Masterclass: Intramedullary Nailing of Tibial Fractures – A Comprehensive Intraoperative Guide

Key Takeaway
This masterclass provides an exhaustive, real-time guide to tibial intramedullary nailing. Fellows will learn comprehensive surgical anatomy, precise patient positioning, and granular, step-by-step intraoperative execution. We cover critical neurovascular risks, instrument use, hardware application, and rationale, alongside extensive pearls, pitfalls, and postoperative management, ensuring a deep understanding of this essential procedure.
Comprehensive Introduction and Patho-Epidemiology
The management of tibial shaft fractures has undergone a profound evolution, transitioning from the era of prolonged cast immobilization to the modern standard of intramedullary nailing (IMN). As the most commonly fractured long bone, the tibia presents a unique biomechanical and biological challenge due to its subcutaneous anteromedial border, tenuous blood supply, and susceptibility to high-energy trauma. Intramedullary nailing has emerged as the unequivocal gold standard for displaced diaphyseal fractures, offering load-sharing biomechanics, preservation of the extraosseous blood supply, and the facilitation of early mobilization. The transition from Küntscher’s initial unreamed, unlocked V-nails to contemporary statically locked, anatomically contoured titanium and steel alloys represents a triumph of modern orthopedic engineering.
The epidemiology of tibial fractures dictates a bimodal distribution, profoundly influencing our surgical decision-making. High-energy mechanisms, such as motor vehicle collisions and pedestrian-struck incidents, predominantly affect young males and are frequently associated with severe soft tissue compromise, comminution, and concomitant polytrauma. Conversely, low-energy torsional mechanisms, such as ground-level falls, are increasingly prevalent in the osteoporotic elderly population, presenting distinct challenges regarding implant purchase and bone stock. Understanding this epidemiological dichotomy is critical, as the energy imparted to the limb directly correlates with the risk of open fractures, compartment syndrome, and long-term sequelae such as delayed union or osteomyelitis.
Historically, the indications for tibial IMN were strictly confined to the diaphyseal isthmus. However, with the advent of multi-planar proximal and distal locking options, extreme-angle screws, and the refinement of the suprapatellar approach, the indications have expanded dramatically. We now routinely employ IMN for complex proximal quarter and distal quarter extra-articular metaphyseal fractures, and even in cases with simple, non-displaced intra-articular extensions. This expansion, while mechanically advantageous, demands an unparalleled understanding of deforming muscle forces and meticulous intraoperative reduction techniques, as the nail no longer benefits from the "interference fit" provided by the narrow diaphyseal canal.
Despite these advancements, we must critically acknowledge the persistent morbidities associated with the procedure. Anterior knee pain remains the Achilles heel of tibial IMN, reported in up to 58% of patients post-operatively. This pain is classically anterior, exacerbated by kneeling or ascending stairs, and often activity-limiting. While the exact etiology remains multifactorial—implicating iatrogenic injury to the infrapatellar branch of the saphenous nerve, Hoffa’s fat pad fibrosis, or proximal hardware prominence—it is notable that nearly half of these patients experience symptomatic relief following implant removal after radiographic union. Our objective in this masterclass is to dissect the nuances of flawless execution, minimizing these inherent complications while optimizing anatomical restoration and functional recovery.
Detailed Surgical Anatomy and Biomechanics
Mastery of tibial intramedullary nailing is inextricably linked to a profound, three-dimensional comprehension of proximal tibial osteology and the surrounding soft tissue envelope. The proximal tibia is a complex, asymmetric, triangular structure. Crucially, the medullary canal is not collinear with the anatomic axis of the proximal metaphysis; rather, it possesses a slight lateral and posterior offset. The proximal medial cortex is obliquely oriented to the frontal plane, creating a significant geometric challenge. If a starting point is placed too medially or even centrally, the rigid anterior medial metaphyseal cortex will inevitably deflect the guidewire and subsequent reamers laterally and posteriorly, resulting in the dreaded iatrogenic valgus and procurvatum deformity.

