Operative Fixation of Medial Femoral Condyle Fractures
Key Takeaway
Isolated fractures of the medial femoral condyle require precise anatomical articular reduction to restore joint congruity and knee biomechanics. This guide details the anteromedial surgical approach, reduction techniques using joystick levers, and definitive fixation strategies—ranging from percutaneous lag screws to buttress plating. Early mobilization combined with rigid internal fixation ensures optimal functional recovery and minimizes post-traumatic osteoarthritis risk.
Comprehensive Introduction and Patho-Epidemiology
Isolated fractures of the medial femoral condyle, classified under the AO/OTA system as 33-B2 (sagittal split) and 33-B3 (coronal shear or Hoffa fractures), represent a relatively uncommon but highly challenging subset of distal femur fractures. While they account for only a fraction of all distal femoral injuries, their intra-articular nature and the immense weight-bearing demands placed upon the medial compartment of the knee make them critical injuries that require precise surgical management. The medial compartment is responsible for transmitting approximately 60% of the axial load during the normal human gait cycle. Consequently, even minute disruptions to the articular congruity or the mechanical axis can precipitate rapid joint degeneration, catastrophic varus instability, and severe post-traumatic osteoarthritis.
The patho-epidemiology of these fractures demonstrates a classic bimodal distribution, reflecting two distinct mechanisms of injury and patient demographics. In the younger population, these fractures are typically the result of high-energy trauma, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights. In these scenarios, the mechanism usually involves a direct axial load applied to a flexed knee, often combined with a severe varus stress that drives the medial tibial plateau into the medial femoral condyle, shearing it off. These high-energy injuries are frequently associated with significant soft tissue trauma, open wounds, and concomitant ligamentous injuries, particularly to the anterior cruciate ligament (ACL) or the medial collateral ligament (MCL).
Conversely, in the elderly population, medial condyle fractures occur via low-energy mechanisms, most commonly a simple fall from a standing height. The underlying pathophysiology in this demographic is intricately linked to osteoporosis, where the metaphyseal bone is severely compromised. In these osteoporotic fractures, the bone fails under minimal varus loading, often resulting in significant comminution, impaction of the articular surface, and complex fracture lines that challenge standard fixation techniques. The surgeon must recognize that the mechanical properties of the bone in this cohort dictate a completely different approach to internal fixation, often necessitating the use of locking plates and load-sharing constructs rather than simple lag screws.
Understanding the precise patho-anatomy is paramount for the orthopedic surgeon. If only one condyle is fractured and the femoral diaphysis remains intact, the operative intervention is conceptually focused purely on the joint. Because the shaft is not involved, the primary and overriding goal is the absolute anatomical restoration of the articular surface. The fundamental principle of treating these intra-articular injuries is absolute stability. Callus formation is not tolerated within a joint space; therefore, primary bone healing must be achieved through anatomical articular reduction combined with rigid interfragmentary compression. Whichever internal fixation construct is selected, it must neutralize the deforming forces sufficiently to allow for early, aggressive range of motion (ROM) to nourish the articular cartilage and prevent debilitating arthrofibrosis.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the distal femur is non-negotiable for the orthopedic surgeon attempting to reconstruct the medial femoral condyle. The distal femur expands from the cylindrical diaphysis into the complex, multi-planar geometry of the metaphysis and the two distinct condyles. The medial femoral condyle is anatomically distinct from its lateral counterpart; it is larger, extends further distally, and possesses a more pronounced convexity. This distal extension is critical for maintaining the normal physiologic valgus of the knee joint. The articular surface of the medial condyle articulates not only with the medial tibial plateau but also forms the medial border of the patellofemoral groove. Any malreduction in the sagittal or coronal plane will therefore disrupt both tibiofemoral kinematics and patellofemoral tracking.
