Distal Tibia Fracture Repair: Mastering Plating and Screws

Key Takeaway
Learn more about Distal Tibia Fracture Repair: Mastering Plating and Screws and how to manage it. Distal tibia medial plating and screws are a surgical technique for open reduction and internal fixation (ORIF) of complex distal tibia and fibula fractures, including those extending into the tibial plafond. This method aims to restore anatomical alignment, length, rotation, and articular surface. The goal is to achieve bony union, minimize post-traumatic arthropathy, and ensure proper function.
"Distal Tibia Fracture Repair: Mastering Plating and Screws"
Introduction and Epidemiology
Distal tibia fractures, particularly those involving the metaphysis and extending into the articular plafond (pilon fractures), represent a significant challenge in orthopedic trauma surgery. These injuries are often high-energy in nature, resulting from falls from height, motor vehicle collisions, or sports-related trauma. The unique anatomical characteristics of the distal tibia, including its subcutaneous location, limited soft tissue envelope, and critical weight-bearing function, contribute to a high incidence of complications and necessitate meticulous surgical planning and execution. Understanding the epidemiology of these fractures is crucial for anticipating patient profiles and potential co-morbidities. They commonly affect younger, active individuals involved in high-energy incidents, but also present in elderly patients with osteoporotic bone following low-energy falls, as exemplified by the index case of a 65-year-old man. The complex interplay of fracture morphology, soft tissue status, and patient factors dictates the optimal management strategy, which often involves staged surgical reconstruction. This discussion will delve into the critical aspects of distal tibia fracture repair, focusing on the principles of plating and screw fixation, from initial assessment and surgical anatomy to detailed operative techniques, potential complications, and rehabilitation protocols.
Surgical Anatomy and Biomechanics
Mastering distal tibia fracture repair necessitates an intimate understanding of the region's complex anatomy and its biomechanical function. The distal tibia is comprised of the metaphyseal-diaphyseal junction, the metaphysis, and the articular plafond. The plafond forms the superior articulation of the ankle joint, interacting with the talus. Its articular surface, characterized by a central groove and medial/lateral facets, is critical for load transmission and requires precise anatomical restoration.
Distal Tibia Anatomy
The distal tibia is characterized by a transition from the triangular cross-section of the tibial diaphysis to a broader, more quadrangular metaphysis and epiphysis. Medially, the bone is relatively subcutaneous, covered by thin skin and minimal muscle, making it susceptible to soft tissue compromise. Laterally, the interosseous membrane separates the anterior and deep posterior compartments. Key anatomical structures to consider include:
- Soft Tissue Envelope: The limited soft tissue coverage, particularly anteromedially, makes this region vulnerable to wound complications, especially in the context of high-energy open injuries.
- Neurovascular Structures:
- Anterior compartment: Anterior tibial artery and deep peroneal nerve pass anterior to the ankle joint.
- Medial compartment: Saphenous vein and nerve are superficial along the anteromedial aspect.
- Posterior compartment: Posterior tibial artery and nerve, and flexor tendons (tibialis posterior, flexor digitorum longus, flexor hallucis longus) are located posteromedially, contained within the tarsal tunnel.
- Lateral compartment: Superficial peroneal nerve and peroneal tendons (peroneus longus and brevis) are situated laterally.
- Ligamentous Structures: The syndesmosis, comprising the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), and interosseous ligament, stabilizes the distal tibiofibular joint. The deltoid ligament medially and the lateral collateral ligaments provide ankle stability.
- Fibular Anatomy: The distal fibula plays a crucial role in maintaining ankle mortise stability and serves as a template for tibial length and rotation. Fractures of the fibula often accompany distal tibia fractures, particularly pilon fractures, and its accurate reduction is paramount before definitive tibial fixation.
 Fig-1a: Anteroposterior radiograph of the left ankle demonstrating a distal tibia and fibula fracture. This initial imaging is crucial for understanding the extent of osseous injury.
Fig-1a: Anteroposterior radiograph of the left ankle demonstrating a distal tibia and fibula fracture. This initial imaging is crucial for understanding the extent of osseous injury.
Biomechanics of the Distal Tibia
The distal tibia and ankle joint are subjected to significant axial and rotational loads during gait and activity. The integrity of the articular surface and the stability of the ankle mortise are fundamental for normal function.
- Load Transmission: The tibial plafond distributes forces from the talus to the tibia. Intra-articular fractures disrupt this load-bearing surface, predisposing to post-traumatic arthritis if not anatomically reduced.
- Syndesmotic Stability: The tibiofibular syndesmosis provides critical stability to the ankle mortise, preventing excessive talar translation and rotation. Disruption of the syndesmosis, often indicated by an associated fibular fracture, mandates its restoration.
- Fibula as a Template: In distal tibia fractures, especially those with comminution, the intact or anatomically reduced fibula acts as a guide for restoring overall tibial length and rotational alignment. Restoring fibular length before tibial plating can simplify the reduction of the more complex tibia fracture.
- Fracture Patterns: High-energy axial compression combined with rotational or shearing forces leads to the comminuted, often intra-articular fracture patterns seen in pilon fractures (e.g., AO/OTA 43C2.3). The energy dissipated determines the degree of articular involvement and metaphyseal comminution. The index case highlights a distal third tibia fracture with extension into the tibial plafond, categorized as AO/OTA 43C2.3, indicating significant articular and metaphyseal involvement.