This inherent anatomical bias mandates an uncompromising adherence to a lateral starting point. The ideal entry portal is located slightly medial to the lateral tibial eminence, precisely in line with the anatomic axis of the medullary canal on the anteroposterior (AP) radiograph, and immediately extra-articular, anterior to the articular margin on the lateral radiograph. The anterior tibial crest, a prominent subcutaneous landmark, serves as a reliable clinical reference for the true sagittal plane of the tibia, guiding our initial trajectory. Failure to respect this complex proximal morphology, particularly in proximal third fractures where the canal cannot guide the nail, is the primary source of malalignment.
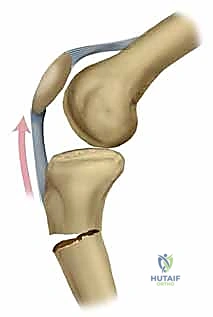
The muscular deforming forces acting upon the fractured tibia must be anticipated and neutralized during reduction. In proximal third fractures, the patellar tendon exerts a powerful anterior translational and extensor force on the proximal fragment. Simultaneously, the hamstring insertions (pes anserinus medially and biceps femoris laterally) flex the distal segment, while the anterior compartment musculature originating from Gerdy’s tubercle pulls the distal segment into valgus and shortening. This combination creates the classic "valgus and apex anterior (procurvatum)" deformity. Overcoming these vectors requires strategic patient positioning, such as the semi-extended position, and the judicious use of intraoperative blocking (Poller) screws to artificially narrow the metaphyseal canal and direct the nail trajectory.
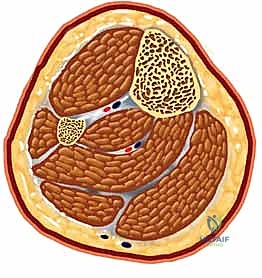
Finally, the neurovascular anatomy demands meticulous respect, particularly during distal interlocking. The anterior neurovascular bundle, comprising the anterior tibial artery and the deep peroneal nerve, courses intimately along the anterior interosseous membrane before transitioning to the anterior aspect of the distal tibia. When placing anterior-to-posterior (AP) distal interlocking screws, this bundle is at significant risk of iatrogenic penetration. A critical surgical pearl to mitigate this risk involves the internal rotation of the leg or the nail construct prior to drilling. This maneuver safely shifts the neurovascular structures laterally, away from the direct trajectory of the drill bit and screw, ensuring safe passage and preventing catastrophic vascular compromise or foot drop.
Exhaustive Indications and Contraindications
The decision to proceed with intramedullary nailing of the tibia requires a sophisticated algorithm balancing fracture morphology, soft tissue integrity, patient physiology, and systemic injury burden. IMN is the definitive treatment of choice for the vast majority of displaced, closed diaphyseal fractures, offering superior biomechanical stability compared to non-operative casting, with significantly lower rates of malunion and joint stiffness. Furthermore, in the context of open diaphyseal fractures (Gustilo-Anderson Types I, II, and IIIA), reamed IMN following meticulous surgical debridement has proven superior to external fixation, demonstrating lower rates of pin-tract infection and malalignment, provided the soft tissue envelope can be adequately managed or reconstructed.
In the polytraumatized patient, the application of IMN must be carefully contextualized within the principles of Damage Control Orthopedics (DCO) versus Early Total Care (ETC). For patients who are hemodynamically unstable, coagulopathic, or presenting with severe head or chest trauma, the physiological hit of intramedullary reaming—which temporarily increases intramedullary pressure and can embolize marrow fat—may be detrimental. In such extremis, rapid spanning external fixation is indicated. However, for the adequately resuscitated patient, early IMN of tibial fractures, particularly in the presence of an ipsilateral femur fracture (the "floating knee"), facilitates nursing care, upright positioning, and aggressive pulmonary toilet, significantly reducing the incidence of acute respiratory distress syndrome (ARDS).
Contraindications to tibial IMN, while relatively few, are absolute when present. The most critical absolute contraindication is the presence of an active intramedullary infection or gross, unmanageable contamination of the medullary canal, which precludes the introduction of hardware that would serve as a nidus for intractable osteomyelitis. Additionally, an intramedullary canal diameter of less than 6 mm (often seen in severe skeletal dysplasia or extreme pediatric cases) physically precludes the insertion of standard commercially available nails. In these rare instances, alternative fixation strategies such as compression plating or fine-wire circular external fixation must be employed.
Relative contraindications require nuanced surgical judgment. Severe soft tissue injuries where limb salvage is questionable (e.g., Gustilo Type IIIC with prolonged ischemia or massive crush injuries) may necessitate primary amputation rather than heroic internal fixation. Furthermore, preexisting angular deformities of the diaphysis or retained hardware that cannot be extracted may physically block nail passage. While significant intra-articular extension was historically a contraindication, modern techniques allow for the independent lag screw fixation of simple articular splits, followed by diaphyseal nailing, provided the articular block is anatomically restored and stable before the nail is introduced.
| Category | Indications | Contraindications |
|---|---|---|
| Absolute | Displaced closed diaphyseal fractures | Active intramedullary infection |
| Open diaphyseal fractures (Gustilo I, II, IIIA) | Canal diameter < 6 mm | |
| Ipsilateral femur fracture ("Floating Knee") | Unmanageable gross contamination | |
| Relative | Unstable metaphyseal fractures (proximal/distal) | Gustilo IIIC (if limb salvage is unviable) |
| Compartment syndrome (post-fasciotomy stabilization) | Pre-existing obstructive diaphyseal deformity | |
| Failure of non-operative management | Retained, irretrievable intramedullary hardware | |
| Polytrauma (Early Total Care candidates) | Complex, highly comminuted intra-articular fractures |
Pre-Operative Planning, Templating, and Patient Positioning
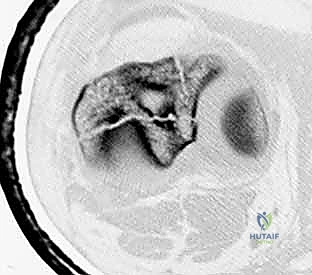
The success of a tibial IMN is largely dictated before the surgical incision is ever made. Meticulous preoperative planning begins with high-quality, orthogonal plain radiographs of the entire tibia and fibula, extending to include the knee and ankle joints. This is non-negotiable to rule out subtle intra-articular extensions or concomitant injuries, such as a Maisonneuve fracture or an ipsilateral femoral neck fracture. For complex metaphyseal fractures, an axial CT scan with sagittal and coronal reconstructions is indispensable. CT imaging definitively maps fracture lines, identifies occult articular involvement, and guides the precise placement of independent interfragmentary lag screws prior to nail insertion.