The ligamentous and tendinous attachments to the medial condyle are critical landmarks and essential stabilizers that must be respected during surgical exposure. The medial epicondyle serves as the primary origin for the superficial medial collateral ligament (sMCL), a robust structure that resists valgus stress. Just proximal and posterior to the epicondyle lies the adductor tubercle, the insertion site for the adductor magnus tendon. The medial patellofemoral ligament (MPFL) attaches in the saddle region between the adductor tubercle and the medial epicondyle. Furthermore, the medial head of the gastrocnemius originates from the posterior aspect of the medial condyle. Aggressive surgical stripping of these soft tissue envelopes not only destabilizes the knee but critically compromises the vascular supply to the condylar fragment, which is heavily reliant on the superior and inferior medial genicular arteries. Avascular necrosis (AVN) of the condyle is a devastating complication directly linked to poor soft tissue handling.
Biomechanically, the medial femoral condyle is subjected to immense compressive and shear forces. The mechanical axis of the lower extremity (the line connecting the center of the femoral head to the center of the ankle joint) passes slightly medial to the center of the knee joint, predisposing the medial compartment to higher physiological loading (approximately 60% of total body weight during the stance phase of gait). When a medial condyle fracture occurs, the inherent varus moment at the knee tends to displace the fragment proximally and medially.
Fracture morphology dictates the biomechanical requirements of the fixation construct. A standard sagittal split (AO 33-B2) requires horizontally directed interfragmentary compression to resist the lateral-to-medial displacement forces. However, a coronal shear fracture (Hoffa fracture, AO 33-B3) presents a completely different biomechanical challenge. The fracture line runs in the coronal plane, creating a posterior articular fragment that is subjected to massive vertical shear forces during knee flexion and weight-bearing. Simple transverse lag screws are biomechanically insufficient to resist these vertical shear forces, often necessitating the addition of an anti-glide or buttress plate applied to the posterior or posteromedial cortex to convert the shear forces into compressive forces at the fracture site.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus nonoperative management of medial femoral condyle fractures is heavily weighted toward surgical intervention. Because of the intra-articular nature of the injury and the high load-bearing requirements of the medial compartment, nonoperative management is fraught with complications, including malunion, nonunion, varus collapse, and rapid-onset post-traumatic osteoarthritis. Consequently, nonoperative management is strictly reserved for a very narrow subset of patients: those who are non-ambulatory at baseline, those with truly nondisplaced fractures (which must be confirmed on CT, not just plain radiography), or those with prohibitive medical comorbidities where the risk of anesthesia and surgery outweighs the functional benefit of a reconstructed knee.
Operative fixation is the gold standard and is mandated for the vast majority of these injuries. The primary goal of surgery is to achieve an anatomical reduction of the articular surface, restore the mechanical axis of the lower extremity, and provide rigid fixation that allows for immediate postoperative mobilization. The threshold for operative intervention regarding articular step-off is incredibly low. While some historical texts cite a 2 mm step-off as the absolute indication for surgery, modern orthopedic principles emphasize that in the weight-bearing zones of the medial compartment, even a 1 mm step-off can significantly alter contact mechanics, increase peak focal stresses on the cartilage, and initiate the cascade of degenerative joint disease.
Furthermore, associated ligamentous instability is an absolute indication for surgical stabilization of the bony architecture. A fractured medial condyle often renders the MCL functionally incompetent, leading to profound varus and rotational instability. Restoring the bony anatomy is the prerequisite first step before any ligamentous reconstruction or healing can be considered. Open fractures, regardless of the degree of displacement, require emergent operative debridement, irrigation, and stabilization to mitigate the risk of devastating intra-articular sepsis.
| Parameter | Operative Indications | Nonoperative Indications / Contraindications |
|---|---|---|
| Articular Displacement | Step-off or gap > 1-2 mm in any plane. | Strictly nondisplaced (< 1 mm) on CT scan. |
| Joint Stability | Associated varus/valgus or rotational instability. | Stable knee exam in a completely nondisplaced fracture. |
| Fracture Pattern | Coronal shear (Hoffa), irreducible fragments, open fractures. | Severe, non-reconstructable comminution in a non-ambulator. |
| Patient Status | Ambulatory patients, polytrauma patients requiring mobilization. | Bedbound baseline, prohibitive cardiopulmonary risk, active local infection. |
| Soft Tissue Envelope | Compartment syndrome, vascular compromise. | Severe soft tissue compromise precluding safe incision (relative contraindication; requires spanning ex-fix). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful intra-articular fracture surgery. The standard radiographic series—anteroposterior (AP), lateral, and bilateral oblique views of the knee—provides the initial assessment of the fracture pattern. However, plain radiographs are notoriously inadequate for fully characterizing the true extent of articular comminution, identifying impacted osteochondral fragments, or accurately diagnosing coronal shear (Hoffa) fractures. The complex overlapping bony anatomy of the distal femur often obscures subtle fracture lines.
