a bleeding bone bed, enhancing biological healing.
5. Anchor Placement and Suture Passing: Suture anchors (biocomposite or PEEK) are placed at the articular margin. Sutures are passed through the tendon using specialized suture-passing devices.
6. Knot Tying/Fixation: A double-row or transosseous-equivalent construct is often utilized to maximize contact area and biomechanical strength, securing the tendon back to its anatomical footprint.
IMPINGEMENT SYNDROMES
Clinical and Radiological Correlation
Although subacromial impingement can be strongly suggested by imaging techniques, it remains fundamentally a clinical diagnosis (characterized by a positive Neer and Hawkins-Kennedy test). MRI is highly valuable in confirming the clinical impression, ruling out full-thickness tears, and providing additional anatomical information regarding the coracoacromial arch.
Imaging findings that suggest the possibility of impingement include:
* Acromial Morphology: A curved (Type II) or hooked (Type III) acromion, as described by Bigliani, significantly decreases the subacromial space.
* Osseous Proliferations: Narrowing of the subacromial space by enthesophytes or osteophytes at the acromioclavicular (AC) joint.
* Soft Tissue Changes: Signal abnormalities in the supraspinatus tendon indicating tendinosis, or fluid in the subacromial-subdeltoid bursa indicating active bursitis.
Surgical Management
If a patient with structurally driven impingement (e.g., a large subacromial spur) fails 3 to 6 months of physical therapy and corticosteroid injections, an arthroscopic subacromial decompression (acromioplasty) is indicated. This involves resecting the coracoacromial ligament and utilizing a burr to flatten the undersurface of the acromion, converting a Type II or III acromion into a flat Type I acromion, thereby restoring the subacromial gliding space.
PATHOLOGICAL CONDITIONS OF THE LABRUM AND INSTABILITY
The Role of MR Arthrography
The glenoid labrum is a fibrocartilaginous ring that deepens the glenoid fossa by 50%, providing critical static stability to the shoulder. Standard non-contrast MRI can struggle to differentiate between normal anatomical variants (such as a sublabral foramen or Buford complex) and true labral tears.
The addition of intraarticular saline or contrast material greatly improves the evaluation of labral pathological conditions and the biceps tendon origin. After the arthrographic instillation of saline, T2-weighted images reveal a hypointense (dark) labrum starkly outlined by bright fluid.
A superior and more widely adopted technique utilizes dilute gadolinium as an intraarticular contrast agent. This allows for T1-weighted imaging, which provides an inherently improved signal-to-noise ratio and exquisite anatomical detail. Imaging is typically performed in a standard position with the arm at the patient’s side.
Figure 2-30: Axial MRI sequence demonstrating the anterior and posterior labrum. Contrast distention allows for the evaluation of capsular redundancy and anterior labral injuries (Bankart lesions).
Advanced Positioning: The ABER View
Additional imaging can be performed with the humerus in Abduction and External Rotation (the ABER position). This position places the inferior glenohumeral ligament (IGHL) under tension, making it the optimal view for assessing the IGHL complex, its origin, and subtle anteroinferior labral tears (pertinent in recurrent anterior instability).
SLAP and Bankart Lesions
- Anterior Labral Injuries (Bankart Lesions): Best visualized in the axial plane. These occur secondary to anterior shoulder dislocations, where the anteroinferior labrum and capsule are avulsed from the glenoid rim.
- Superior Labral Anteroposterior (SLAP) Lesions: Best depicted in axial or coronal images. These involve the superior labrum and the origin of the long head of the biceps tendon.
Using direct MRI arthrography, a sensitivity of 91% and a specificity of 93% have been reported in the detection of pathological labral conditions. However, the accuracy of MRI in the evaluation of SLAP lesions is slightly less, as contrast can sometimes track into normal superior sublabral recesses, mimicking a Type II SLAP tear.
Clinical Pearl - Indirect Arthrography: Some investigators have proposed indirect arthrography as an alternative method of joint opacification. In this technique, delayed intraarticular enhancement is achieved by exercising the joint after the intravenous administration of gadolinium. Although it is a less invasive technique (avoiding a joint injection), the degree of capsular distention is significantly less than that achieved with direct arthrography, making it inferior for detecting subtle capsular laxity.
