

Introduction and Epidemiology
Distal femur fractures represent a complex and challenging subset of lower extremity trauma, demanding a comprehensive understanding for optimal management. These fractures involve the metadiaphyseal and intra-articular regions of the distal femur, proximal to the knee joint. Their incidence, mechanisms, and patient demographics exhibit distinct patterns that significantly influence treatment paradigms and prognoses.
Distal femoral fractures account for approximately 7% of all femur fractures. When considering only femoral shaft fractures, excluding hip fractures, this proportion rises substantially, with one-third involving the distal portion. This highlights their clinical significance within the spectrum of femoral trauma.
A characteristic bimodal age distribution is observed for distal femur fractures. The first peak occurs in younger, often active males, typically resulting from high-energy mechanisms. These include severe motor vehicle or motorcycle accidents, falls from significant heights, or high-impact sports injuries. Such injuries frequently present with greater comminution, soft tissue damage, and a higher propensity for open fractures. The second peak occurs in elderly women, predominantly stemming from low-energy falls. These fractures often occur in the setting of osteoporotic bone, which can influence fracture patterns, comminution, and implant choice, as well as the patient's overall medical comorbidities and functional demands. The overall incidence demonstrates a 1:2 ratio of men to women, reflecting the influence of osteoporosis in the older female demographic.
Open fractures, characterized by a communication between the fracture site and the external environment, occur in 5% to 10% of all distal femur fractures. The presence of an open fracture significantly increases the risk of infection, prolongs healing time, and necessitates urgent surgical débridement and antibiotic prophylaxis in addition to fracture stabilization. The associated soft tissue envelope around the distal femur is relatively thin, particularly anteriorly and laterally, making it vulnerable in high-energy trauma.
Surgical Anatomy and Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the distal femur is paramount for accurate reduction, stable fixation, and successful patient outcomes. The distal femur encompasses both the supracondylar and condylar regions, forming a critical load-bearing segment of the lower limb.
Gross Anatomy of the Distal Femur
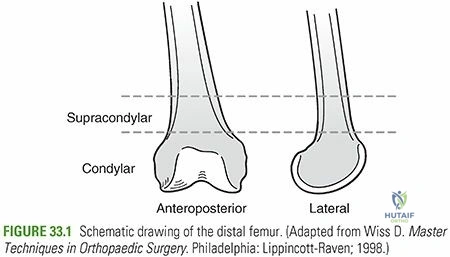
The supracondylar area of the femur is defined as the zone between the femoral condyles and the junction of the metaphysis with the femoral shaft. This region typically spans the distal 10 to 15 cm of the femur. Proximally, the femoral shaft is cylindrical, gradually broadening distally to form the two prominent, curved femoral condyles. These condyles are separated posteriorly and distally by the intercondylar groove (or notch).
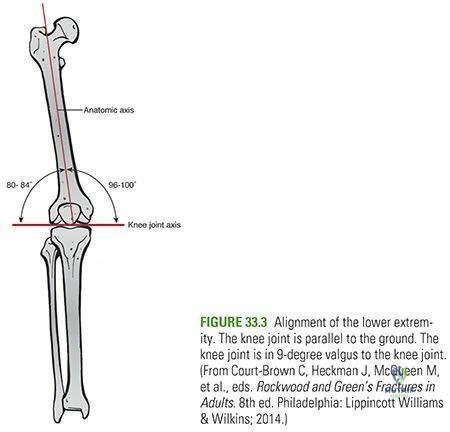
The medial femoral condyle is notably more distal and more convex than the lateral femoral condyle. This anatomical asymmetry is crucial as it contributes to the physiological valgus alignment of the femur, typically 5-7 degrees, which allows the knee joint to lie in a relatively horizontal plane relative to the ground during bipedal stance. This valgus angle is essential for understanding reduction goals, particularly for extra-articular supracondylar fractures.
