
Comprehensive Introduction and Patho-Epidemiology
Fellows, welcome to the operating theater. Today, we embark on a journey through the intricacies of Cemented Total Hip Arthroplasty (THA), a procedure that, for over four decades, has stood as the most successful surgical solution for end-stage hip disease. Sir John Charnley’s pioneering work in the 1960s with low-friction arthroplasty revolutionized our field, establishing the use of polymethylmethacrylate (PMMA) bone cement as a reliable medium for implant fixation. Our goal today is not merely to perform an operation, but to impart the critical principles, meticulous technique, and clinical wisdom that ensure reproducible, durable, and outstanding long-term patient outcomes.
Before we even consider the scalpel, a profound understanding of the patient's pathology and a thorough preoperative assessment are paramount. Cemented THA is an incredibly versatile treatment, addressing a broad spectrum of hip pathologies that culminate in advanced degeneration. The conditions that lead patients to our operating table are varied, each presenting its own distinct biomechanical challenges, bone quality considerations, and anatomical distortions that must be accounted for during surgical planning.

The Spectrum of End-Stage Hip Disease
Most commonly, we encounter osteoarthritis (OA), which may be idiopathic or secondary to underlying biomechanical aberrations. The natural history of degenerative joint disease is relentless progression, characterized by articular cartilage fibrillation, subchondral sclerosis, osteophyte formation, and eventual joint space collapse. While medical therapies and intra-articular injections can temporarily manage the inflammatory cascade associated with conditions like rheumatoid arthritis or acute OA flares, they do not act as definitive disease-modifying agents for the structural mechanical failure of the joint.
Inflammatory arthritides, including rheumatoid arthritis and the seronegative spondyloarthropathies, present a different pathophysiological challenge. Driven by systemic autoimmunity, these conditions often result in widespread synovial hypertrophy, pannus formation, and symmetric joint destruction. The bone in these patients is frequently osteopenic or osteoporotic, not only from the disease process itself but also from chronic corticosteroid use. This poor bone stock makes cemented fixation particularly advantageous, as it does not rely on host bone ingrowth for initial or long-term stability.
Vascular necrosis, or osteonecrosis, introduces another layer of complexity. Whether idiopathic or linked to etiologic factors such as high-dose corticosteroid use, alcoholism, sickle cell disease, or coagulopathies, the fundamental insult is a compromise of the vascular supply to the femoral head. This leads to bone infarction, subchondral collapse, and subsequent rapid secondary arthrosis. Furthermore, developmental abnormalities like Developmental Dysplasia of the Hip (DDH) and Femoroacetabular Impingement (FAI) predispose the hip to abnormal joint reaction forces and articular shear forces, accelerating mechanical joint degeneration well before the typical age of onset for primary OA.
Pathophysiological Mechanisms of Degeneration
Understanding the microscopic and macroscopic deterioration of the hip joint is essential for appreciating why arthroplasty provides such profound relief. In the osteoarthritic hip, the delicate balance between chondrocyte-mediated synthesis and degradation of the extracellular matrix is disrupted. Matrix metalloproteinases (MMPs) and pro-inflammatory cytokines, such as Interleukin-1 (IL-1) and Tumor Necrosis Factor-alpha (TNF-a), drive the catabolic destruction of type II collagen and aggrecan, leading to a loss of the cartilage's viscoelastic properties.
As the cartilage thins, the underlying subchondral bone is subjected to increased focal mechanical stress. This triggers a reparative but ultimately maladaptive response, resulting in subchondral sclerosis and the formation of subchondral cysts (geodes) due to the intrusion of synovial fluid through microfractures in the bone plate. Concurrently, endochondral ossification at the joint margins produces osteophytes in a futile attempt to distribute the abnormal load over a broader surface area.
In the context of cemented arthroplasty, these pathophysiological changes directly dictate our intraoperative strategy. Sclerotic bone, for instance, resists the interdigitation of PMMA. Therefore, during acetabular and femoral preparation, we must meticulously expose the underlying cancellous bone bed. The preservation of a robust cancellous layer, unlike the aggressive reaming often utilized in press-fit techniques, is the cornerstone of achieving micro-interlock with the bone cement, thereby transforming the bone-cement interface into a durable composite structure capable of withstanding decades of cyclic loading.
Detailed Surgical Anatomy and Biomechanics
A masterful cemented THA requires a three-dimensional appreciation of the hip's surgical anatomy and its underlying biomechanics. The hip is a classic diarthrodial ball-and-socket joint, engineered for both high mobility and immense weight-bearing capacity. To restore normal kinematics, the surgeon must precisely reconstruct the center of rotation, the femoral offset, and the leg length, all while navigating a complex topography of neurovascular structures and dynamic muscular stabilizers.