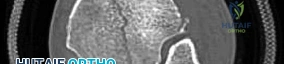
 Fig-2: Computed tomographic (CT) scan axial view revealing the complex articular involvement and comminution characteristic of an AO/OTA 43C2.3 fracture. CT scans are indispensable for detailed pre-operative planning.
Fig-2: Computed tomographic (CT) scan axial view revealing the complex articular involvement and comminution characteristic of an AO/OTA 43C2.3 fracture. CT scans are indispensable for detailed pre-operative planning.
Indications and Contraindications
The decision-making process for distal tibia fractures, particularly those involving the articular surface, is multifactorial, considering fracture morphology, soft tissue status, patient comorbidities, and surgeon expertise. A staged approach is frequently preferred, especially in high-energy injuries with significant soft tissue swelling or open wounds.
Operative Indications for Distal Tibia Fractures
Operative intervention is typically indicated for displaced or unstable fractures where non-operative management is unlikely to achieve satisfactory anatomical reduction and functional outcomes.
- Displaced Intra-Articular Fractures (Pilon Fractures): Any significant displacement (>2mm) or step-off of the articular surface, particularly in young, active patients, warrants surgical stabilization to restore joint congruity and minimize the risk of post-traumatic arthritis.
- Unstable Extra-Articular Distal Tibia Fractures: Fractures of the distal metaphysis that are significantly displaced, shortened, or angulated, and cannot be adequately reduced or maintained by closed means.
- Open Fractures: All open fractures require immediate irrigation and debridement (I&D) to prevent infection, followed by stabilization. This often involves external fixation as a temporizing measure, with definitive internal fixation performed once the soft tissue envelope has recovered. The index case presented with a small open wound over the fibular fracture, necessitating immediate I&D and external fixation.
 Fig-3: Clinical photograph demonstrating the external fixator applied for temporary stabilization following initial irrigation and debridement of the open fracture.
Fig-3: Clinical photograph demonstrating the external fixator applied for temporary stabilization following initial irrigation and debridement of the open fracture.
- Polytrauma Patients: Early stabilization of long bone fractures, including the distal tibia, is part of damage control orthopedics in polytrauma patients to reduce systemic inflammatory response and improve overall outcomes.
- Fractures with Neurovascular Compromise: Although rare, if closed reduction fails to restore perfusion or relieve nerve compression, operative intervention is indicated.
- Fractures with Compartment Syndrome: While prophylactic fasciotomy is controversial, established compartment syndrome necessitates emergency fasciotomy, often followed by staged fracture stabilization.
Non-Operative Indications for Distal Tibia Fractures
Non-operative management may be considered in a select group of patients, primarily those with stable, minimally displaced fractures or those with significant medical contraindications to surgery.
- Non-Displaced, Stable Extra-Articular Fractures: Fractures with minimal displacement, no articular involvement, and maintained alignment can sometimes be managed with cast immobilization, provided close follow-up ensures no secondary displacement.
- Medically Unstable Patients: Patients with severe comorbidities that preclude safe anesthesia and surgery may be managed non-operatively, accepting a potentially suboptimal anatomical outcome in favor of survival and reduced perioperative risk.
- Severe Soft Tissue Compromise (Relative): In cases of extreme soft tissue damage, the initial treatment may involve external fixation and soft tissue reconstruction, delaying definitive plating until the soft tissues are amenable to internal fixation. This is more of a staged approach than a true non-operative decision.
Contraindications to Operative Intervention
Absolute contraindications are rare, but relative contraindications significantly influence the timing and approach to surgery.
- Absolute Contraindications: Severely compromised soft tissues that cannot be adequately prepared for internal fixation, even with staged approaches, may necessitate alternative strategies like definitive external fixation or primary amputation in extreme cases.
- Relative Contraindications:
- Extremely poor surgical candidate: Severe medical comorbidities (e.g., uncontrolled diabetes, severe peripheral vascular disease, end-stage renal disease) that significantly increase operative risks.
- Active infection: Unless the fracture itself is the source and needs debridement, active systemic infection generally defers elective definitive internal fixation.
- Patient non-compliance: Inability to adhere to post-operative rehabilitation protocols can impact outcomes.