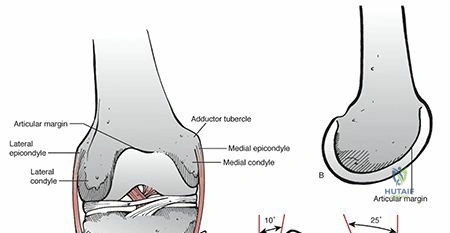
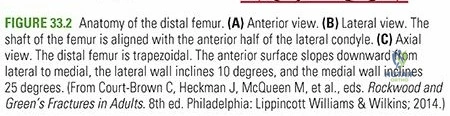
When viewing the lateral aspect of the distal femur, the femoral shaft is aligned with the anterior half of the lateral condyle. This relationship is important for plate positioning and trajectory, particularly in the sagittal plane, to avoid implant prominence or impingement with patellofemoral articulation.
Muscular and Ligamentous Attachments
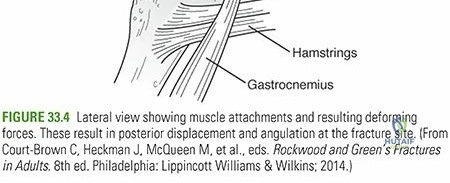
Numerous powerful muscles and crucial ligaments influence fracture displacement and guide reduction maneuvers. The gastrocnemius muscle, originating from the posterior aspects of both femoral condyles, exerts a significant deforming force. In supracondylar fractures, the proximal fragment is often drawn into varus by the adductor musculature and shortened by the hamstring and quadriceps groups. Concurrently, the distal condylar fragment is typically pulled into apex posterior angulation and flexion by the gastrocnemius, complicating closed reduction efforts and often necessitating direct manipulation. The plantarflexion moment created by the gastrocnemius is particularly strong.
The collateral ligaments (medial collateral ligament, MCL; lateral collateral ligament, LCL) originate from the epicondyles of the femur and insert onto the tibia and fibula, respectively. These provide critical varus-valgus stability to the knee joint. The cruciate ligaments (anterior cruciate ligament, ACL; posterior cruciate ligament, PCL) originate from within the intercondylar notch. Intra-articular fractures (condylar and intercondylar) can compromise these ligamentous structures, either directly through fracture lines or indirectly through avulsion injuries.
Vascular and Neural Structures
The neurovascular structures posterior to the distal femur are highly vulnerable in high-energy trauma or during surgical intervention. The popliteal artery and vein, along with the tibial nerve and common peroneal nerve, pass directly posterior to the distal femur in the popliteal fossa. Significant displacement of distal femur fractures, particularly posterior displacement, carries a substantial risk of popliteal artery injury, which can lead to limb-threatening ischemia. A thorough neurovascular examination, including ankle-brachial index (ABI) measurements, is mandatory both pre-operatively and post-operatively. During surgical approaches, meticulous care must be taken to protect these structures, often requiring careful dissection and retraction.
Bone Quality and Biomechanics
The distal femur metaphysis is characterized by a relatively thin cortex and a significant amount of cancellous bone. This makes it susceptible to comminution, especially in osteoporotic bone. The transition from the cylindrical diaphysis to the broad metaphyseal-epiphyseal segment creates a region of stress concentration, explaining why this area is prone to fracture. The presence of pre-existing hardware, such as knee arthroplasty components, further complicates fracture patterns and fixation strategies, particularly in periprosthetic fractures.
The mechanical axis of the lower limb passes through the center of the hip, knee, and ankle joints. Restoring this axis, along with proper rotational and sagittal plane alignment, is a primary goal of surgical fixation to prevent long-term functional deficits and post-traumatic arthritis.
Indications and Contraindications
The decision-making process for managing distal femur fractures involves a careful consideration of fracture characteristics, patient factors, and available resources. Most distal femur fractures in skeletally mature individuals are best managed operatively to achieve stable fixation, restore articular congruity, and facilitate early mobilization.
Operative Indications
Absolute indications for operative management include open fractures, fractures with associated vascular injury, compartment syndrome, and irreducible fractures. Relative indications encompass the vast majority of displaced and unstable distal femur fractures. The primary goals of operative management are to restore articular anatomy, axial alignment, length, and rotation, allowing for early range of motion to prevent knee stiffness.
Non-Operative Indications
Non-operative treatment is reserved for a select group of patients and fracture patterns. These include:
* Minimally displaced, stable fractures: Especially in the elderly or those with severe comorbidities where surgical risks outweigh potential benefits.
* Non-ambulatory patients: In patients with very limited functional demands, comfort care may supersede aggressive surgical intervention.
