
Introduction and Epidemiology
A fracture of the proximal or distal tibial metaphysis can occur from a variety of high- and low-energy trauma. Fractures may be confined to the metaphysis or extend into the articular surface. Simple fractures suggest lower energy injuries, whereas comminution signifies a greater amount of energy and a higher velocity mechanism.
Common causes of tibial fractures include high-energy collisions (pedestrian versus car bumper) such as an automobile or motorcycle crash. Lower energy injuries, such as certain sports injuries or falls, can also cause fractures of both the proximal or distal tibial metaphysis. Fractures of the tibia can occur in all age groups and from a variety of mechanisms, presenting a bimodal distribution. Young males typically present following high-energy trauma, while older females frequently sustain low-energy osteoporotic fractures.
The goals of treatment include the restoration of length, rotation, and alignment of the tibia with a return to the previous level of activity and function. Recognition and treatment of associated injuries including those to nerves, blood vessels, or compartment syndrome should be an integral part of the assessment and treatment to prevent devastating complications. While diaphyseal tibial fractures are routinely and successfully managed with intramedullary nailing, extending this technique to the metaphyseal regions introduces significant biomechanical and technical challenges. The lack of cortical contact in the "bell-shaped" metaphysis compromises the inherent stability of the intramedullary nail, necessitating advanced reduction techniques, precise entry points, and multi-planar locking configurations.
Surgical Anatomy and Biomechanics
Proximal metaphyseal fractures of the tibia are those that occur proximal to the isthmus of the tibia. Distal metaphyseal fractures of the tibia are those that occur distal to the isthmus of the tibia.
Proximal Tibial Anatomy and Deforming Forces
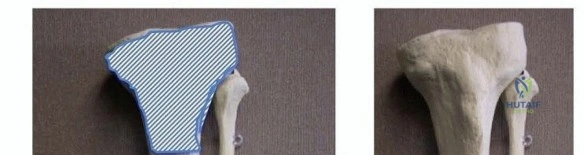
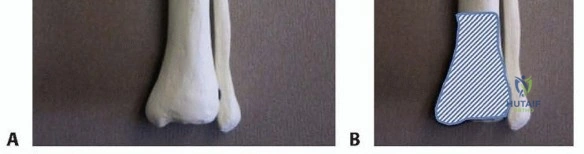
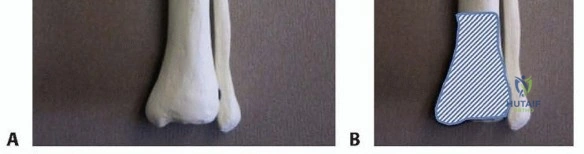
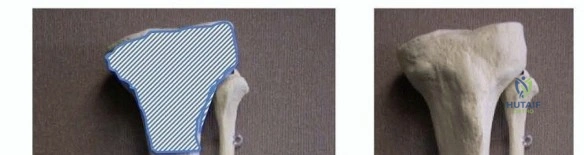
The proximal tibia expands from the narrow diaphyseal isthmus into a wide, cancellous metaphyseal flare. This geometric transition is the primary reason intramedullary nails fail to achieve cortical chatter and subsequent stability in proximal third fractures. The deforming forces in the proximal tibia are profound. The extensor mechanism (patellar tendon) exerts a strong anterior pull on the proximal fragment, leading to apex anterior angulation (procurvatum). Concurrently, the hamstring insertions (pes anserinus medially, biceps femoris laterally) and the iliotibial band create asymmetric forces that frequently result in a valgus deformity.
Distal Tibial Anatomy and Deforming Forces
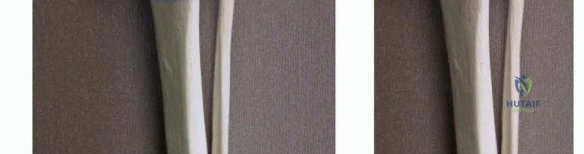
The distal tibia similarly widens into the tibial plafond. The soft tissue envelope in this region is notoriously thin, with minimal muscular coverage anteriorly and medially, making the distal tibia highly susceptible to open fractures and wound healing complications. Biomechanically, the Achilles tendon exerts a strong plantarflexion force on the calcaneus, which translates through the talus to the distal tibial articular block, often driving the distal segment into apex posterior angulation (recurvatum). Furthermore, asymmetric comminution or the presence of an intact or rigidly fixed fibula can drive the distal tibia into varus or valgus malalignment.