Table of Indications for Distal Tibia Fracture Management
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Pattern | Displaced intra-articular fractures (pilon) with >2mm step-off/gaps, significant comminution (e.g., AO/OTA 43C2, 43C3). Unstable extra-articular distal metaphyseal fractures (AO/OTA 43A, 43B) with unacceptable angulation (>5 degrees), shortening (>1cm), or rotation. | Minimally displaced extra-articular fractures (<5 degrees angulation, <1cm shortening, no rotational deformity). Stable, non-displaced metaphyseal fractures in patients with low functional demands. |
| Soft Tissue | Open fractures (urgent I&D and stabilization). Significant soft tissue swelling (after resolution/staging). | Severe soft tissue compromise (e.g., large degloving, severe crush injury) precluding immediate safe internal fixation; often managed with temporizing external fixation followed by soft tissue coverage. |
| Patient Status | Polytrauma patients (for damage control orthopedics). Neurologic compromise due to fracture. | Medically unstable patients (ASA >III) where operative risks outweigh benefits. Patients with severe peripheral vascular disease or other comorbidities that significantly impair wound healing. |
| Associated Injury | Compartment syndrome (fasciotomy and fixation). Associated fibular fracture causing ankle instability (syndesmotic disruption). | |
| Functional Demand | High functional demand patients where anatomical reduction is critical for long-term outcome. | Elderly, low functional demand patients where acceptable alignment can be achieved with non-operative methods, or where surgical risks are deemed too high. |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful distal tibia fracture repair, minimizing intraoperative surprises and optimizing outcomes. This phase involves meticulous assessment, imaging interpretation, staged management decisions, and detailed surgical blueprinting.
Initial Management and Staging
The immediate post-injury management, as demonstrated in the index case, is critical.
* Clinical Assessment: Evaluate for neurovascular compromise, assess the integrity of the skin and soft tissue envelope. Note any lacerations, ecchymosis, or blistering. The presence of a small laceration over the fibular fracture, indicating an open fracture (Gustilo-Anderson Type I), mandates immediate attention.
* Open Fracture Protocol: For open fractures, immediate tetanus prophylaxis, intravenous broad-spectrum antibiotics (e.g., cefazolin), and surgical irrigation and debridement (I&D) are paramount. The goal is to minimize bacterial contamination and prevent infection.
* Temporary Stabilization: Application of a spanning external fixator provides temporary stability, restores gross alignment, protects the soft tissues, and facilitates nursing care. This allows time for soft tissue swelling to subside, crucial for definitive internal fixation.
*  Fig-1d: Lateral radiograph showing the distal tibia fracture with significant displacement.
Fig-1d: Lateral radiograph showing the distal tibia fracture with significant displacement.
*  Fig-1c: Oblique radiograph depicting the fracture pattern more clearly.
Fig-1c: Oblique radiograph depicting the fracture pattern more clearly.
*  Fig-1b: Anteroposterior radiograph (different angle) of the left ankle, complementing Fig-1a for a comprehensive initial assessment.
Fig-1b: Anteroposterior radiograph (different angle) of the left ankle, complementing Fig-1a for a comprehensive initial assessment.
* Compartment Syndrome Monitoring: Close monitoring for compartment syndrome is essential, especially in high-energy injuries.
Advanced Imaging
- Radiographs: Initial AP, lateral, and oblique views of the ankle and tibia are mandatory to assess the fracture pattern, degree of comminution, and any associated fibular injury. Long leg radiographs may be needed to rule out ipsilateral knee or proximal tibia injuries, especially relevant given the patient's prior ipsilateral total knee arthroplasty (TKA).
- Computed Tomography (CT) Scan: A CT scan with fine cuts through the ankle joint and 3D reconstructions is indispensable. It precisely delineates the articular involvement, number and size of fragments, degree of comminution, and posterior malleolar involvement. This information is critical for surgical planning. The AO/OTA classification (e.g., 43C2.3 in the case description) is based on these detailed imaging findings.
Definitive Surgical Planning
Once the soft tissue envelope is amenable to surgery (wrinkle sign present, minimal edema, no blistering), definitive fixation can proceed.
* Approach Selection: Based on the fracture pattern and comminution, decide on the optimal surgical approach (anteromedial, anterolateral, posteromedial, or a combination).
* Reduction Strategy: Plan the sequence of reduction maneuvers. This often involves restoring fibular length and rotation first, followed by reduction of the main articular fragments, and then bridging the metaphyseal comminution to the diaphysis. Ligamentotaxis, direct reduction (mini-open), and external fixator-assisted reduction are key techniques.
* Implant Choice: Select appropriate implants. Distal tibia locking plates (e.g., LCP plates) are commonly used due to their ability to provide stable fixation in comminuted metaphyses and osteoporotic bone. Consider plate length, screw number, and trajectory. A medial plate is commonly chosen for distal tibia fractures, as indicated in the seed content.
* Ancillary Procedures: Plan for bone grafting if significant metaphyseal defects are present after reduction, or if there's an anticipated high risk of nonunion.
* Previous Ipsilateral TKA: The presence of a prior ipsilateral total knee arthroplasty (TKA) should be noted. This could influence patient positioning, the potential for using a long nail, or general surgical considerations, although for a distal tibia fracture requiring plating, its direct impact on the distal tibia approach is usually limited to anesthetic and positioning considerations.
Patient Positioning and Drape
- Position: The patient is typically positioned supine on a radiolucent table. A bump may be placed under the ipsilateral hip to allow for internal rotation of the leg, if needed for access.
- Tourniquet: A thigh tourniquet is applied for a bloodless field, crucial for visualization and precise reduction.
- Fluoroscopy: Ensure the image intensifier (C-arm) can obtain true AP, lateral, and oblique views of the distal tibia and ankle without obstruction. Test this pre-drape.
- Draping: The entire lower extremity is prepped and draped freely to allow for manipulation of the limb and adjustment of fluoroscopy.
