Cephalomedullary Nailing for Proximal Femur Fractures: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on cephalomedullary nailing for proximal femur fractures. We'll meticulously cover patient assessment, advanced preoperative planning, precise surgical anatomy, and a granular, step-by-step intraoperative execution. Learn critical techniques, identify potential pitfalls, and manage postoperative care for optimal patient outcomes in complex pertrochanteric and subtrochanteric injuries.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are undertaking a comprehensive exploration of a ubiquitous yet technically demanding injury: the proximal femur fracture, specifically focusing on its stabilization via cephalomedullary nailing. This procedure, while routinely performed in trauma centers globally, demands an uncompromising standard of precision, a profound three-dimensional anatomical understanding, and meticulous surgical technique. We will deconstruct this procedure step by step, analyzing the biomechanical rationale and intraoperative decision-making processes as if you are scrubbed in directly across the table from me.
The epidemiological burden of proximal femur fractures represents a looming crisis in global orthopedic traumatology. With an aging demographic, the incidence of osteoporotic fragility fractures is escalating exponentially, projecting millions of cases annually worldwide by the mid-21st century. These injuries are associated with a staggering one-year mortality rate that historically hovers between twenty and thirty percent, heavily influenced by the patient’s pre-injury comorbidities, time to surgical intervention, and the efficacy of post-operative mobilization. Consequently, our surgical mandate extends far beyond mere osteosynthesis; it is fundamentally an act of physiological rescue, aiming to restore ambulatory capacity and mitigate the catastrophic cascade of prolonged recumbency.
Historically, the evolution of internal fixation for these fractures has transitioned from extramedullary devices, such as the sliding hip screw (SHS), to intramedullary load-sharing constructs. While the SHS remains a viable option for stable, two-part intertrochanteric fractures, the cephalomedullary nail has emerged as the gold standard for unstable fracture patterns, reverse obliquity configurations, and subtrochanteric extensions. The intramedullary position of the nail offers a mechanically superior construct by shortening the lever arm between the implant and the mechanical axis of the lower extremity, thereby reducing bending moments and minimizing the risk of implant failure in highly comminuted or osteopenic bone.

Before we even consider a scalpel, we must appreciate the vast spectrum of proximal femur fractures, which are broadly categorized based on their anatomical location and their profound biomechanical implications. Intracapsular fractures, encompassing the femoral head and neck, are biologically precarious due to their reliance on the tenuous medial femoral circumflex artery, making avascular necrosis and nonunion significant concerns. Extracapsular fractures, including pertrochanteric (intertrochanteric) and subtrochanteric variants, occur in a robustly vascularized metaphyseal-diaphyseal envelope but are subjected to massive deforming muscle forces. Our focus today, and the primary indication for cephalomedullary nailing, resides squarely in mastering the extracapsular pertrochanteric and subtrochanteric domains.
Detailed Surgical Anatomy and Biomechanics
Osteology and Vascular Considerations
The proximal femur is a marvel of biomechanical engineering, designed to transmit immense loads from the axial skeleton to the lower appendicular skeleton. The trabecular architecture, notably the primary compressive and primary tensile trabeculae, intersects to form a dense network of structural support, with Ward’s triangle representing a central area of relative osteopenia. The calcar femorale, a dense vertical plate of bone originating posteromedially in the proximal shaft and radiating proximally toward the posterior aspect of the greater trochanter, serves as a critical buttress. Restoring the continuity of the medial cortex and the calcar is paramount for construct stability; failure to do so places excessive, often insurmountable, stress on the cephalomedullary implant.
Vascularly, while extracapsular fractures do not typically jeopardize the viability of the femoral head in the same manner as intracapsular fractures, understanding the regional blood supply is critical for optimizing fracture healing. The profound femoral artery gives rise to the medial and lateral circumflex femoral arteries, which form an extracapsular arterial ring at the base of the femoral neck. The robust muscular envelope surrounding the subtrochanteric region provides an excellent blood supply for secondary bone healing (callus formation), provided the surgeon respects the soft tissues and employs biologically friendly, minimally invasive reduction and insertion techniques.



Deforming Forces and Biomechanical Principles
To achieve and maintain an anatomical reduction, the orthopedic surgeon must intimately understand the muscular forces acting upon the proximal femur fragments. In subtrochanteric and unstable pertrochanteric fractures, the proximal fragment is invariably driven into flexion, external rotation, and abduction. Flexion is driven by the iliopsoas tendon inserting onto the lesser trochanter; external rotation is dictated by the short external rotators inserting into the piriformis fossa and intertrochanteric crest; and abduction is powered by the gluteus medius and minimus inserting onto the greater trochanter. Conversely, the distal diaphyseal fragment is typically drawn proximally and into adduction by the massive adductor musculature, creating the classic varus and shortened deformity.
The biomechanical superiority of the cephalomedullary nail in unstable patterns lies in its load-sharing capacity. By residing within the medullary canal, the nail is positioned significantly closer to the body's center of gravity and the mechanical axis of the limb compared to an extramedullary plate. This proximity drastically reduces the bending moment applied to the implant. Furthermore, intramedullary devices act as internal splints, allowing for controlled axial micromotion and impaction at the fracture site upon weight-bearing, which stimulates robust secondary bone healing. However, this mechanical advantage is entirely dependent on meticulous surgical execution, particularly regarding entry point selection and the precise placement of the proximal fixation element within the femoral head.