Biomechanics of Intramedullary Nailing in the Metaphysis
Standard tibial nails feature a proximal Herzog bend designed to accommodate the anterior entry portal while aligning with the anatomic axis of the diaphysis. In proximal fractures, the wedge effect of this bend, combined with a medullary canal that is significantly wider than the nail, forces the proximal fragment into procurvatum and translation. To counteract this, modern surgical techniques rely on blocking screws (Poller screws), which artificially narrow the metaphyseal canal, direct the path of the nail, and neutralize deforming forces.
Clinical Evaluation and Diagnostic Imaging
Patients will often present with a recent history of trauma. Tibial fractures may present with a variety of findings including pain in the affected extremity with an inability to bear weight, leg length inequality, visual deformity including tenting of the skin, contusions or abrasions, nerve injury, open fractures, and compartment syndrome. Sensory deficits in the foot are less common but require immediate investigation.
Differential Diagnosis
The differential diagnosis in the acute trauma setting includes fractures of the knee, fractures of the ankle, severe soft tissue injury, compartment syndrome, peripheral vascular injury, pathologic processes (tumor or malignancy), and deep space infection.
Imaging Modalities
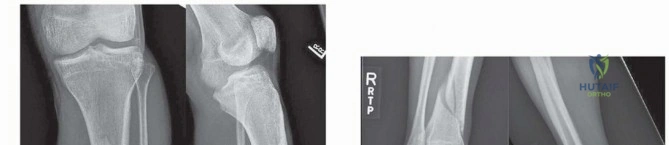
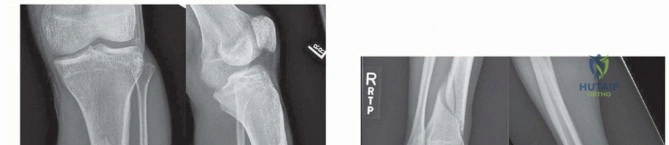
Diagnosis of a proximal or distal tibia fracture can usually be made with standard orthogonal anteroposterior (AP) and lateral radiographs.
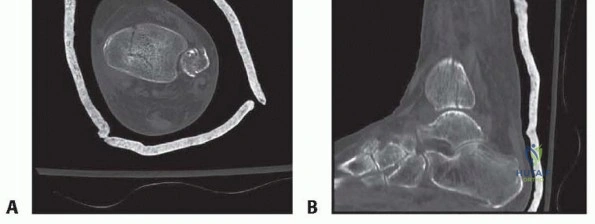
Dedicated knee and ankle radiographs are necessary to decrease the chance of missing a fracture at the articular surface. Fractures that extend proximally or distally into the articular surface frequently require a computed tomography (CT) scan to evaluate joint involvement, assess articular step-off, and aid in meticulous preoperative planning. CT imaging is highly recommended for any distal metaphyseal fracture to rule out occult extension into the tibial plafond, which fundamentally alters the fixation strategy.

Indications and Contraindications
Nonoperative management is normally reserved for lower energy injuries with minimal or no displacement. Patients with low functional demands (e.g., paraplegic) or significant medical comorbidities can be successfully treated without surgical intervention. Nonoperative management of metaphyseal fractures relies on long-leg casting followed by functional bracing, but requires vigilant radiographic follow-up to detect late displacement.