Detailed Surgical Approach and Technique
The surgical repair of a distal tibia fracture, especially one involving the articular surface, demands a systematic and meticulous approach. The objective is anatomical reduction of the articular surface, restoration of axial alignment, length, and rotation, and stable fixation to permit early rehabilitation while respecting the fragile soft tissue envelope. The "medial plating" mentioned in the seed content suggests an anteromedial approach, which is commonly employed.
Anteromedial Surgical Approach to the Distal Tibia
This approach provides excellent access to the medial aspect of the distal tibia, which is often comminuted, and allows direct visualization of the medial articular fragments.
- Incision: A longitudinal incision is made along the anteromedial aspect of the distal tibia, typically centered over the proposed plate position. It should extend proximally enough to allow adequate plate length and distally to visualize the medial malleolus and plafond. Care is taken to design the incision to preserve viable skin bridges if other incisions (e.g., for fibula) are contemplated. The saphenous vein and nerve are identified and protected, often retracted anteriorly or posteriorly.
 Fig-16: Anteroposterior fluoroscopic view showing the plate position relative to the syndesmosis.
Fig-16: Anteroposterior fluoroscopic view showing the plate position relative to the syndesmosis. Fig-17: Lateral fluoroscopic view confirming plate position and screw trajectories.
Fig-17: Lateral fluoroscopic view confirming plate position and screw trajectories.
- Dissection: The subcutaneous tissue is incised, and full-thickness flaps are carefully raised to expose the periosteum of the distal tibia. Aggressive retraction or excessive stripping of periosteum should be avoided to preserve vascularity. The deep fascia is incised longitudinally. The tibialis anterior muscle may be retracted laterally to expose the anterior tibial metaphysis, if needed.
Fibula Fixation (If Applicable)
In many distal tibia fractures, particularly pilon fractures, an associated fibula fracture is present. Restoring the fibular length and rotation first is a critical step, as the fibula acts as a template for the tibia.
- Approach: A separate lateral incision can be made over the fibular fracture.
- Reduction: The fibular fracture is anatomically reduced, ensuring correct length and rotation.
- Fixation: Typically, a one-third tubular plate or a locking plate is applied to the lateral aspect of the fibula, secured with screws. Intraoperative fluoroscopy confirms reduction and hardware placement.
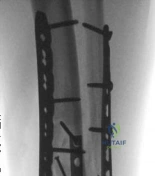 Fig-4: Radiograph of the distal tibia and fibula post-reduction and external fixation, prior to definitive internal fixation.
Fig-4: Radiograph of the distal tibia and fibula post-reduction and external fixation, prior to definitive internal fixation. Fig-5: Intraoperative photograph showing the external fixator in place.
Fig-5: Intraoperative photograph showing the external fixator in place. Fig-6: Intraoperative photograph during fibular reduction and plating.
Fig-6: Intraoperative photograph during fibular reduction and plating.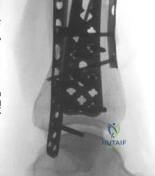 Fig-7: Fluoroscopic image of fibular fixation with a plate and screws.
Fig-7: Fluoroscopic image of fibular fixation with a plate and screws.- Fig-8: Post-operative radiograph (AP view) after fibular plating.
 Fig-9: Post-operative radiograph (lateral view) after fibular plating.
Fig-9: Post-operative radiograph (lateral view) after fibular plating.
Tibial Fracture Reduction
This is the most challenging aspect, especially with articular involvement.
* Indirect Reduction (Ligamentotaxis): With the external fixator still in place (or reapplied if removed), axial traction can be applied to achieve gross length and alignment. This helps to reduce articular fragments through tension on soft tissue attachments.
* Direct Reduction (Mini-Open): Small incisions or a limited arthrotomy can be made to directly visualize and reduce articular fragments. Fragment-specific fixation using K-wires or small screws (e.g., 2.0 or 2.7 mm) is often employed first to reconstruct the articular surface.
* 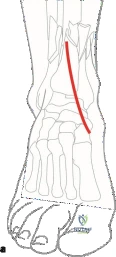 Fig-10: Intraoperative photograph during the reduction of the main tibial fracture fragments using provisional K-wires.
Fig-10: Intraoperative photograph during the reduction of the main tibial fracture fragments using provisional K-wires.
* Fragment-Specific Fixation: Each major articular fragment is reduced to its anatomical position and temporarily secured with K-wires. This involves meticulous anatomical restoration of the plafond.
* 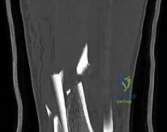 Fig-11: Fluoroscopic image showing initial reduction with K-wires.
Fig-11: Fluoroscopic image showing initial reduction with K-wires.
*  Fig-12: Another fluoroscopic view highlighting articular reduction with provisional fixation.
Fig-12: Another fluoroscopic view highlighting articular reduction with provisional fixation.
* Metaphyseal Reduction: Once the articular block is reconstructed, it is then reduced to the tibial diaphysis. This can be challenging in comminuted fractures. Techniques include:
* Ligamentotaxis: As described above, to gain length and rough alignment.
* External Fixator-Assisted: The ex-fix can be used to distract, compress, and angulate to aid reduction.
* Direct Manipulation: Using clamps, periosteal elevators, and bone hooks through the minimal soft tissue exposure.