* Medically unstable patients: Patients with severe, uncontrolled comorbidities where anesthesia and surgery pose an unacceptably high risk to life.
* Palliative care: In some terminal conditions, comfort-based non-operative care may be chosen.
* Contaminated open fractures: In rare instances, severe contamination and soft tissue loss may necessitate initial external fixation and delayed definitive management.
The following table summarizes the general indications for operative versus non-operative management:
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | Displaced intra-articular fractures | Minimally displaced, stable extra-articular fractures |
| Displaced extra-articular fractures with instability | ||
| Fracture Morphology | Comminuted fractures | Nondisplaced or minimally displaced hairline fractures |
| Articular step-off > 2mm | ||
| Associated Injuries | Open fractures | |
| Neurovascular compromise | ||
| Compartment syndrome | ||
| Patient Factors | Young, active patients with high functional demands | Severely medically unstable patients |
| Skeletally mature individuals | Non-ambulatory patients with limited functional demands | |
| Terminal illness requiring palliative care | ||
| Soft Tissue Status | Adequate soft tissue envelope for surgical approach | Severe soft tissue compromise precluding internal fixation |
| Other | Polytrauma patients requiring early mobilization |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful distal femur fracture management, minimizing intraoperative complications and optimizing outcomes.
Imaging and Assessment
- Radiographs: Standard AP and lateral views of the femur and knee are essential. Oblique views and traction views can be helpful to delineate fracture patterns, especially articular involvement. Full-length femurs are critical for assessing overall alignment, pre-existing deformities, and planning implant length.
- Computed Tomography (CT) Scan: A fine-cut CT scan with 2D and 3D reconstructions is indispensable for understanding intra-articular involvement, articular depression, comminution, and fragment orientation. This information directly guides reduction strategy and implant selection.
- Vascular Assessment: In high-energy trauma, consider an ankle-brachial index (ABI). If diminished or if clinical suspicion for vascular injury exists (e.g., expanding hematoma, pulse deficit), a CT angiogram should be performed pre-operatively.
- Soft Tissue Assessment: Evaluate for open wounds, fracture blisters, and significant swelling. Delaying definitive fixation may be necessary to allow for soft tissue swelling to subside, often managed with temporary external fixation.
Templating and Implant Selection
Detailed templating is crucial for anticipating implant size, length, and screw trajectories.
* Plate Fixation: Long locking plates (e.g., LISS, LCP distal femoral plates) are typically used. Consider plate length (spanning 6-8 diaphyseal diameters), screw trajectories, and specific plate designs for the distal femur (e.g., anatomical contour). Pre-contouring plates is often necessary for optimal fit.
* Intramedullary Nailing: Retrograde intramedullary nailing is an option for certain extra-articular or simple articular patterns. Pre-operative assessment of the intercondylar notch width is critical to ensure nail passage without iatrogenic fracture.
* External Fixation: Used for temporary stabilization in polytrauma, open fractures, or those with severe soft tissue compromise.
Patient Positioning
Patient positioning must allow for excellent fluoroscopic imaging in both AP and lateral planes, surgical access, and intraoperative manipulation of the fracture.
* Supine Position: This is the most common position. The patient is placed on a radiolucent table.
* A bump or blanket roll can be placed under the ipsilateral hip to allow for easier access to the lateral aspect of the distal femur.
* A fracture table with skeletal traction through a distal femoral or proximal tibial pin can be used, particularly for reduction and length restoration. However, it can restrict intraoperative imaging and direct manipulation.
* Alternatively, a bolster under the ipsilateral knee (allowing knee flexion) can help relax the gastrocnemius, facilitating reduction of the distal fragment.
* Lateral Decubitus Position: Less common but can be useful for complex posterior plating or when concurrent injuries necessitate.
* Draping: Standard sterile draping allows for exposure from the distal thigh to the foot. The knee should be free-draped to allow for intraoperative manipulation and assessment of range of motion.
Detailed Surgical Approach and Technique
The choice of surgical approach and technique for distal femur fractures is dictated by the fracture pattern (extra-articular vs. intra-articular, comminution), soft tissue status, and surgeon preference. The goals remain anatomical reduction, stable fixation, and preservation of the soft tissue envelope.