Digital templating is a critical step that must not be bypassed. Utilizing orthogonal radiographs of the uninjured contralateral tibia provides a perfect anatomical template. The surgeon must measure the narrowest diameter of the isthmus on both the AP and lateral views to determine the appropriate nail diameter and to anticipate the necessity and extent of intramedullary reaming. Furthermore, the lateral radiograph is the most accurate modality for determining the precise nail length, measured from the proposed proximal entry point to the physeal scar of the distal tibia. Anticipating the required implant dimensions ensures the appropriate inventory is available, preventing catastrophic intraoperative delays.

Preoperative soft tissue and neurovascular assessment is paramount. The presence of fracture blisters, abrasions, or severe edema dictates the surgical timing. Operating through compromised skin exponentially increases the risk of deep infection. Continuous clinical monitoring for compartment syndrome is mandatory. If the patient is obtunded or the clinical exam is equivocal in the face of massive swelling, invasive compartment pressure monitoring is required. A delta pressure (diastolic blood pressure minus intracompartmental pressure) of less than 30 mm Hg is an absolute indication for emergent four-compartment fasciotomies, which should be performed concurrently with or immediately preceding the IMN.

Patient positioning sets the stage for the entire procedure and is heavily influenced by the fracture pattern and the chosen surgical approach (infrapatellar vs. suprapatellar). The traditional setup utilizes a fracture table with calcaneal skeletal traction. This provides excellent, sustained mechanical traction, which is invaluable for restoring length in highly comminuted or shortened fractures, particularly when surgical assistance is limited. However, the fracture table restricts knee flexion, making it suboptimal for proximal fractures where the extensor mechanism exerts a strong deforming force.
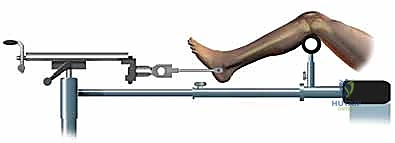
Alternatively, positioning the patient supine on a radiolucent flat table with the leg draped free has become the preferred method for many trauma surgeons, particularly when utilizing the suprapatellar approach. This setup allows for dynamic manipulation of the limb, facilitating the semi-extended position (15-20 degrees of flexion), which neutralizes the pull of the patellar tendon and dramatically simplifies the reduction of proximal third fractures. In this configuration, length and alignment are maintained using manual traction, a femoral distractor, or temporary external fixation pins placed strategically outside the planned path of the nail.


Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the proximal tibia has seen a paradigm shift with the popularization of the suprapatellar portal. While the traditional infrapatellar approaches (medial parapatellar, lateral parapatellar, or tendon-splitting) remain highly effective for midshaft and distal fractures, they require hyperflexion of the knee (often >90 degrees) to access the starting point. This hyperflexion exacerbates the pull of the extensor mechanism, driving proximal fractures into procurvatum. The suprapatellar approach, performed with the knee in 15-20 degrees of flexion, neutralizes this force. Through a 3-4 cm incision proximal to the superior pole of the patella, a specialized cannula is passed bluntly through the patellofemoral joint, protecting the articular cartilage, and landing directly on the ideal lateral starting point.