Plate Application and Screw Fixation
The choice of plate and screw technique is crucial for stable fixation. Medial locking plates are commonly used for distal tibia fractures, offering stable construct in the metaphyseal bone.
1. Plate Contouring: An anatomically pre-contoured distal tibia locking plate is typically used. While pre-contoured, minor adjustments may be needed to achieve optimal fit on the bone, especially in cases with unique anatomy or significant deformity. The plate should sit flush on the bone surface without causing undue soft tissue tension.
*  Fig-13: Intraoperative image showing the contoured medial locking plate being positioned on the distal tibia.
Fig-13: Intraoperative image showing the contoured medial locking plate being positioned on the distal tibia.
*  Fig-14: Fluoroscopic view confirming plate placement and initial screw trajectory.
Fig-14: Fluoroscopic view confirming plate placement and initial screw trajectory.
2. Proximal Plate Fixation: The plate is first secured proximally to the tibial diaphysis using bicortical locking screws. Ensure good purchase in the cortical bone.
3. Distal Plate Fixation (Articular Block):
* Non-Locking Screws (Lag Screws): If direct compression of an articular fragment is desired, a non-locking lag screw can be placed through a dynamic compression unit (DCU) hole or a dedicated lag screw hole in the plate. This is done before placing locking screws in the same segment to allow for compression.
*  Fig-18: Intraoperative view after initial plate application, showing guide wires for distal locking screws.
Fig-18: Intraoperative view after initial plate application, showing guide wires for distal locking screws.
*  Fig-19: Fluoroscopic image showing the placement of distal screws, ensuring they do not penetrate the articular surface.
Fig-19: Fluoroscopic image showing the placement of distal screws, ensuring they do not penetrate the articular surface.
*  Fig-20: Close-up intraoperative view of screw insertion.
Fig-20: Close-up intraoperative view of screw insertion.
* 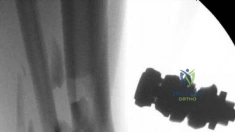 Fig-21: Fluoroscopic image demonstrating the final screw configuration in the distal fragment.
Fig-21: Fluoroscopic image demonstrating the final screw configuration in the distal fragment.
* Locking Screws: Distal screws are predominantly locking screws, providing angular stability in the comminuted metaphyseal and epiphyseal bone. These screws should be directed into specific fragments of the articular block, avoiding joint penetration. Multiple screws (typically 3-5) are placed into the distal articular segment, ensuring good purchase in the subchondral bone. These screws create a fixed-angle construct, reducing the risk of plate pull-out or loss of reduction in osteoporotic bone.
* Fig-22: Post-operative AP radiograph showing the definitive medial plate and screw construct for the tibia.
*  Fig-23: Post-operative lateral radiograph, confirming reduction and hardware position.
Fig-23: Post-operative lateral radiograph, confirming reduction and hardware position.
*  Fig-24: Post-operative oblique radiograph providing additional views of the internal fixation.
Fig-24: Post-operative oblique radiograph providing additional views of the internal fixation.
4. Metaphyseal Screws: Screws are also placed into the metaphyseal region to bridge comminution and secure the plate to the main bone fragments.
5. Cortical Screws: Non-locking cortical screws may be used in the diaphyseal portion of the plate to provide additional compression or aid in initial reduction before locking screws are placed.
*  Fig-15: Final intraoperative view of the plate secured with screws.
Fig-15: Final intraoperative view of the plate secured with screws.
Final Assessment
- Fluoroscopic Evaluation: Obtain AP, lateral, and oblique fluoroscopic images to confirm anatomical reduction of the articular surface, proper alignment of the tibia (length, rotation, angulation), and appropriate placement of all hardware, ensuring no screws penetrate the joint space.
- Ankle Stability: Assess the stability of the ankle mortise and syndesmosis. If there is concern for syndesmotic instability after fibular and tibial plating, stress views or a dedicated syndesmotic screw may be considered.
- Range of Motion: Gently assess passive ankle range of motion to ensure no mechanical block from hardware or malreduction.
Wound Closure
- Hemostasis: Achieve meticulous hemostasis.
- Drain: A suction drain may be considered if there is significant dead space or concern for hematoma formation, although this is surgeon-dependent.
- Soft Tissue Closure: Close the deep fascia, subcutaneous tissue, and skin layers carefully without tension. Avoid excessive suturing or tight closure to minimize the risk of wound complications in this vulnerable area.
 Fig-46: Clinical photograph of the closed incision.
Fig-46: Clinical photograph of the closed incision.
Examples of Other Approaches and Techniques (Brief Overview)
- Anterolateral Approach: Used for fractures predominantly involving the anterolateral plafond or for biplanar plating (e.g., in complex pilon fractures).
- Posteromedial/Posterolateral Approaches: Essential for posterior malleolar fractures or large posterior articular fragments. These approaches avoid the compromised anterior soft tissues and can provide direct visualization for posterior fragment reduction.
- Minimally Invasive Plate Osteosynthesis (MIPO): Increasingly popular for metaphyseal fractures without significant articular comminution. Small incisions are used for plate insertion and percutaneous screw placement, minimizing soft tissue disruption. While less common for true pilon fractures, it can be advantageous for lower energy distal metaphyseal fractures.