Osteology and Articular Mechanics
The acetabulum is a hemispherical cavity formed by the confluence of the ilium, ischium, and pubis. Its articular surface, the lunate facies, is covered with hyaline cartilage, while the central cotyloid fossa contains the ligamentum teres and a fat pad. Radiographically, we rely on landmarks such as the radiographic teardrop (the inferior margin of the acetabulum), Kohler’s line (the ilioischial line), and the sourcil (the weight-bearing dome). When preparing the acetabulum for a cemented component, our objective is to ream to a true hemisphere, medializing to the cotyloid fossa without violating the medial wall, thereby optimizing the biomechanical center of rotation.
The proximal femur consists of the head, neck, and the greater and lesser trochanters. The femoral neck projects superomedially and anteriorly, establishing the critical parameters of neck-shaft angle (typically 125-135 degrees) and femoral anteversion (typically 10-15 degrees). The calcar femorale, a dense vertical plate of bone extending from the posteromedial aspect of the femoral shaft to the posterior portion of the femoral neck, provides crucial structural support. In cemented femoral fixation, the stem must be positioned in neutral alignment, surrounded by an intact, uniform mantle of PMMA that transfers loads seamlessly from the prosthesis to the endosteal bone.
Biomechanically, the hip operates as a first-class lever during the single-leg stance phase of gait. The body weight acts on a long lever arm extending from the center of gravity to the center of the femoral head, while the abductor musculature acts on a much shorter lever arm extending from the greater trochanter to the center of the femoral head. To maintain a level pelvis, the abductors must generate a force approximately 2.5 to 3 times body weight. Consequently, the joint reaction force across the hip can exceed 3 to 4 times body weight during normal walking. Restoring the femoral offset (the perpendicular distance from the center of rotation to the anatomical axis of the femur) is critical; inadequate offset weakens the abductor moment arm, leading to a Trendelenburg gait and increased joint reaction forces, which can accelerate cement mantle fatigue.
Myology and Neurovascular Topography
The muscular envelope of the hip is divided into distinct functional groups that must be respected and, when necessary, carefully repaired during the surgical approach. The abductors, primarily the gluteus medius and minimus, are innervated by the superior gluteal nerve. Damage to these muscles or their nerve supply is catastrophic, resulting in intractable limp and instability. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris) are frequently divided in the posterior approach to access the joint capsule; meticulous enhanced posterior soft tissue repair of these structures is essential to minimize the risk of postoperative dislocation.
Anteriorly, the iliopsoas acts as the primary hip flexor, and its tendon can occasionally be a source of postoperative impingement against an oversized or retroverted acetabular component. The rectus femoris and sartorius provide additional anterior dynamic stability. The neurovascular bundles demand our utmost vigilance. The sciatic nerve, exiting the greater sciatic foramen typically below the piriformis, is intimately related to the posterior aspect of the hip joint and is at risk during posterior retractor placement or excessive limb lengthening.
Anteriorly, the femoral nerve, artery, and vein lie within the femoral triangle, separated from the hip joint by the iliopsoas muscle. While rarely injured directly during a posterior or lateral approach, they can be compromised by errant anterior retractor placement or cement extrusion through an unrecognized medial wall defect. Understanding this complex three-dimensional anatomy is not merely an academic exercise; it is the fundamental prerequisite for executing a safe, efficient, and anatomically restorative arthroplasty.
Exhaustive Indications and Contraindications
The decision to proceed with a cemented THA over a cementless (press-fit) alternative is a nuanced one, predicated on a careful analysis of patient demographics, bone morphology, and the specific underlying pathology. While cementless fixation has become the dominant paradigm in North America for the majority of primary THAs, cemented fixation remains the undisputed gold standard for specific patient populations, offering immediate stability and unparalleled long-term survivorship in compromised bone.
Patient Selection Criteria
The ideal candidate for a cemented total hip arthroplasty is typically an older patient (generally over 65 to 70 years of age) with lower physical demands and compromised bone quality. In these patients, particularly postmenopausal females, the proximal femur often exhibits a "stovepipe" morphology—classified as Dorr Type C bone. This bone is characterized by thin cortices and a wide, capacious medullary canal lacking the robust cancellous isthmus required for reliable initial scratch-fit and subsequent biological osteointegration of a cementless stem.