Operative management via intramedullary nailing has become the gold standard for diaphyseal fractures and is increasingly favored for metaphyseal fractures due to its load-sharing biomechanics and preservation of the extraosseous blood supply compared to extensive plating.
| Clinical Scenario | Operative Management (IM Nailing) | Non-Operative Management |
|---|---|---|
| Displacement | > 5 degrees angulation, > 1 cm shortening, > 50% translation | Minimal displacement, stable alignment |
| Soft Tissue Status | Open fractures (Gustilo I, II, IIIA), threatened skin | Intact skin, severe medical contraindications to surgery |
| Polytrauma | Damage control orthopedics, early mobilization required | Isolated injury in non-ambulatory patient |
| Articular Extension | Simple, non-displaced articular splits (requires supplemental lag screws) | Severe intra-articular comminution (relative contraindication for IMN) |
| Patient Factors | High functional demand, compliance with rehab | Non-ambulatory, severe peripheral vascular disease |
Contraindications to IM Nailing: Active intramedullary infection, severe intra-articular comminution precluding stable locking, pediatric patients with open physes (standard antegrade nailing), and critical limb ischemia.
Pre Operative Planning and Patient Positioning
Preoperative templating is paramount. The surgeon must determine the appropriate nail length, diameter, and the specific locking configuration required. For metaphyseal fractures, nails with multi-planar locking options placed at the extreme ends of the implant are mandatory.

Patient Positioning Options
Positioning heavily influences the reduction of metaphyseal fractures.
- Supine on a Radiolucent Flat Table: This is the preferred method for the suprapatellar approach. The leg is positioned with a slight bump under the knee to maintain 15 to 20 degrees of flexion. This minimizes the pull of the extensor mechanism, significantly reducing the risk of procurvatum in proximal fractures.
- Fracture Table or Leg Holder: Historically used for infrapatellar nailing. The knee is flexed to 90 degrees or more. While this facilitates the anterior entry point, it maximizes the pull of the patellar tendon, exacerbating apex anterior angulation in proximal third fractures.


A sterile tourniquet may be applied to the proximal thigh but is rarely inflated unless severe hemorrhage is encountered or open reduction of an articular segment is required.
Detailed Surgical Approach and Technique
Mastering intramedullary nailing of metaphyseal fractures requires strict adherence to reduction principles prior to canal preparation. The nail will follow the reamer, and the reamer will follow the path of least resistance. If the fracture is not reduced prior to reaming, the nail will permanently lock the bone in a malreduced position.
Proximal Tibial Fractures Surgical Technique
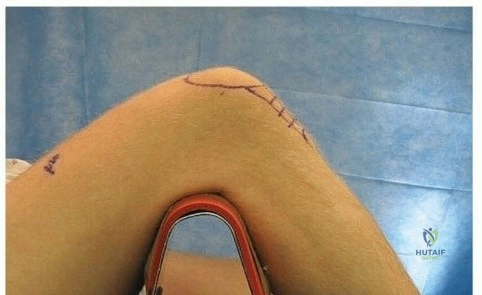
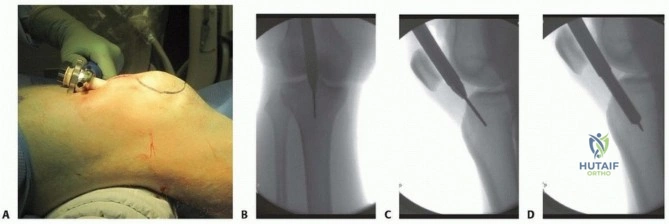
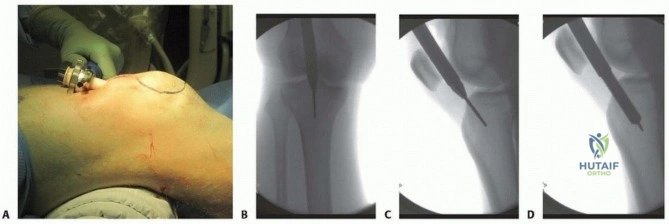
For proximal third fractures, the suprapatellar approach is highly recommended. By keeping the knee in near-extension, the deforming forces of the quadriceps are neutralized.
- Incision and Approach: A 3 to 4 cm longitudinal incision is made proximal to the superior pole of the patella. The quadriceps tendon is split longitudinally.
- Cannula Insertion: A protective trocar and cannula system is passed deep to the patella into the trochlear groove, resting on the proximal tibia.
- Entry Point: The starting point is critical. It must be slightly higher on the anterior slope and slightly more lateral (centered on the lateral tibial spine in the AP plane) compared to diaphyseal fractures. An anterior starting point will inevitably lead to procurvatum.
