Hallux Rigidus: Pathophysiology, Surgical Anatomy & Biomechanics Guide
Key Takeaway
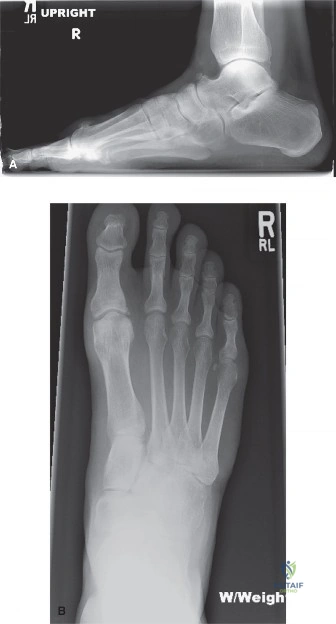
Hallux rigidus is a degenerative arthritic condition of the first metatarsophalangeal (MTP) joint, characterized by stiffness, pain, and restricted dorsiflexion. Its pathophysiology involves genetic predisposition, biomechanical factors like metatarsus primus elevatus, and traumatic events. These lead to cartilage degeneration and osteophyte formation, particularly dorsally, impeding motion.
A 55-year-old active male presents with a 2-year history of worsening dorsal foot pain. He reports difficulty wearing stiff-soled work boots and pain during the push-off phase of gait. On examination, there is palpable dorsal bony prominence and restricted passive dorsiflexion of the first MTP joint. You order weight-bearing radiographs. Based on the clinical presentation and the typical findings in this condition, how would you classify and manage this patient?
Candidate: I would suspect Hallux Rigidus. I would classify it using the Coughlin and Shurnas system. Since the patient has dorsal pain and limited motion, I would start with conservative management like stiff-soled shoes or orthotics. If that fails, I would offer surgery, likely a cheilectomy.
Failing to define the Coughlin and Shurnas stages specifically or neglecting to mention the importance of the lateral radiograph in assessing "metatarsus primus elevatus." Candidates often fail to distinguish between motion-preserving procedures (cheilectomy/osteotomy) and arthrodesis, suggesting surgery too generically without linking it to the specific grade.
I would perform a clinical assessment and weight-bearing radiographs (AP, lateral, and oblique) to stage the condition using the Coughlin and Shurnas classification (0-4). The lateral view is critical to assess the extent of dorsal osteophytes and the presence of metatarsus primus elevatus. For a grade 1 or 2, I would recommend a trial of conservative care: stiff-soled shoes, rocker-bottom modifications, and NSAIDs. If surgery is required, I would discuss the risks/benefits of a cheilectomy (dorsal decompression) to remove the impingement. If the patient has advanced, end-stage (Grade 4) disease, I would counsel them toward a first MTP arthrodesis, which remains the gold standard for predictable pain relief and durable function.
Following a failed cheilectomy for Grade 2 Hallux Rigidus, the patient now has persistent pain and restricted motion. You are considering a Moberg osteotomy. Explain the biomechanical rationale for this procedure and how it alters the functional anatomy of the first ray.
Candidate: The Moberg osteotomy is a dorsal closing wedge osteotomy of the proximal phalanx. It shifts the phalanx dorsally to allow more room for dorsiflexion. It essentially re-orients the joint to give the patient more functional range of motion during gait.
Candidates often miss the "Windlass Mechanism" connection. They explain it as "making more room" but fail to explain that it changes the neutral position of the hallux relative to the weight-bearing surface, thereby decreasing the required dorsiflexion during the toe-off phase of the gait cycle.
The Moberg osteotomy is a dorsal closing wedge osteotomy at the base of the proximal phalanx. Its primary biomechanical goal is to functionally increase dorsiflexion by reorienting the phalanx. By dorsiflexing the base of the phalanx relative to the metatarsal head, it effectively "pre-loads" the hallux into a position of dorsiflexion. This reduces the amount of active dorsiflexion required at the MTP joint during the toe-off phase of the gait cycle, thereby bypassing the impingement area and reducing pain without needing to further resect the metatarsal head, which preserves stability and the Windlass mechanism.