Surgical Approach: Arthroscopic Labral Repair
- Positioning and Setup: Lateral decubitus positioning is often preferred for instability cases as it provides excellent access to the inferior glenoid.
- Preparation: The torn labrum and capsule are mobilized from the glenoid neck using an elevator. The glenoid rim is decorticated to bleeding bone.
- Anchor Insertion: For a Bankart repair, anchors are typically placed at the 5:30, 4:30, and 3:00 o'clock positions (for a right shoulder).
- Capsulolabral Shift: Sutures are passed through the capsule and labrum, shifting the tissue superiorly and laterally to restore capsular tension and recreate the labral bumper.
OTHER CAUSES OF SHOULDER PAIN
Biceps Tendon Pathology
Pathological conditions of the tendon of the long head of the biceps—including rupture, subluxation/dislocation (often associated with subscapularis tears), or chronic tendinitis—should be routinely detected on standard MRI examinations. Axial images are particularly useful for evaluating the biceps tendon within the bicipital groove.
Suprascapular Nerve Entrapment
An uncommon but critical cause of shoulder pain and weakness is suprascapular nerve entrapment. This is frequently caused by paralabral ganglion cysts located in the spinoglenoid notch or suprascapular notch.
* Pathophysiology: These cysts typically arise from a one-way valve effect caused by an adjacent labral tear (often a posterior or SLAP tear). Joint fluid is pumped into the cyst, which then compresses the suprascapular nerve.
* MRI Appearance: Similar to ganglia elsewhere, these lesions appear as lobular, multiseptate, hyperintense fluid collections on T2-weighted or gradient-echo sequences.
* Clinical Correlation: Compression at the spinoglenoid notch leads to isolated infraspinatus atrophy, while compression at the suprascapular notch affects both the supraspinatus and infraspinatus. The presence of these ganglia must trigger a careful radiological search for the associated labral injury. Surgical management requires arthroscopic labral repair combined with cyst decompression.
Occult Fractures and Osteonecrosis
MRI is highly sensitive for detecting other osseous causes of shoulder pain, such as occult fractures of the greater tuberosity or early-stage osteonecrosis (avascular necrosis) of the humeral head. Osteonecrosis will present with a characteristic "double-line sign" on T2-weighted images, representing the interface between viable and necrotic bone.
Surgical Warning regarding the Brachial Plexus: The brachial plexus is not adequately imaged on a routine shoulder MRI examination. If a pathological condition of the brachial plexus (such as Parsonage-Turner syndrome or traumatic traction injury) is suspected clinically, a dedicated MRI study of the brachial plexus and cervical spine must be explicitly ordered.
POSTOPERATIVE REHABILITATION PROTOCOLS
Successful surgical outcomes in shoulder orthopaedics rely as much on meticulous postoperative rehabilitation as on surgical execution.
Rotator Cuff Repair Protocol:
* Phase I (0-4 Weeks): Maximum protection. The shoulder is immobilized in an abduction sling. Only passive range of motion (PROM) is permitted to prevent stiffness while protecting the healing tendon-to-bone interface.
* Phase II (4-8 Weeks): Active-assisted range of motion (AAROM) is initiated. The sling is gradually weaned.
* Phase III (8-12 Weeks): Active range of motion (AROM) is achieved. Light isotonic strengthening begins, focusing on the periscapular stabilizers and the intact cuff force couples.
* Phase IV (3-6 Months): Advanced strengthening and return to functional/sports-specific activities.
Labral Repair Protocol:
* Phase I (0-4 Weeks): Sling immobilization. External rotation is strictly limited (usually to neutral or 30 degrees) to protect the anterior capsulolabral repair.
* Phase II (4-8 Weeks): Progressive restoration of ROM.
* Phase III (8-12+ Weeks): Strengthening of the dynamic stabilizers. Return to contact sports is typically delayed until 6 months postoperatively to ensure robust biological healing of the fibrocartilage.