 Fig-25: AP radiograph of an alternative plating strategy using a different approach or plate type.
Fig-25: AP radiograph of an alternative plating strategy using a different approach or plate type. Fig-26: Lateral radiograph of an alternative plating strategy.
Fig-26: Lateral radiograph of an alternative plating strategy. Fig-27: Oblique radiograph of an alternative plating strategy.
Fig-27: Oblique radiograph of an alternative plating strategy.
Complications and Management
Distal tibia fractures, particularly pilon fractures, are associated with a high rate of complications due to the severity of injury, extensive soft tissue damage, and challenges in achieving anatomical reduction and stable fixation. Vigilant post-operative monitoring and prompt management are crucial for optimal outcomes.
Common Complications
- Wound Complications and Infection: Given the thin soft tissue envelope and high-energy mechanism, wound dehiscence, necrosis, and deep infection are significant concerns. Open fractures further increase this risk.
- Incidence: Up to 30% for wound complications, 5-15% for deep infection.
- Management: Meticulous wound care, early debridement for necrosis, aggressive I&D for deep infection, often with hardware removal and soft tissue reconstruction (e.g., muscle flaps) if required. Staged approach and delayed definitive fixation are key preventive measures.
 Fig-28: Post-operative AP radiograph showing stable fixation (example of good outcome).
Fig-28: Post-operative AP radiograph showing stable fixation (example of good outcome). Fig-29: Post-operative lateral radiograph showing stable fixation (example of good outcome).
Fig-29: Post-operative lateral radiograph showing stable fixation (example of good outcome).
- Nonunion and Malunion: Extensive comminution, soft tissue compromise, infection, and inadequate fixation can lead to delayed union or nonunion. Malunion can occur if anatomical alignment is not achieved or maintained.
- Incidence: 5-20% for nonunion, higher for malunion.
- Management: Revision surgery with debridement of nonunion site, re-reduction, stable fixation (e.g., larger plate, allograft/autograft bone grafting, bone stimulators). For symptomatic malunion, corrective osteotomy may be required.
 Fig-30: Post-operative AP radiograph at a later follow-up showing early signs of consolidation.
Fig-30: Post-operative AP radiograph at a later follow-up showing early signs of consolidation. Fig-31: Post-operative lateral radiograph at a later follow-up.
Fig-31: Post-operative lateral radiograph at a later follow-up.
- Post-Traumatic Arthritis: Particularly common in intra-articular fractures (pilon) due to residual articular incongruity, cartilage damage, and altered biomechanics.
- Incidence: Up to 50% in pilon fractures.
- Management: Conservative measures (NSAIDs, injections, physical therapy), arthroscopic debridement, osteotomies, or ultimately, ankle arthrodesis (fusion) or total ankle arthroplasty (replacement) for severe, debilitating arthritis.
 Fig-32: Follow-up AP radiograph showing progression towards healing.
Fig-32: Follow-up AP radiograph showing progression towards healing.
- Hardware-Related Complications: Prominent hardware, hardware failure (breakage, pull-out), or irritation of surrounding tendons/nerves.
- Incidence: Variable, but common due to subcutaneous nature.
- Management: Symptomatic hardware removal after fracture union (typically 12-18 months post-op). Revision fixation for hardware failure if reduction is lost.
 Fig-33: Follow-up AP radiograph at 3 months post-op.
Fig-33: Follow-up AP radiograph at 3 months post-op. Fig-34: Follow-up lateral radiograph at 3 months post-op.
Fig-34: Follow-up lateral radiograph at 3 months post-op.
- Compartment Syndrome: Though initially managed, it can still develop or be missed.
- Incidence: 1-5%.
- Management: Emergency fasciotomy.
- Nerve Injury: Damage to superficial peroneal, saphenous, or deep peroneal nerves during dissection or by prominent hardware.
- Incidence: Rare to moderate.
- Management: Protection during surgery, neurolysis or exploration if severe.
- Reflex Sympathetic Dystrophy (CRPS): Chronic pain condition.
- Incidence: Up to 10%.
- Management: Early diagnosis, physical therapy, pain management, regional nerve blocks.
 Fig-35: Follow-up AP radiograph at 6 months post-op, showing good healing.
Fig-35: Follow-up AP radiograph at 6 months post-op, showing good healing. Fig-36: Follow-up lateral radiograph at 6 months post-op.
Fig-36: Follow-up lateral radiograph at 6 months post-op. Fig-37: Follow-up oblique radiograph at 6 months post-op.