Lateral Parapatellar Approach for Lateral Plating
This is the most common approach for distal femur fractures, particularly for locking plate application.
Incision and Dissection
- Skin Incision: A longitudinal incision is made along the lateral aspect of the distal femur. The length depends on the fracture comminution and anticipated plate length, typically extending from proximal to the fracture site to just proximal to the lateral epicondyle. The incision can be slightly curved anteriorly or posteriorly depending on surgeon preference and plate trajectory.
- Fascial Incision: The fascia lata is incised longitudinally. The vastus lateralis muscle is identified.
- Internervous Plane: The approach to the lateral distal femur utilizes an internervous plane. The vastus lateralis muscle is retracted anteriorly, exposing the lateral intramuscular septum. The septum is then incised, or elevated from the femoral shaft, to expose the lateral femoral cortex. This plane typically involves separating the vastus lateralis (innervated by the femoral nerve) from the biceps femoris (innervated by the sciatic nerve), or more precisely, elevating the vastus lateralis from the lateral femoral shaft. The ascending branch of the lateral femoral circumflex artery and vein may be encountered proximally and should be ligated or cauterized.
Fracture Reduction
- Length and Alignment Restoration: Traction, either manual or via a fracture table, is crucial. For supracondylar fractures, the gastrocnemius pull often causes apex posterior angulation of the distal fragment. Flexing the knee to 60-90 degrees relaxes the gastrocnemius, facilitating reduction.
- Indirect Reduction: Primarily, indirect reduction techniques are preferred to minimize further soft tissue stripping.
- External Fixator as a Reduction Tool: A temporary external fixator can be applied from the proximal femur to the tibia to restore length and approximate alignment.
- Distractor/Femoral Condyle Clamp: Large pointed reduction clamps (e.g., Verbrugge clamps) or a femoral distractor can be used to achieve length and reduce fragments.
- Plate as a Reduction Aid: The definitive locking plate can sometimes be used as a reduction jig, slid submuscularly and provisionally fixed proximally, then used to "push" or "pull" the distal fragment into alignment.
- Direct Reduction (for articular fragments): For intra-articular fractures (condylar or intercondylar), direct visualization and reduction of articular fragments are often necessary.
- Arthrotomy: A limited medial or lateral parapatellar arthrotomy can be performed to directly visualize the articular surface.
- Temporary K-wires: Small articular fragments are reduced under direct vision and provisionally fixed with K-wires.
- Reduction Forceps: Small pointed reduction forceps are used to manipulate and compress articular fragments.
- Bone Grafts: For articular impaction or bone loss, structural bone grafts (autograft or allograft) may be necessary to support the articular surface.
Fixation with Locking Plate
- Plate Positioning: The plate is slid submuscularly (minimally invasive plate osteosynthesis, MIPO) if possible, to preserve the periosteal blood supply. It is positioned along the lateral aspect of the distal femur, ensuring it is centered over the lateral femoral condyle distally and centered on the shaft proximally. Proper rotation of the plate is crucial to match the anatomical twist of the femur.
- Distal Fixation:
- Multiple locking screws (typically 4-6) are inserted into the distal fragment. These screws should engage sufficient bone stock and avoid articular penetration. Use fluoroscopy in multiple planes to confirm screw length and position.
- Aim for bicortical fixation where possible without violating the joint.
- The most distal screws should aim into the subchondral bone for maximum purchase.
- Proximal Fixation:
- After confirming alignment (length, rotation, angulation) with fluoroscopy, locking screws are inserted into the proximal fragment.
- A minimum of 3-4 bicortical locking screws are generally recommended in the diaphysis.
- Avoid placing screws too close to the fracture site proximally in a highly comminuted zone to prevent stress risers.
- Lag Screws (if indicated): For specific fracture patterns with amenable oblique components, a lag screw can be inserted through the plate or independently to achieve interfragmentary compression before locking screws are placed.
- Biomechanical Principles: The concept of "biological fixation" emphasizes indirect reduction and maintaining the soft tissue attachments to the fracture fragments. The plate acts as an internal fixator or bridging plate, with locking screws providing angular stability rather than compression. This construct allows for relative stability and callus formation.