Furthermore, cemented fixation is highly indicated in patients with previously irradiated bone, such as those treated for pelvic or proximal femoral malignancies. Radiation profoundly impairs the osteogenic potential of local mesenchymal stem cells, rendering biological ingrowth unpredictable or impossible. Similarly, patients with severe metabolic bone diseases, Paget's disease, or chronic renal osteodystrophy are excellent candidates for cemented constructs, as the PMMA acts as an immediate structural grout, bypassing the need for host bone remodeling.
Conversely, young, highly active patients with robust, Dorr Type A (champagne flute) bone are generally better served by cementless implants. In this demographic, the repetitive high-impact cyclic loading can eventually lead to fatigue failure of the cement mantle over several decades. Additionally, active local or systemic infection is an absolute contraindication to any arthroplasty, and in cases of severe active infection, a staged approach with an antibiotic-loaded PMMA spacer is required before definitive reconstruction can be considered.
Table of Indications and Contraindications
| Category | Cemented THA Indications | Cemented THA Contraindications |
|---|---|---|
| Patient Demographics | Elderly patients (>70 years); Low physical demand; Postmenopausal females. | Young, highly active patients (<50 years); High-impact sports participants. |
| Bone Quality / Morphology | Dorr Type C bone (stovepipe canal); Severe osteoporosis; Thin cortices. | Dorr Type A bone (champagne flute canal); Thick, robust cortices. |
| Pathologic Conditions | Irradiated bone; Paget's disease; Metastatic disease requiring immediate stability; Rheumatoid arthritis with severe osteopenia. | Active local joint infection; Uncontrolled systemic sepsis. |
| Anatomical Challenges | Proximal femoral deformity precluding cementless stem fit; Wide medullary canals where press-fit would require excessive bone removal. | Severe hypersensitivity to polymethylmethacrylate (PMMA) or its components (extremely rare). |
Pre-Operative Planning, Templating, and Patient Positioning
Once pain has been definitively localized to the hip, and conservative measures have been exhausted, we transition to the critical phase of surgical planning. Preoperative planning is not a mere suggestion; it is the blueprint for surgical success. It allows the surgeon to anticipate anatomical anomalies, select the appropriate implant philosophy, predict component sizing, and establish a precise strategy for restoring the patient's unique biomechanics.
Clinical Assessment and Differential Diagnosis
Our initial clinical evaluation must precisely identify the extent to which the patient's pain originates from intra-articular hip pathology. Hip pain is a notorious mimicker. Patients typically report deep groin pain, but it frequently refers to the peritrochanteric region, the anterior thigh, the knee, or occasionally even distal to the knee. Overlap with lumbar spine disease is incredibly common; spinal stenosis or lumbar radiculopathy frequently causes pain in these exact same dermatomal regions. A thorough neurological examination, including straight leg raise testing, is mandatory to differentiate neurogenic claudication from coxarthrosis.