Fig-37: Follow-up oblique radiograph at 6 months post-op.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
| Infection | 5-15% (Deep) | Urgent aggressive irrigation and debridement, antibiotics (IV for 6 weeks +/- oral for 3-6 months), culture-directed antibiotics, possible hardware removal, bone grafting if required. If large soft tissue defect, plastic surgery consultation for flap coverage. |
| Primary Injury | | |
| Wound Breakdown/Necrosis | Up to 30% | Local wound care (debridement, dressings), negative pressure wound therapy (NPWT), rotational muscle flap or free flap coverage, staged closure. Aggressive debridement for non-viable tissue. |
| Nonunion/Malunion | 5-20% (Nonunion) | Revision ORIF with plate fixation, bone grafting (autograft/allograft, bone marrow aspirate, DBM) for nonunion. Corrective osteotomy and refixation for symptomatic malunion. Ex-fix and bone transport for segmental defects. |
| Post-Traumatic Arthritis | Up to 50% (Pilon Fx) | Conservative management (NSAIDs, injections, bracing), physical therapy, activity modification. Surgical: Arthroscopic debridement, osteotomies, ankle arthrodesis (fusion) or total ankle arthroplasty. |
| * *Malunion/Deformity | Higher in articular Fx | Revision osteotomy to restore alignment and joint congruity, possibly with internal fixation and bone grafting. |
| Post-Traumatic Arthritis | Up to 50% (Pilon Fx) | Conservative management (NSAIDs, injections, bracing), physical therapy, activity modification. Surgical options: Arthroscopic debridement for mild cases, osteotomies to correct alignment, or ultimately ankle arthrodesis or total ankle arthroplasty for severe, debilitating arthritis. |
| Hardware Irritation/Failure | Common (subcutaneous) | Symptomatic hardware removal (usually after fracture union). Revision fixation if hardware failure leads to loss of reduction. |
| Nerve Impingement/Injury | Low to moderate | Intraoperative protection/identification. Post-operative: Conservative management (observation, NSAIDs) for neurapraxia. Surgical: Neurolysis or exploration for persistent symptoms or clear evidence of entrapment. |
| Complex Regional Pain Syndrome | 2-10% | Early diagnosis and multi-modal treatment: aggressive physical therapy, pain medication (gabapentin, tricyclics), regional nerve blocks, psychological support. |
Post Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is paramount for optimizing functional outcomes following distal tibia fracture repair. The protocol must be individualized, considering the fracture stability, quality of fixation, patient's bone quality, and overall soft tissue healing.
Immediate Post-Operative Period (0-2 weeks)
- Immobilization: The extremity is typically immobilized in a removable splint or boot (e.g., CAM walker) to protect the surgical site and hardware.
- Elevation: Strict elevation of the limb above the heart is maintained to minimize swelling and promote wound healing.
- Weight-Bearing: Non-weight bearing (NWB) is strictly enforced on the operative leg. Crutches or a walker are used for ambulation.
- Early Motion:
- Toe ROM: Gentle active range of motion of the toes is encouraged to maintain circulation and prevent stiffness.
- Knee ROM: If not contraindicated, active and passive knee range of motion exercises are started to prevent stiffness in the ipsilateral knee, especially relevant in the context of a previous TKA.
- Wound Care: Daily wound inspection, dressing changes, and monitoring for signs of infection or wound breakdown.
 Fig-38: Clinical photograph of the post-operative incision during early follow-up.
Fig-38: Clinical photograph of the post-operative incision during early follow-up.
Early Mobilization and Progressive Weight-Bearing (2-6 weeks)
- Radiographic Assessment: Initial post-operative radiographs are reviewed for reduction and hardware position.
- Soft Tissue Healing: Once incisions are well-healed and swelling has significantly decreased (typically around 2-3 weeks).
- Ankle ROM: Gentle, progressive active and passive ankle range of motion exercises are initiated within the protected splint/boot. This may include dorsiflexion, plantarflexion, inversion, and eversion, avoiding excessive stress on the fracture site. Non-impact loading.
- Theraband Exercises: Light strengthening exercises for ankle musculature using elastic bands.
- Isometric Exercises: Gentle isometric contractions of calf and tibialis anterior muscles.
- Weight-Bearing: Touch-down weight-bearing (TDWB) or 10-20% partial weight-bearing (PWB) may be initiated based on radiographic evidence of early healing and fracture stability, gradually progressing as tolerated and as per surgeon's discretion.
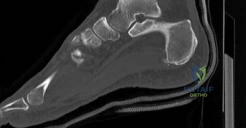 Fig-39: Follow-up AP radiograph at 9 months post-op, demonstrating continued healing.
Fig-39: Follow-up AP radiograph at 9 months post-op, demonstrating continued healing. Fig-40: Follow-up lateral radiograph at 9 months post-op.
Fig-40: Follow-up lateral radiograph at 9 months post-op.
Strengthening and Full Weight-Bearing (6-12+ weeks)
- Radiographic Confirmation: Radiographs are repeated, typically at 6 weeks and 12 weeks, to assess fracture healing. Clinical union must be present before full weight-bearing.
- Discontinuation of Boot: Once radiographic and clinical signs of union are evident, the walking boot can be gradually weaned.
- Progressive Weight-Bearing: Full weight-bearing (FWB) is allowed once union is confirmed.
- Advanced Strengthening: Progress to more aggressive strengthening exercises, including calf raises, balance and proprioception training (e.g., wobble board), and single-leg stance exercises.
- Gait Training: Focus on normal gait mechanics.
- Cardiovascular Fitness: Non-impact cardiovascular activities (e.g., cycling, swimming) are encouraged.
 Fig-41: Follow-up AP radiograph at 1 year post-op, showing complete fracture union.