Therefore, a preoperative computed tomography (CT) scan with fine (1 mm) axial cuts and multi-planar 3D reconstructions is considered the absolute gold standard and is mandatory for all suspected medial condyle fractures. The CT scan allows the surgeon to map the exact trajectory of the fracture planes, quantify the size of the articular fragments, and identify any central articular impaction that will require elevation and bone grafting. Furthermore, the CT scan is indispensable for preoperative templating. The surgeon must mentally and digitally rehearse the operation, selecting the appropriate screw trajectories to ensure they are perfectly perpendicular to the fracture plane, and determining whether the fragment size necessitates a buttress plate. Digital templating software should be used to estimate screw lengths and plate sizes, ensuring the required inventory is available in the operating room.
Patient positioning must be executed with precision to facilitate both the surgical approach and unimpeded intraoperative fluoroscopy. The patient is placed supine on a completely radiolucent flat-topped table. A standard operating table with a radiolucent extension can be used, but a dedicated Jackson table or fracture table often provides superior imaging access. A bump (often a rolled blanket or specialized foam pad) is placed under the ipsilateral hip. This corrects the natural external rotation of the lower extremity, ensuring that the patella faces directly toward the ceiling, which is critical for establishing accurate coronal and sagittal alignment during reduction. A sterile tourniquet is applied to the proximal thigh to provide a bloodless field during the critical phases of articular visualization, though its use should be minimized to prevent ischemic complications.
Fluoroscopy positioning is a critical step that must be finalized before the patient is prepped and draped. The C-arm is typically positioned on the contralateral side of the table, entering perpendicular to the patient. The surgeon must verify that perfect AP and lateral views of the distal femur can be obtained without obstruction from the table pedestal or the contralateral leg. The lateral view is particularly crucial for assessing the reduction of the articular surface and ensuring that screws do not penetrate the patellofemoral joint. Often, simple condylar fractures can be provisionally reduced with longitudinal traction and maintained with large, pointed periarticular reduction clamps applied percutaneously before the formal incision is made. This percutaneous provisional reduction can significantly simplify the subsequent open procedure.
Step-by-Step Surgical Approach and Fixation Technique
Open reduction and internal fixation (ORIF) is strictly indicated for displaced, irreducible condylar fractures or when percutaneous methods fail to achieve an absolute anatomical articular surface. The anteromedial approach is the workhorse for these injuries, providing unparalleled visualization of the medial condyle, the medial aspect of the intercondylar notch, and the medial patellofemoral articulation.
The Anteromedial Surgical Dissection
The skin incision begins longitudinally on the anteromedial aspect of the knee, starting approximately 10 cm proximal to the joint line. It is extended distally to just below the level of the joint line, curving slightly toward the medial tibial tubercle if distal exposure is required. The dissection is deepened through the subcutaneous tissues to expose the extensor mechanism, taking care to achieve meticulous hemostasis. An arthrotomy is then performed by incising the joint capsule and synovium perfectly in line with the skin incision.
To gain adequate proximal exposure, this arthrotomy is extended proximally along the lateral edge of the vastus medialis muscle, precisely at its junction with the quadriceps tendon—a classic medial parapatellar arthrotomy. The patella is then gently retracted laterally. This exposes the entire medial femoral condyle, the patellofemoral groove, and the intercondylar area. The surgeon must exercise extreme caution to avoid aggressively stripping the soft tissue attachments from the medial epicondyle. The medial collateral ligament (MCL) and the local vascular anastomoses must be preserved; devascularization of the medial condyle fragment will almost certainly lead to nonunion or avascular necrosis.