The physical examination must systematically unveil the pathology. We assess active and passive Range of Motion (ROM), noting that limited internal rotation and abduction in flexion are the hallmark early signs of hip arthritis. A fixed flexion contracture, elucidated by the Thomas test, is a common finding that must be addressed intraoperatively to prevent postoperative lumbar hyperlordosis and anterior pelvic tilt. Motor power, particularly of the abductors, is assessed; profound abductor weakness diminishes the likelihood of achieving a limp-free gait post-arthroplasty and may influence our choice of surgical approach.
Leg-Length Discrepancy (LLD) must be meticulously evaluated. We observe for true shortening, which is common in severe DJD and DDH, and differentiate it from apparent shortening caused by adduction or abduction contractures. Pelvic tilt resulting from fixed spinal deformity (e.g., scoliosis) can also contribute to functional LLD. Documenting these findings preoperatively manages patient expectations and guides our intraoperative templating to ensure we do not inadvertently overlengthen the limb in an attempt to achieve stability.
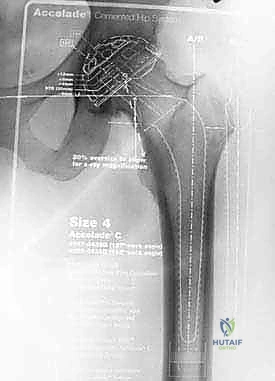
Radiographic Analysis and Templating Methodology
Plain radiographs remain our primary diagnostic and planning tool. A high-quality, low Anteroposterior (AP) view of the pelvis, centered over the pubic symphysis and including the proximal third of the femora, is non-negotiable. The hips must be internally rotated approximately 15 degrees to profile the true femoral neck-shaft angle and offset. We verify the quality of the film by ensuring the coccyx points directly to the symphysis pubis, located about 1 to 3 cm superior to it, confirming the absence of significant pelvic rotation or tilt.
Templating is our surgical roadmap. We begin by establishing consistent pelvic reference lines on the AP radiograph. A horizontal line connecting the inferior margins of the radiographic teardrops provides the baseline. We then mark the most prominent medial point of the lesser trochanters. By measuring the perpendicular distance from the inter-teardrop line to the lesser trochanters bilaterally, we precisely quantify the radiographic leg-length discrepancy.
Next, we template the acetabulum. The goal is to identify a component size that achieves maximum contact with the subchondral bone while restoring the anatomical center of rotation. We position the template such that its medial border rests against the teardrop, the superolateral border provides adequate coverage beneath the sourcil, and the inferior border aligns with the obturator foramen. Once the center of rotation is established, we template the femur. We select a stem size that allows for a uniform 2 to 3 mm cement mantle circumferentially. The neck cut is planned relative to the lesser trochanter to restore the patient's native femoral offset and precisely correct the calculated leg-length discrepancy.
Anesthesia, Positioning, and Operative Preparation
The choice of anesthesia—typically regional (spinal or epidural) versus general—is made in conjunction with the anesthesia team, heavily favoring regional techniques when possible. Regional anesthesia has been shown to reduce intraoperative blood loss, lower the incidence of deep vein thrombosis, and provide superior early postoperative pain control. Furthermore, hypotensive epidural anesthesia can significantly reduce cancellous bone bleeding, which is a critical factor in achieving a dry bone bed essential for optimal PMMA interdigitation.

Patient positioning depends entirely on the surgeon's chosen approach. For the ubiquitous posterior approach, the patient is placed in the lateral decubitus position. Rigid pelvic fixation using peg boards or specialized positioners is absolute; any undetected intraoperative shifting of the pelvis will directly compromise the surgeon's ability to accurately judge acetabular version and inclination. Bony prominences, particularly the peroneal nerve at the fibular head and the axilla of the dependent arm, must be meticulously padded to prevent neuropraxias.
The operative field is prepped and draped using strict aseptic technique. We utilize iodine-impregnated adhesive drapes to isolate the skin edges. Prophylactic intravenous antibiotics, typically a first-generation cephalosporin, must be administered within one hour prior to the skin incision to ensure adequate tissue concentrations during the procedure. Only when the patient is perfectly positioned, secured, and prepped do we proceed with the surgical exposure.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a cemented THA is an exercise in meticulous, uncompromising technique. The survival of the reconstruction relies entirely on the integrity of the bone-cement interface and the cement-prosthesis interface. Modern third-generation cementing techniques have dramatically reduced the incidence of aseptic loosening, transforming cemented femoral fixation into one of the most reliable procedures in all of surgery.
The Surgical Approach
While the anterolateral, direct anterior, and posterior approaches can all be utilized for cemented THA, the posterior approach remains the most widely taught and utilized due to its extensile nature and excellent visualization of the proximal femur. The incision is centered over the posterior aspect of the greater trochanter, curving proximally in line with the fibers of the gluteus maximus. The fascia lata and gluteus maximus fascia are incised, and the gluteus maximus fibers are bluntly split.
Deep to the maximus, the short external rotators (piriformis, gemelli, obturator internus) are identified. These are tagged and detached close to their insertion on the greater trochanter, reflecting them posteriorly to protect the sciatic nerve. A complete capsulectomy or a robust capsulotomy is performed to expose the joint. The hip is then dislocated with a combination of flexion, adduction, and internal rotation.
The femoral neck osteotomy is executed precisely according to the preoperative template, utilizing the lesser trochanter as a constant reference point. A reciprocating or oscillating saw is used, taking care to protect the surrounding soft tissues with retractors. Once the femoral head is removed, the acetabulum is exposed by placing a retractor anteriorly over the anterior lip, one inferiorly beneath the transverse acetabular ligament, and one posteriorly.
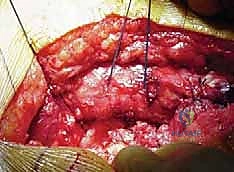
Acetabular Preparation and Cementation
Preparation of the acetabulum for a cemented all-polyethylene component requires a fundamentally different philosophy than press-fit preparation. The goal is not to achieve a tight equatorial scratch-fit, but rather to create a hemispherical bed of bleeding, supportive subchondral bone that can interlock with the PMMA. We begin by clearing the cotyloid fossa of all soft tissue and osteophytes to identify the true medial wall. Reaming is performed sequentially, increasing in size until all remaining cartilage is removed and a bleeding subchondral bed is exposed. We intentionally avoid over-reaming, which would destroy the crucial subchondral plate.

