Reconstruction Materials: What You Need to Know About Associated Complications
Key Takeaway
This article provides essential research regarding Reconstruction Materials: What You Need to Know About Associated Complications. A femoral neck fracture in an 82-year-old with a total hip replacement most likely occurred due to mechanical etching or laser marking on the component during production. This relates to the inherent quality of the implant's materials and associated manufacturing processes. Risk factors for such failures can include excessive body weight and inadequate proximal osseous support.
We are discussing orthopaedic reconstruction materials. A critical concern in any implant surgery is the interaction between the host and the material. Could you define the concept of 'stress shielding' and describe how we mitigate this when selecting reconstruction hardware?
Candidate: Stress shielding happens when an implant is stiffer than the bone, like a metal plate or stem. Because it's stiffer, it carries most of the load, so the bone underneath doesn't get the stress it needs to remodel, according to Wolff's Law. This causes the bone to thin out or resorb. We try to use materials with a lower modulus of elasticity or implants that allow for load-sharing rather than being purely load-bearing.
Failing to mention Wolff's Law by name or lacking a technical explanation of the "modulus of elasticity" mismatch. Some candidates confuse stress shielding with aseptic loosening from wear debris, which are distinct pathologies.
Define stress shielding as the reduction in bone density resulting from the removal of normal physiological stress by a high-stiffness implant (stiff vs. stiff). Explicitly cite Wolff’s Law. Explain that the mismatch in the Young’s Modulus (e.g., Cobalt Chrome vs. Bone) leads to the implant bearing the load. Mitigation strategies include: using lower modulus materials like Titanium alloys, utilizing load-sharing constructs, or designing implants with "tapered" geometries to allow gradual stress transfer rather than abrupt transitions.
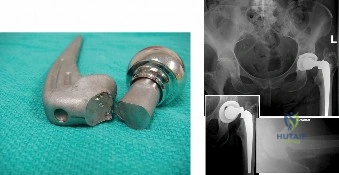
The image provided shows a range of bearing materials used in joint reconstruction. In the context of modern hip arthroplasty, what is the significance of the "bearing couple" in terms of long-term failure mechanisms?
Candidate: The bearing couple is the interface between the head and the liner. The main failure mechanism historically was polyethylene wear, which creates debris. This debris leads to macrophage activation and osteolysis, ultimately causing aseptic loosening. We now use highly cross-linked polyethylene and ceramic bearings to minimize this wear and the subsequent osteolytic reaction.
Missing the concept of the biological response to particulate debris. A weak candidate might say "it just wears out" without explaining the osteolysis mediated by macrophages that leads to the actual loosening of the components.
Systematically structure the response: 1) Wear Particles: The production of sub-micron particles (specifically polyethylene) triggers a systemic or local immune response. 2) Osteolytic Cascade: Macrophages ingest debris, releasing pro-inflammatory cytokines (IL-1, IL-6, TNF-alpha), which activate osteoclasts. 3) Mechanical Result: Periprosthetic bone resorption occurs, leading to component migration and aseptic loosening. Mention that current "Gold Standards" like highly cross-linked polyethylene have significantly reduced volumetric wear rates compared to conventional UHMWPE.
When considering the use of allograft versus autograft for a large intercalary defect, what are the primary biological and clinical risks you must explain to the patient during informed consent?
Candidate: Autograft is the gold standard because it's osteoinductive, osteoconductive, and osteogenic. The risk is donor site morbidity, like pain or nerve injury. Allograft is great for large defects but the risk is that it takes longer to heal, it can break or fail to incorporate, and there's a tiny risk of disease transmission or immune reaction.
Failing to mention the "Creeping Substitution" process for allograft incorporation. A poor candidate treats the graft as an inert bridge rather than a scaffold that requires remodeling.
Contrast the properties: Autograft provides the "triad" (Osteoinduction, Osteoconduction, Osteogenesis). Identify the distinct risks:
- Autograft: Donor site morbidity (e.g., lateral femoral cutaneous nerve injury for iliac crest).
- Allograft: Slower creeping substitution (host bone remodeling), higher risk of non-union, and structural failure. Mention the minimal but real risk of disease transmission (e.g., HIV, Hepatitis) and immune response, managed through strict tissue bank processing (gamma irradiation/freeze-drying).