Retrograde Intramedullary Nailing
Retrograde intramedullary nailing is a viable option for certain extra-articular supracondylar fractures (AO/OTA 33-A1, 33-A2) and some simple intra-articular patterns (33-C1) without significant articular comminution. It offers a more load-sharing construct and may be advantageous for highly osteoporotic bone.
Technique
- Patient Positioning: Supine with the knee flexed to 60-90 degrees, often over a bolster or a fracture table allowing knee flexion.
-
Entry Portal: A small incision is made just proximal to the patella, either through the patellar tendon (transpatellar) or paramedially/paralaterally (parapatellar). The aim is to create an entry portal within the intercondylar notch, slightly medial to the center in the AP plane and just anterior to the PCL origin in the lateral plane.
-
Reaming and Nailing: The medullary canal is reamed sequentially to the desired nail diameter. The nail is then advanced retrograde across the fracture site.
- Distal Locking: Multiple locking screws (typically 2-4) are inserted proximally from the nail end into the distal fragment. Careful fluoroscopic guidance is necessary to avoid joint penetration.
- Proximal Locking: Standard proximal locking screws are inserted through the nail jig into the proximal femoral shaft.
Medial or Anterior Approaches
- Medial Approach: Less common but may be necessary for specific fracture patterns involving the medial condyle or for bicondylar fixation requiring a medial plate. The internervous plane is between the vastus medialis (femoral nerve) and the adductor magnus (obturator nerve). Care must be taken to protect the saphenous nerve and artery.
- Anterior Approach (e.g., extensor mechanism splitting): Reserved for very complex articular fractures or revision surgeries where maximal articular visualization is required. This approach carries a higher risk of quadriceps dysfunction and patellofemoral issues.
External Fixation
Primarily used for temporary stabilization in trauma settings:
* Damage Control Orthopaedics: For polytrauma patients requiring stabilization prior to definitive internal fixation.
* Open Fractures: To stabilize the fracture after initial débridement, allowing for soft tissue healing before internal fixation.
* Severe Soft Tissue Compromise: When definitive internal fixation is contraindicated due to significant swelling, blisters, or skin loss.
Pins are usually placed proximally in the femoral shaft and distally in the tibia or calcaneus, avoiding the zone of injury and anticipated definitive fixation.
Complications and Management
Distal femur fractures are associated with a significant rate of complications, which can profoundly impact functional outcomes. Proactive identification and appropriate management are critical.
| Complication | Incidence | Management Strategies |
|---|---|---|
| Nonunion | 5-20% | Hypertrophic: Revision surgery with rigid fixation (e.g., larger plate, longer screws, IM nail), bone grafting. Atrophic: Revision surgery, debridement of fibrous tissue, potent bone graft (autograft), rigid fixation, biological adjuncts (e.g., BMPs). |
| Malunion | Up to 20% | Mild/Asymptomatic: Observation. Symptomatic (pain, gait disturbance, arthritis): Corrective osteotomy (opening/closing wedge), often requiring revision fixation. |
| Infection | 2-10% (higher in open) | Superficial: Oral antibiotics, local wound care. Deep (acute): Urgent irrigation and débridement, IV antibiotics (culture-guided), retention of stable hardware if possible, exchange nailing. Deep (chronic): Debridement, hardware removal, long-term antibiotics, staged reconstruction (e.g., external fixator, then definitive fixation), possible muscle flap. |
| Knee Stiffness / Loss of ROM | 20-50% | Early aggressive rehabilitation. Persistent: Manipulation under anesthesia (MUA), arthroscopic or open arthrofibrosis release. |
| Implant Failure | 5-15% | Revision surgery with stronger fixation (e.g., revision plate, conversion to IM nail or vice versa), addressing underlying cause (nonunion, malreduction, poor bone quality). |
| Neurovascular Injury | <1-5% | Acute: Immediate surgical exploration, vascular repair (interposition graft), nerve repair (primary, grafting), fasciotomy for compartment syndrome. Chronic: Nerve grafting, tendon transfers for functional deficits. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | 5-15% / 1-2% | Chemical prophylaxis (LMWH, fondaparinux). Mechanical prophylaxis (sequential compression devices). Confirmed DVT: Therapeutic anticoagulation. Confirmed PE: Therapeutic anticoagulation, critical care support. |
| Periprosthetic Fracture | Varies widely | Often requires specialized revision implants (e.g., hinged knee replacement, long stemmed components, modular plates) or conversion to arthrodesis/amputation in severe cases. |
| Painful Hardware | 10-30% | Symptomatic hardware removal after fracture union, typically 12-18 months post-op. |
Nonunion
Nonunion, defined as a lack of radiographic progression of healing after 6-9 months, or earlier if clear signs of failure are present, is a significant concern. Contributing factors include severe comminution, excessive soft tissue stripping, inadequate fixation stability, infection, and patient factors (e.g., smoking, poor nutrition, medical comorbidities). Management depends on the type of nonunion (hypertrophic vs. atrophic) and involves revision surgery, often with more rigid fixation, bone grafting, and correction of any malalignment or instability.