To enhance cement interdigitation, multiple keyholes (typically 3 to 5) are drilled into the ilium, ischium, and pubis using a specialized drill bit. The bone bed is then vigorously cleansed using pulsatile lavage to remove all marrow, fat, and debris, which would otherwise interpose between the bone and the cement. The acetabulum is packed with epinephrine-soaked sponges or hydrogen peroxide to achieve strict hemostasis. A dry bone bed is the absolute prerequisite for successful cementing.

The PMMA is mixed, often utilizing vacuum mixing to reduce porosity and increase the fatigue strength of the cement. When the cement reaches a doughy state, it is introduced into the acetabulum. A pressurizer is immediately applied to force the cement into the trabecular interstices and the prepared keyholes. The all-polyethylene component, typically featuring a peripheral flange to aid in pressurization and PMMA pegs for uniform spacing, is then introduced. It is held firmly in the correct anatomical alignment (typically 40-45 degrees of inclination and 15-20 degrees of anteversion) until the cement is fully polymerized.
Femoral Preparation and Cementing Technique
Femoral preparation begins with identifying the anatomical axis of the medullary canal. A box osteotome is used to remove lateral neck bone, ensuring straight-line access to the canal to prevent varus malpositioning of the stem. The canal is then sequentially broached. Crucially, unlike cementless techniques where broaching continues until cortical chatter is heard, cemented broaching stops when the broach is rotationally stable within the cancellous envelope. We must preserve a 2 to 3 mm layer of strong cancellous bone, as this is the micro-architectural lattice into which the cement will interdigitate.
Once the appropriate size is reached, a trial reduction is performed to confirm leg length, offset, and stability. After trialing, the canal is prepared for cementing. A distal PMMA or polyethylene restrictor (cement plug) is inserted 1 to 2 cm distal to the planned tip of the prosthesis. This plug is essential; it prevents distal migration of the cement, allowing for profound pressurization of the PMMA within the proximal femur. The canal is then aggressively brushed and subjected to high-volume pulsatile lavage to remove all blood and fat. Hemostasis is achieved by packing the canal with a sponge soaked in dilute epinephrine.

Modern third-generation cementing technique dictates the use of vacuum-mixed cement injected retrogradely using a cement gun. The nozzle is placed against the distal restrictor, and as the cement is injected, the gun is slowly withdrawn, ensuring the canal is filled from distal to proximal without entraining air or blood. Once filled, a proximal silicone seal is applied, and the cement is heavily pressurized.

The definitive femoral stem—whether a polished, double-tapered design (like the Exeter, designed to predictably subside and wedge within the mantle) or a composite-beam roughened design—is introduced slowly. The slow insertion allows the viscous cement to flow proximally and interdigitate deeply into the cancellous bed. The stem is held rigidly in neutral alignment until the exothermic polymerization reaction is complete.


Complications, Incidence Rates, and Salvage Management
While cemented THA is highly successful, it is not immune to complications. The introduction of PMMA into the medullary canal carries specific intraoperative risks, and the long-term survival of the implant is threatened by mechanical fatigue and biological reactions to particulate debris. A master surgeon must not only execute the procedure flawlessly but also anticipate, recognize, and aggressively manage these complications.
Intraoperative and Early Postoperative Complications
Clinical & Radiographic Imaging Archive
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding cemented-total-hip-arthroplasty