Fracture Reduction and the Joystick Technique
Upon entering the joint, a significant hemarthrosis will invariably be present. The joint must be thoroughly cleared of all hematoma, debris, and loose, non-viable bone chips using copious pulsatile irrigation. The meniscus and cruciate ligaments must be inspected for associated pathology, as meniscal entrapment within the fracture site is a known cause of irreducibility.
To manipulate the fractured condyle, the "joystick technique" is highly effective. A 3.2-mm or 4.0-mm Steinmann pin, or a partially threaded Schanz screw, is inserted directly into the large medial condylar fragment. This pin acts as a robust lever, allowing the surgeon to manipulate the fragment in multiple planes—correcting rotation, translation, and angulation simultaneously. The fracture is reduced under direct, bright illumination, ensuring absolute, perfect congruity of the articular cartilage. Once anatomical reduction is achieved, it is provisionally maintained by inserting multiple smooth Kirschner wires (K-wires) across the fracture site, driving them from the medial fragment directly into the intact lateral femoral condyle. These provisional wires must be strategically placed outside the planned trajectory of the definitive fixation screws.
Definitive Fixation: Lag Screws and Buttress Plating
The choice of definitive implant depends heavily on the fracture pattern, the size of the articular fragment, and the patient's bone density. For large, uncomminuted sagittal split fractures of the medial condyle, cancellous lag screw fixation provides excellent, rigid interfragmentary compression. The trajectory of these screws must be planned to be perfectly perpendicular to the fracture plane to maximize compression and prevent shear forces from displacing the reduction during tightening.
When utilizing fully threaded screws, the near cortex (the medial fragment) must be overdrilled to create a gliding hole (e.g., using a 4.5 mm drill for a 4.5 mm screw), while the far cortex is drilled with the core diameter (e.g., 3.2 mm drill). Alternatively, partially threaded cancellous screws can be used, ensuring all threads bypass the fracture line to achieve the lag effect. Typically, two or three large-diameter screws (ranging from 4.5-mm to 6.5-mm) are placed to fix the medial fragment to the intact lateral condyle.
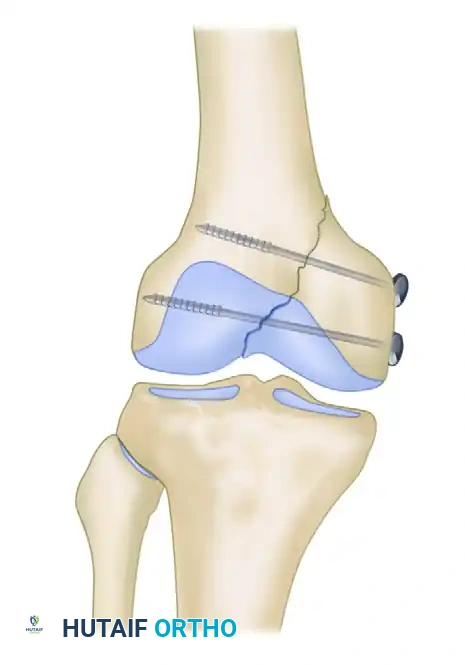
FIGURE 54-72: Fracture of the medial condyle fixed with 6.5-mm cancellous screws. Note the perpendicular trajectory to the fracture line to maximize interfragmentary compression.
In patients with osteoporotic bone, the thin medial cortex provides poor purchase. In these cases, a metal washer must be placed under the head of the screw to distribute the load and prevent the screw head from sinking through the metaphyseal bone, which would instantly result in a loss of compression. Furthermore, it is absolutely critical that the screws achieve bicortical purchase. Osteoporotic cancellous bone within the condyle does not afford adequate pull-out strength; engaging the dense lateral cortex is mandatory for construct stability.