Regardless of the approach, establishing the perfectly trajectory for the starting guidewire is the most critical step of the operation. Under biplanar fluoroscopy, the entry point must be meticulously confirmed. On the AP view, it should reside slightly medial to the lateral tibial spine. On the lateral view, it must be exactly at the anterior margin of the articular surface. An awl or rigid entry reamer is advanced to open the proximal cortex. It is imperative that the trajectory of this opening instrument is collinear with the anatomic axis of the tibial shaft. Any deviation here will dictate the path of the guidewire, the reamers, and ultimately the nail, leading to unavoidable malalignment.


Once the entry portal is established, a ball-tipped guidewire is advanced down the medullary canal. In displaced fractures, closed reduction maneuvers must be employed to pass the wire into the distal fragment. This is where the true art of trauma surgery is demonstrated. If manual reduction is insufficient, the surgeon must utilize percutaneous joysticks, a femoral distractor, or blocking (Poller) screws. Poller screws are strategically placed in the metaphyseal bone of the concave side of the deformity. They act as artificial cortices, physically preventing the guidewire and nail from migrating into the path of least resistance, thereby forcing the implant into the center of the canal and correcting the angular deformity.


With the guidewire centrally located in the distal epiphysis (centered on the plafond on the AP, and centered in the distal metaphysis on the lateral), sequential intramedullary reaming commences. Reaming serves a dual purpose: it generates biologically active autogenous bone graft that is deposited at the fracture site, and it expands the canal to accommodate a larger, biomechanically superior nail. Reaming should be performed in 0.5 mm increments until cortical "chatter" is felt, indicating contact with the diaphyseal endosteum. The nail, typically 1.0 to 1.5 mm smaller than the final reamer, is then attached to the insertion jig and advanced over the guidewire.

The final phase is interlocking. Distal interlocking is typically performed first using a freehand fluoroscopic technique. Depending on the fracture proximity to the plafond, two or three multi-planar screws are placed to maximize stability. As noted previously, internal rotation of the limb is crucial when placing AP directed screws to protect the anterior neurovascular bundle. Following distal fixation, the fracture is compressed. The insertion jig is struck retrogradely (back-slapping) to close any diaphyseal gaps, preventing delayed union. Finally, proximal interlocking screws are placed through the targeting jig, securing the construct.



Complications, Incidence Rates, and Salvage Management
Despite rigorous technique, complications following tibial IMN are well-documented and require prompt, aggressive management. Malalignment remains a primary concern, particularly in metaphyseal fractures. Proximal third fractures notoriously drift into valgus and procurvatum, while distal third fractures tend toward varus. The incidence of malalignment (defined as >5 degrees of angulation) can approach 30% if meticulous reduction techniques, such as the suprapatellar approach and blocking screws, are not utilized. Salvage of a healed malunion requires a complex corrective osteotomy, whereas acute intraoperative recognition allows for immediate revision of the nail trajectory or the addition of supplemental plating.

Nonunion and delayed union are significant biological complications, occurring in 5% to 15% of cases, with higher rates observed in severe open fractures, heavy smokers, and cases with significant bone loss or inadequate mechanical stabilization. Clinically, patients present with persistent pain at the fracture site upon weight-bearing. Radiographically, a lack of bridging callus at 6 months defines a nonunion. The first-line salvage for an atrophic or oligotrophic nonunion is dynamization (removal of the static locking screws at the longer end of the nail) to allow axial micro-motion and stimulate callus formation. If dynamization fails, or in the presence of a hypertrophic nonunion, exchange nailing (removal of the nail, aggressive over-reaming by 2-3 mm, and insertion of a larger diameter nail) is highly effective, boasting union rates exceeding 90%.

Infection following IMN is a devastating complication, incidence ranging from 1% in closed fractures to over 15% in Gustilo Type III open fractures. Deep intramedullary infection presents with escalating pain, erythema, wound drainage, and elevated inflammatory markers (ESR, CRP). The management is unequivocally surgical. The intramedullary nail must be removed, and the canal aggressively reamed and irrigated (the Reamer-Irrigator-Aspirator or RIA system is excellent for this). The canal is then filled with an antibiotic-impregnated cement spacer (often molded over a chest tube or a dedicated nail mold) to deliver high local concentrations of antibiotics while maintaining length and stability. Systemic culture-directed antibiotics are required for 6-12 weeks, followed by definitive reconstruction once the infection is eradicated.