Fig-41: Follow-up AP radiograph at 1 year post-op, showing complete fracture union. Fig-42: Follow-up lateral radiograph at 1 year post-op, confirming union.
Fig-42: Follow-up lateral radiograph at 1 year post-op, confirming union. Fig-43: Follow-up oblique radiograph at 1 year post-op.
Fig-43: Follow-up oblique radiograph at 1 year post-op.
Return to Activity and Long-Term Follow-Up (3-12 months and beyond)
- Return to Activity: Gradual return to light recreational activities, progressing to sports-specific training once strength, flexibility, and proprioception are fully restored. High-impact activities are typically delayed until 6-12 months post-op, depending on fracture severity and healing.
- Hardware Removal: Symptomatic hardware may be considered for removal after 12-18 months, once the fracture is fully healed and remodeled. This decision is made on a case-by-case basis.
 Fig-44: Final follow-up AP radiograph after hardware removal.
Fig-44: Final follow-up AP radiograph after hardware removal. Fig-45: Final follow-up lateral radiograph after hardware removal, demonstrating good bone healing and alignment.
Fig-45: Final follow-up lateral radiograph after hardware removal, demonstrating good bone healing and alignment.
- Long-Term Monitoring: Patients should be counseled on the risk of post-traumatic arthritis and monitored for long-term complications.
- Fig-47: Clinical photograph of the ankle and leg at the final follow-up, showing good cosmetic and functional outcome.
 Fig-48: Clinical photograph showing good range of motion at final follow-up.
Fig-48: Clinical photograph showing good range of motion at final follow-up.- Fig-49: Another clinical photograph illustrating good ankle dorsiflexion.
 Fig-50: Clinical photograph demonstrating excellent plantarflexion.
Fig-50: Clinical photograph demonstrating excellent plantarflexion.
Summary of Key Literature and Guidelines
The management of distal tibia fractures has evolved significantly, driven by advancements in surgical techniques, implant technology, and a deeper understanding of soft tissue biology. Current literature and clinical guidelines emphasize a patient-centered, evidence-based approach.
Staged Management and Soft Tissue Considerations
The consensus in high-energy, comminuted, or open distal tibia fractures, particularly pilon fractures, favors a staged approach. Initial management with irrigation and debridement (for open fractures), temporary spanning external fixation, and delayed definitive internal fixation has been shown to significantly reduce the incidence of soft tissue complications and deep infection compared to immediate ORIF in the acute setting with compromised soft tissues. The external fixator provides stability, reduces pain, and allows for soft tissue rest and swelling resolution (the "wrinkle sign" is a common clinical indicator for readiness for definitive surgery).
Role of External Fixation
While primarily a temporizing measure, external fixation can sometimes be used as definitive treatment, particularly in severely contaminated open fractures, patients unfit for internal fixation, or those with significant bone loss requiring bone transport. Hybrid external fixators (Ilizarov type) offer good stability and allow for precise manipulation of fragments, but are associated with pin tract infections and prolonged patient discomfort.
Advantages of Locking Plates
The introduction of locking plate technology has revolutionized the treatment of distal tibia fractures. Locking compression plates (LCPs) provide fixed-angle constructs, offering superior angular stability compared to conventional plates, especially in comminuted metaphyseal fractures and osteoporotic bone. This stability allows for earlier mobilization and reduced rates of nonunion and loss of reduction. Minimally invasive plate osteosynthesis (MIPO) techniques, utilizing locking plates, have gained traction for appropriate fracture patterns, aiming to minimize further soft tissue stripping and preserve periosteal blood supply. However, MIPO has limitations in complex intra-articular fractures where direct articular visualization and reduction are paramount.
Reduction Strategies
Anatomical reduction of the articular surface remains the primary goal in pilon fractures to prevent post-traumatic arthritis. Ligamentotaxis, direct visualization through limited arthrotomy, and external fixator-assisted reduction are all valid strategies. The role of the fibula as a length and rotation guide is consistently emphasized across the literature; fibular fixation typically precedes tibial fixation.
Outcomes and Predictive Factors
Despite optimal surgical management, outcomes for high-energy distal tibia fractures can be guarded. Post-traumatic arthritis, nonunion, and malunion remain significant challenges. Factors associated with poorer outcomes include severe comminution, extensive soft tissue injury (higher Gustilo-Anderson grades), older age, comorbidities (e.g., diabetes, smoking), and residual articular incongruity. Functional outcomes, often assessed using validated scores, demonstrate that while many patients return to pre-injury activities, a considerable number experience residual pain, stiffness, and functional limitations.
Future Directions
Research continues into optimizing biomaterials, plate designs, and biological augmentation (e.g., bone morphogenetic proteins, platelet-rich plasma) to improve healing rates and reduce complications. Advanced imaging techniques and navigation systems are also being explored to enhance reduction accuracy. The long-term role of total ankle arthroplasty as a salvage procedure for post-traumatic arthritis is also a growing area of interest.
The case presented illustrates a typical clinical scenario for a distal tibia fracture with articular extension, highlighting the necessity for prompt initial management, thorough imaging, staged surgical planning, and a comprehensive rehabilitation strategy. Mastery of these principles is essential for any orthopedic surgeon treating these challenging injuries.
Clinical & Radiographic Imaging