In scenarios involving severe osteoporotic bone, vertical shear fracture patterns, or metaphyseal comminution, fixation with lag screws alone is biomechanically inadequate and will fail under physiological loads. In these instances, a buttress plate must be applied to neutralize the shear forces. A small fragment locking plate, or a specifically contoured distal femoral medial plate, is applied to the medial cortex. Interfragmentary compression is first achieved with independent 3.5-mm or 4.5-mm lag screws (either through the plate or outside of it). The plate is then secured, acting as an anti-glide construct to physically block the proximal and medial migration of the condylar fragment. For coronal shear (Hoffa) fractures, screws must be directed from anterior to posterior (AP) or posterior to anterior (PA), strictly perpendicular to the coronal fracture line, often requiring headless compression screws countersunk beneath the articular cartilage.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative fixation of medial femoral condyle fractures carries a significant risk of complications. The intra-articular nature of the injury, combined with the high mechanical stresses of the knee joint and the frequently compromised bone quality in elderly patients, creates an environment where both biological and mechanical failures can occur. Surgeons must counsel patients extensively regarding these risks and maintain a high index of suspicion during the postoperative follow-up period.
The most common complication following distal femur intra-articular fractures is arthrofibrosis, or profound knee stiffness. This is directly correlated with prolonged postoperative immobilization and failure to initiate early range of motion. The suprapatellar pouch and the capsular recesses rapidly develop dense adhesions if the knee is not mobilized within the first few days after surgery. Loss of fixation is another catastrophic complication, primarily occurring in osteoporotic bone where the surgeon failed to achieve lateral cortical purchase, or in vertical shear patterns where a buttress plate was omitted. When the fixation fails, the condyle displaces proximally, leading to immediate varus collapse of the knee.
Post-traumatic osteoarthritis (PTOA) is a late but frequent complication, directly linked to the quality of the initial articular reduction. A residual articular step-off greater than 2 mm significantly increases peak contact stresses, leading to accelerated cartilage wear. Even with perfect anatomical reduction, the initial impact of the trauma causes chondrocyte apoptosis, meaning PTOA can still develop years later. Furthermore, prominent medial-sided hardware, particularly bulky buttress plates or screw heads that are not properly seated, can cause severe irritation to the vastus medialis or the superficial MCL. This often necessitates a secondary surgery for hardware removal once complete fracture union is confirmed (typically 12 to 18 months postoperatively).
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Arthrofibrosis (Stiffness) | 15% - 30% | Prolonged immobilization, excessive surgical trauma, delayed rehab. | Aggressive physical therapy; Manipulation under anesthesia (MUA); Arthroscopic lysis of adhesions. |
| Loss of Fixation / Varus Collapse | 5% - 10% | Osteoporosis, failure to use buttress plate for shear patterns, poor screw purchase. | Revision ORIF with locking plates and bone grafting; Distal femoral replacement (megaprosthesis) in elderly. |
| Post-Traumatic Osteoarthritis | 20% - 40% (Long-term) | Articular step-off > 2mm, initial cartilage impact damage, meniscal injury. | Activity modification, injections; Total Knee Arthroplasty (TKA) for end-stage disease. |
| Nonunion / Avascular Necrosis | < 5% | Excessive stripping of medial epicondyle (vascular supply), inadequate fixation stability. | Revision ORIF with autologous bone grafting; TKA or Megaprosthesis if AVN is severe. |
| Hardware Irritation | 10% - 20% | Prominent screw heads, bulky medial anti-glide plates irritating the MCL. | Elective hardware removal after definitive radiographic and clinical union (minimum 12 months). |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome following the operative fixation of a medial femoral condyle fracture is as dependent on the postoperative rehabilitation protocol as it is on the surgical execution. The residual disability can be minimized, and an excellent range of motion can be regained, provided that the internal fixation is absolutely rigid, allowing for immediate joint mobilization. The rehabilitation must be carefully phased to protect the articular reduction while simultaneously preventing the debilitating effects of arthrofibrosis and muscle atrophy.
Phase 1: Immediate Postoperative (Days 0-14)
The primary goals in the first two weeks are wound healing, edema control, and the prevention of joint stiffness. Immediately postoperatively, the patient is placed in a bulky soft dressing with a light compression wrap and a hinged knee brace locked in extension for ambulation. Continuous passive motion (CPM) can be initiated in the recovery room or on postoperative day one, typically starting at 0 to 30 degrees and increasing by 10 degrees daily as tolerated by the patient's pain levels. Ambulation with a walker or crutches is started on postoperative day one or two. Weight-bearing is strictly limited to touch-down weight bearing (TDWB) or non-weight bearing (NWB) to completely protect the articular reduction from the massive compressive forces of the gait cycle. Active-assisted range of motion exercises are encouraged, focusing on achieving full terminal extension.