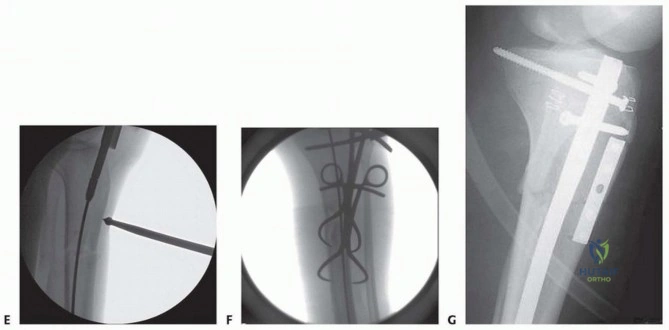
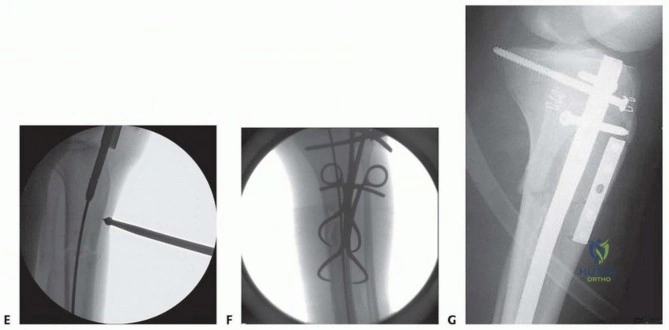
- Reduction and Blocking Screws: Prior to passing the guidewire, the fracture must be reduced. Poller (blocking) screws are placed to narrow the wide metaphyseal canal.
- Rule of Thumb: Place the blocking screw on the concave side of the deformity. For a typical proximal fracture tending toward procurvatum and valgus, place blocking screws posterior and lateral to the intended nail path in the proximal segment.
- Reaming and Nail Insertion: The guidewire is passed, and sequential reaming is performed through the protective cannula. The nail is inserted manually to avoid propagation of occult fracture lines.
- Proximal Locking: Maximize fixation by utilizing all available proximal locking options, including oblique and multi-planar screws, to achieve an interference fit within the cancellous bone.


Distal Tibial Fractures Surgical Technique
Distal metaphyseal fractures require meticulous attention to the distal articular block and the fibula.
- Articular Reconstruction: If CT imaging reveals articular extension, these splits must be anatomically reduced and stabilized with independent lag screws prior to intramedullary reaming. Ensure these screws are placed peripherally so they do not obstruct the path of the nail.
- Fibula Management Controversy: The decision to plate a concomitant fibula fracture is debated. Plating the fibula can restore length and rotational alignment, aiding in the reduction of the distal tibia. However, if the fibula is plated in slight malalignment, it can force the distal tibia into varus or valgus. Current consensus suggests plating the fibula if it is highly unstable or if the syndesmosis is disrupted, but recognizing that the tibia dictates the ultimate alignment.
- Guidewire Placement: The guidewire must be centered perfectly in both the AP and lateral planes within the distal articular block. A wire placed too far medially will result in varus malalignment.
- Distal Blocking Screws: Similar to the proximal tibia, the distal metaphysis is wide. Blocking screws placed adjacent to the fracture in the distal segment can prevent translation and angular deformity during nail insertion.
- Distal Locking: Utilize at least three distal locking screws. Modern nails offer multi-planar distal locking within millimeters of the nail tip, which is essential for capturing the short distal segment.




Complications and Management
Complications following intramedullary nailing of metaphyseal tibial fractures are higher than those of diaphyseal fractures due to the complex biomechanics and tenuous soft tissue envelope.
Compartment Syndrome
This is a devastating acute complication. The tibia is surrounded by four fascial compartments. High-energy trauma, combined with the intramedullary pressure generated during reaming, can elevate intra-compartmental pressures above capillary perfusion pressure. Diagnosis is primarily clinical (pain out of proportion, pain with passive stretch). If suspected, compartment pressures must be measured, and if the delta pressure (Diastolic BP - Compartment Pressure) is less than 30 mmHg, emergent four-compartment fasciotomies are indicated.