Malunion
Malunion occurs when the fracture heals in an unacceptable position, leading to residual angulation, rotation, or shortening. Even minor malalignment can significantly alter knee joint mechanics, leading to pain, instability, and accelerated osteoarthritis. Surgical correction via osteotomy may be indicated for symptomatic malunions.
Infection
Deep surgical site infection is a devastating complication, particularly with extensive hardware. Prevention includes meticulous sterile technique, appropriate antibiotic prophylaxis, thorough débridement of open fractures, and minimizing surgical time. Treatment involves aggressive surgical irrigation and débridement, culture-directed antibiotics, and often hardware retention if stable, or staged removal and re-implantation.
Knee Stiffness
Arthrofibrosis and loss of knee range of motion (ROM) are common sequelae, especially with intra-articular involvement and prolonged immobilization. Early, controlled ROM exercises are crucial. If severe stiffness persists, manipulation under anesthesia (MUA) or arthroscopic/open arthrolysis may be required.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is a critical component of successful recovery after distal femur fracture fixation, aiming to restore knee function, strength, and mobility while protecting the surgical repair. Protocols must be individualized based on fracture stability, fixation quality, bone quality, and patient comorbidities.
Phase I: Immediate Postoperative (Weeks 0-6)
Goals:
* Pain control and wound healing.
* Protect fracture fixation.
* Prevent complications (DVT, stiffness).
* Initiate early, controlled range of motion.
Weight Bearing:
* Touch-down weight bearing (TDWB) or non-weight bearing (NWB): Typically for 6-8 weeks, especially for comminuted fractures, osteoporotic bone, or unstable fixation. Weight bearing restrictions are lifted based on radiographic evidence of healing and clinical stability.
* Partial weight bearing (PWB): May be allowed earlier for very stable extra-articular fractures or retrograde nailing, depending on surgeon discretion.
Range of Motion (ROM):
* Continuous Passive Motion (CPM) machine: May be used in the immediate postoperative period, particularly for intra-articular fractures, to reduce stiffness and improve cartilage nutrition.
* Active-assisted and passive ROM: Initiate within pain tolerance. Goal for knee flexion is often 0-90 degrees by 4-6 weeks. Avoid resisted knee extension against gravity initially.
* Ankle pumps: To prevent DVT.
Exercises:
* Gluteal sets, quadriceps sets (gentle), hamstring curls (gentle).
* Upper body conditioning to aid mobility.
* Core stability exercises.
Phase II: Early Consolidation (Weeks 6-12)
Goals:
* Gradual increase in weight bearing.
* Improve knee ROM and strength.
* Restore normal gait patterns.
Weight Bearing:
* Progressive weight bearing (PWB to FWB): Initiated based on radiographic union and clinical assessment. Typically, 25% weight bearing initially, progressing to full weight bearing over several weeks.
* Use of crutches or a walker to maintain balance and support.
Range of Motion:
* Continue active and passive ROM exercises. Aim for >100-110 degrees of knee flexion.
* Scar massage and mobilization to prevent adhesions.
Exercises:
* Strengthening: Gentle isometric exercises progressing to isotonic, including quadriceps strengthening (e.g., knee extensions, leg presses with light resistance), hamstring curls, hip abduction/adduction.
* Proprioception: Single leg stance with support, balance exercises.
* Gait training: Focus on heel-toe progression and proper mechanics.
Phase III: Advanced Strengthening and Functional Recovery (Weeks 12-24)
Goals:
* Restore full knee ROM and strength.