Phase 2: Early Rehabilitation (Weeks 2-6)
Once the surgical incisions have healed and the sutures are removed, the focus shifts to more aggressive range of motion and early muscle activation. The goal by the end of week six is to achieve a minimum of 90 to 100 degrees of knee flexion and maintain full, active extension. Isometric quadriceps sets, straight leg raises, and gentle hamstring curls are initiated to prevent profound muscle atrophy. Patellar mobilization techniques are crucial during this phase to prevent scarring of the extensor mechanism. Weight-bearing status remains strictly TDWB. The articular cartilage and the underlying subchondral bone require a minimum of six weeks to begin meaningful consolidation without the destructive stress of axial loading.
Phase 3: Intermediate Rehabilitation (Weeks 6-12)
At the six-week mark, new orthogonal radiographs are obtained to assess for early callus formation at the metaphyseal fracture lines and to ensure the absolute maintenance of the articular reduction. If the fracture is demonstrating satisfactory clinical and radiographic signs of healing, and the patient is pain-free at the fracture site upon palpation, a graduated weight-bearing protocol is initiated. The patient progresses to partial weight bearing (PWB), typically starting at 25% of their body weight and increasing by 25% every one to two weeks. Closed-chain kinetic exercises, such as mini-squats and leg presses with restricted weight, are introduced to stimulate bone healing through controlled mechanical stress (Wolff's Law) and to rebuild quadriceps endurance.
Phase 4: Advanced Rehabilitation (Weeks 12+)
By 12 weeks postoperatively, assuming complete radiographic union is evident, the patient is transitioned to full weight bearing (FWB) without the use of assistive devices. The rehabilitation focus shifts entirely to advanced strengthening, proprioception training, and the normalization of gait mechanics. Advanced closed-chain exercises, stationary cycling with resistance, and balance board training are emphasized. Return to heavy manual labor or high-impact sports is generally not permitted until 5 to 6 months postoperatively, and only after the patient has demonstrated symmetrical lower extremity strength (at least 85% of the contralateral limb) and complete absence of pain during functional testing.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative techniques for medial femoral condyle fractures is deeply rooted in the biomechanical and clinical literature. The foundational principles of intra-articular fracture management, originally championed by the AO Foundation and heavily influenced by Letournel's work on acetabular fractures, dictate that absolute anatomical reduction is the paramount predictor of long-term joint survival. Landmark clinical studies have consistently demonstrated that an articular step-off of greater than 2 mm leads to a statistically significant increase in the rapid development of post-traumatic osteoarthritis. Modern orthopedic consensus, however, pushes this threshold even lower, arguing that in the highly loaded medial compartment, any palpable step-off is unacceptable and warrants surgical correction.
The literature surrounding coronal shear (Hoffa) fractures has fundamentally altered preoperative imaging guidelines. Multiple retrospective reviews have highlighted that up to 30% of Hoffa fractures are missed or severely underestimated on standard plain anteroposterior and lateral radiographs. This high miss rate has led to the universal clinical guideline that any high-energy distal femur fracture, or any fracture with suspicious intra-articular extension, mandates a preoperative CT scan with 3D reconstructions. The CT scan is no longer considered an optional adjunct; it is the standard of care required for accurate diagnosis and surgical templating.
Furthermore, biomechanical studies evaluating fixation constructs have definitively proven the superiority of combined screw and plate constructs over isolated lag screws in specific fracture patterns. In vertical shear injuries and osteoporotic bone models, isolated cancellous screws frequently fail under physiological cyclical loading due to the lack of a buttress effect. Literature dictates that the addition of a medial anti-glide plate significantly increases the load to failure and minimizes fracture micromotion, establishing buttress plating as the gold standard guideline for complex, comminuted, or osteoporotic medial condyle fractures. Adherence to these evidence-based guidelines is critical for optimizing patient outcomes and minimizing the high complication rates historically associated with these severe intra-articular injuries.