Malalignment
Malalignment is the most common technical failure in metaphyseal nailing.
* Proximal: Procurvatum and valgus.
* Distal: Varus and recurvatum.
Prevention through proper positioning, entry point selection, and blocking screws is paramount. If recognized postoperatively, early revision is preferred over late corrective osteotomy.


Complications Summary Table
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Malalignment (>5 degrees) | 10% - 20% | Improper entry point, failure to use blocking screws, un-neutralized deforming forces | Early revision, blocking screws, or late corrective osteotomy |
| Anterior Knee Pain | 30% - 50% | Infrapatellar approach, prominent proximal nail, saphenous nerve injury | Nail removal after union, physical therapy, switch to suprapatellar approach |
| Nonunion / Delayed Union | 5% - 10% | Open fractures, severe comminution, infection, inadequate stability | Dynamization, exchange nailing (larger diameter), bone grafting |
| Compartment Syndrome | 2% - 9% | High-energy crush injuries, aggressive reaming in tight envelopes | Emergent 4-compartment fasciotomy, delayed primary closure/skin grafting |
| Deep Infection | 1% - 5% | Open fractures, compromised soft tissues, prolonged operative time | Irrigation and debridement, suppressive antibiotics, implant removal if loose, antibiotic-coated nails |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation must be tailored to the fracture pattern, the stability of the fixation, and the patient's overall polytrauma status.
- Weight Bearing: For stable, length-stable metaphyseal fractures fixed with multi-planar locking, immediate weight-bearing as tolerated (WBAT) is increasingly advocated to promote callus formation via micromotion. However, for highly comminuted fractures or those with articular extensions lacking rigid lag screw fixation, restricted weight-bearing (toe-touch or partial) for 6 to 8 weeks is prudent to prevent hardware failure or loss of reduction.
- Range of Motion: Early active and passive range of motion of the knee and ankle is initiated immediately postoperatively to prevent arthrofibrosis and promote venous return.
- Deep Vein Thrombosis (DVT) Prophylaxis: Chemical prophylaxis (e.g., Low Molecular Weight Heparin or Direct Oral Anticoagulants) should be administered according to institutional polytrauma guidelines, typically for 2 to 4 weeks, combined with mechanical prophylaxis.
Summary of Key Literature and Guidelines
The evolution of intramedullary nailing for metaphyseal fractures is heavily supported by orthopedic literature.
- The SPRINT Trial (Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures): Demonstrated that reamed intramedullary nailing is superior to unreamed nailing for closed tibial fractures and equivalent for open fractures, establishing reaming as the standard of care.
- Suprapatellar vs. Infrapatellar Nailing: Multiple recent meta-analyses (e.g., Tornetta et al.) have demonstrated that the suprapatellar approach significantly reduces the incidence of proximal malalignment (procurvatum) and may reduce the long-term incidence of anterior knee pain compared to traditional infrapatellar techniques.
- Poller (Blocking) Screws: Originally described by Krettek et al., the biomechanical efficacy of blocking screws in narrowing the metaphyseal canal and directing the nail path remains a cornerstone concept for any surgeon treating proximal or distal tibial fractures with intramedullary devices. Mastery of these adjunctive techniques is mandatory for achieving consistent, anatomic results in the metaphyseal zones.
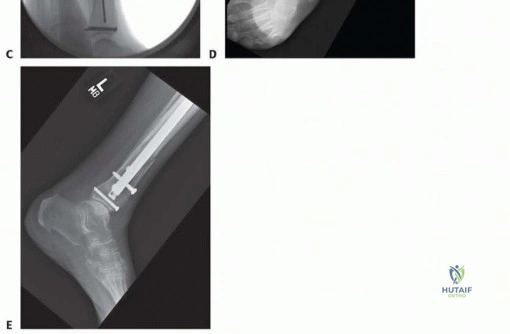
Clinical & Radiographic Imaging













Detailed Chapters & Topics
Dive deeper into specialized chapters regarding intramedullary-nailing-of-metaphyseal-proximal-and-distal-fractures