* Regain balance and proprioception.
* Progress to sport-specific or activity-specific training.
Weight Bearing:
* Full weight bearing without assistive devices as tolerated.
Range of Motion:
* Achieve full, pain-free ROM.
Exercises:
* Progressive resistance exercises (PREs): Increase intensity and resistance for all major muscle groups of the lower extremity.
* Functional exercises: Squats, lunges, step-ups/downs, partial jumps (if appropriate).
* Agility training: Lateral shuffles, controlled pivots.
* Cardiovascular conditioning: Stationary cycling, swimming, elliptical trainer.
Phase IV: Return to Activity (Months 6+)
Goals:
* Return to prior activity level, including sport or work.
* Maintain strength and flexibility.
Exercises:
* Continue advanced strengthening and conditioning.
* Sport-specific drills, plyometrics, and high-impact activities if cleared by the surgeon and physical therapist.
* Emphasize maintenance and injury prevention.

Throughout rehabilitation, regular clinical and radiographic follow-up is essential to monitor fracture healing, identify complications, and adjust the rehabilitation protocol accordingly.
Summary of Key Literature and Guidelines
The management of distal femur fractures has evolved significantly with advances in implant design, surgical techniques, and a better understanding of fracture biology. Several key classification systems and principles guide current practice.
Classification Systems
- AO/OTA Classification: The most widely accepted system for long bone fractures, including the distal femur. It provides a standardized method for describing fracture morphology, guiding treatment decisions, and facilitating research. Distal femur fractures are designated as 33-A (extra-articular), 33-B (partial articular, unicondylar), and 33-C (complete articular, bicondylar). Subtypes further detail comminution and fragment patterns. This granular classification assists in predicting prognosis and tailoring surgical approaches.
Principles of Fixation
- Biological Fixation (MIPO): Modern approaches emphasize indirect reduction techniques and minimally invasive plate osteosynthesis (MIPO) to preserve the periosteal blood supply. This approach reduces soft tissue stripping, potentially leading to lower infection rates and improved healing capacity.
- Anatomic Reduction of Articular Surface: For intra-articular fractures (33-B, 33-C), anatomical reduction of the articular surface (step-off <2mm) is paramount to minimize the risk of post-traumatic osteoarthritis. Direct visualization, often with limited arthrotomy or arthroscopy, is frequently necessary.
- Angular Stable Fixation (Locking Plates): Locking plates have become the workhorse for distal femur fractures, particularly in osteoporotic bone. They provide fixed-angle constructs, offering angular stability independent of plate-to-bone compression, which is beneficial in metaphyseal comminution and poor bone quality.
- Relative Stability: While articular fragments require absolute stability, the metaphyseal and diaphyseal components benefit from relative stability to encourage callus formation and secondary bone healing. Bridging plating techniques are commonly employed for comminuted metaphyses.
Evidence-Based Guidelines
- Retrograde Intramedullary Nailing vs. Plating: The choice between retrograde intramedullary nailing and lateral locking plate fixation remains a topic of debate for specific fracture patterns. Nailing offers a load-sharing construct and may be advantageous for highly comminuted supracondylar fractures (33-A) and some simple articular patterns (33-C1) without significant articular extension. However, it requires an intact intercondylar notch and is less effective for reconstructive efforts involving articular fragments. Plating provides greater control over articular reduction and can accommodate complex articular comminution.
- Open Fractures: The management of open distal femur fractures follows established ATLS protocols, including urgent irrigation and débridement, appropriate antibiotic administration (e.g., first-generation cephalosporin for Gustilo Type I/II, adding aminoglycoside for Type III, and potentially penicillin for farm injuries), and often temporary external fixation followed by definitive internal fixation once the soft tissue envelope is optimized.
- Periprosthetic Fractures: Distal femur fractures around total knee arthroplasty (TKA) are increasingly common. The Vancouver classification system (A, B, C) guides management, often involving specialized periprosthetic plates (e.g., condylar locking plates designed for TKA components) or revision arthroplasty components with long stems, depending on implant stability and bone stock.
Continuous research and outcome studies further refine these principles, emphasizing functional recovery, complication mitigation, and patient-specific treatment plans.
Clinical & Radiographic Imaging
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding distal-femur-fractures