Anterior knee pain, as discussed, is the most frequent subjective complaint, affecting up to 58% of patients. While often self-limiting, it can severely impact the quality of life. The etiology is debated but is likely a combination of iatrogenic nerve injury, tendonitis, and fat pad scarring. Conservative management with NSAIDs, physical therapy, and targeted injections is the first line. If pain persists beyond radiographic union (typically >12-18 months post-op), hardware removal is indicated. Literature suggests that approximately 50-60% of patients will experience significant relief following nail extraction, though patients must be counseled that complete resolution is not guaranteed.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Anterior Knee Pain | 30% - 58% | Surgical approach, prominent hardware, nerve injury | PT, NSAIDs, eventual hardware removal after union |
| Malalignment (>5°) | 10% - 30% (Metaphyseal) | Poor starting point, un-neutralized muscle forces | Intra-op: Blocking screws. Post-op: Corrective osteotomy |
| Nonunion / Delayed Union | 5% - 15% | Smoking, open fractures, inadequate stability | Dynamization, Exchange Nailing with over-reaming |
| Deep Infection | 1% (Closed) - 15% (Open) | Soft tissue compromise, gross contamination | Nail removal, aggressive debridement, antibiotic spacer |
| Compartment Syndrome | 2% - 9% | High-energy crush, reperfusion injury | Emergent 4-compartment fasciotomy |
Phased Post-Operative Rehabilitation Protocols
The immediate post-operative phase (0-2 weeks) is focused on wound healing, edema control, and the prevention of deep vein thrombosis. The biomechanical advantage of a locked intramedullary nail is its load-sharing capacity, which, in the context of stable diaphyseal fractures, allows for immediate weight-bearing as tolerated. However, the surgeon must tailor the weight-bearing prescription to the specific fracture morphology. In highly comminuted, length-unstable fractures, or complex metaphyseal fractures requiring supplemental fixation, a period of restricted weight-bearing (e.g., toe-touch only) for 4-6 weeks may be mandated to prevent hardware failure or loss of reduction. Early active and passive range of motion of the knee and ankle is initiated immediately to prevent arthrofibrosis.
During the early rehabilitation phase (2-6 weeks), physical therapy intensifies. The primary goals are the restoration of full, symmetric knee extension and the activation of the quadriceps mechanism, which often suffers profound inhibition following surgical trauma to the extensor mechanism. Patellar mobilization techniques are critical to prevent infrapatellar contractures. Patients are transitioned from assistive devices (crutches/walkers) to independent ambulation as their pain and radiographic healing dictate. The surgeon monitors the soft tissue envelope closely, removing sutures or staples at the 2-to-3-week mark once the incisions are completely sealed.
The intermediate phase (6-12 weeks) marks the transition to functional restoration. Radiographically, we expect to see the development of bridging callus bridging the fracture site. As secondary bone healing progresses, the mechanical load is gradually transferred from the titanium nail back to the biological bone. Patients are encouraged to normalize their gait mechanics and begin closed-kinetic chain strengthening exercises (e.g., leg presses, shallow squats). Proprioceptive training and balance exercises are introduced to prepare the limb for the unpredictable loads of daily living and eventual return to sport.
The advanced return to function phase (3-6+ months) is highly individualized. Return to high-impact activities or heavy manual labor requires clinical evidence of pain-free full weight-bearing and radiographic evidence of solid union across at least three cortices on orthogonal views. For patients experiencing the aforementioned chronic anterior knee pain, this is the phase where discussions regarding hardware removal are initiated. It is imperative that the surgeon confirms robust, mature cortical bridging before extracting the nail to prevent the catastrophic complication of a re-fracture through a biologically immature union site.
Summary of Landmark Literature and Clinical Guidelines
The contemporary practice of tibial intramedullary nailing is heavily guided by rigorous, prospective, randomized controlled trials. The landmark SPRINT (Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures) trial definitively shaped our understanding of reaming. This massive international study demonstrated that for closed tibial fractures, reamed IMN significantly reduced the risk of nonunion and the need for secondary
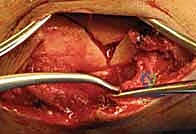
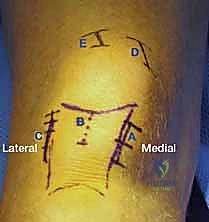
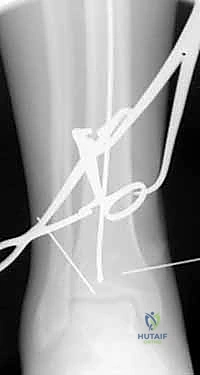
Clinical & Radiographic Imaging Archive