Exhaustive Indications and Contraindications
Selecting the Appropriate Patient and Implant
The decision to proceed with cephalomedullary nailing must be predicated on a rigorous analysis of the fracture morphology, the patient's physiological reserve, and the inherent limitations of the available implant systems. While the indications for intramedullary nailing have expanded significantly over the past two decades, it is not a panacea for all proximal femur fractures. The surgeon must carefully weigh the benefits of a minimally invasive, load-sharing device against the technical complexities of intramedullary instrumentation, particularly in cases involving severe anatomical distortion or extremely narrow medullary canals.
For complete, displaced proximal femur fractures in ambulatory adults, nonoperative treatment is virtually obsolete, relegated only to patients who are medically unfit for any form of anesthesia or those at the absolute end of life where palliation is the sole objective. The natural history of an untreated displaced hip fracture is invariably significant shortening, severe varus deformity, chronic pain, and profound functional impairment. Even with state-of-the-art surgical treatment, functional recovery in the geriatric population can be arduous. Our ultimate goal is to provide rigid, stable fixation that permits immediate weight-bearing, thereby facilitating early mobilization and maximizing the patient's potential to return to their pre-injury baseline.




| Category | Specific Conditions | Rationale / Notes |
|---|---|---|
| Primary Indications | Unstable intertrochanteric fractures (AO/OTA 31-A2, A3) | Loss of posteromedial support necessitates a load-sharing IM device. |
| Reverse obliquity fractures | Extramedullary devices fail due to lateral wall blowout and medial displacement forces. | |
| Subtrochanteric fractures | High bending moments in the subtrochanteric region require the mechanical advantage of an IM nail. | |
| Pathologic proximal femur fractures | Prophylactic or therapeutic stabilization of metastatic lesions, often requiring long nails to protect the entire diaphysis. | |
| Relative Contraindications | Stable, two-part intertrochanteric fractures (AO/OTA 31-A1) | A sliding hip screw (SHS) is equally effective, cheaper, and avoids violating the medullary canal and abductor mechanism. |
| Extremely narrow medullary canals | May require excessive reaming, risking iatrogenic fracture or thermal necrosis. | |
| Pre-existing severe femoral deformity | Excessive femoral bowing or prior hardware may preclude safe passage of a straight or standard-bowed nail. | |
| Absolute Contraindications | Active deep infection at the surgical site | Introducing hardware into an infected field guarantees chronic osteomyelitis. |
| Displaced intracapsular femoral neck fractures (in most cases) | High risk of AVN and nonunion; typically treated with arthroplasty (THA or hemi) in older adults, or specialized cannulated screws/DHS in young patients. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Diagnostic Imaging
Our surgical journey begins long before the patient crosses the threshold of the OR. A comprehensive history is paramount. We must meticulously discern the mechanism of injury: a low-energy ground-level fall in an osteoporotic octogenarian tells a vastly different physiological story than a high-energy motor vehicle collision in a robust thirty-year-old. In high-energy scenarios, the orthopedic surgeon must maintain a high index of suspicion for associated, potentially life-threatening injuries, strictly adhering to ATLS protocols. For the elderly patient, it is critical to investigate potential syncopal episodes, which might unmask underlying, untreated cardiovascular or neurological pathologies. Furthermore, a history of malignancy, including recent screenings, is crucial to rule out a pathologic fracture, which would drastically alter our implant choice and biological management.
On physical examination, a displaced extracapsular hip fracture classically presents with profound shortening of the affected extremity and a marked external rotation deformity compared to the contralateral limb. Pain and crepitance are elicited with any attempted motion of the hip joint. Do not neglect the Lippmann test: auscultating the symphysis pubis or greater trochanter with a stethoscope while placing a vibrating tuning fork on the patella. Decreased tone or pitch transmission suggests a bony discontinuity, confirming a fracture. Always meticulously inspect the skin integrity, actively searching for lacerations, Morel-Lavallée lesions, or pre-existing decubitus ulcers that could dictate our surgical approach or increase the risk of perioperative infection.

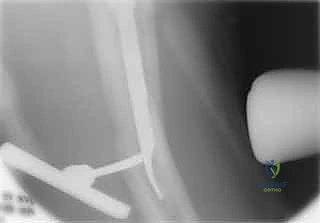




Our diagnostic workup relies heavily on high-quality plain radiographs. An AP pelvis view is essential for comparison with the uninjured contralateral side and for assessing overall pelvic ring integrity. AP and cross-table lateral views of the affected hip are the absolute workhorses for diagnosis, fracture classification, and initial surgical planning. Crucially, AP and lateral radiographs of the entire affected femur down to the knee joint are non-negotiable if we are considering a long cephalomedullary nail. These full-length views allow us to meticulously assess the anterior femoral bow, the medullary canal diameter at the isthmus, and any distal deformities, thereby preventing catastrophic distal anterior cortical penetration during nail insertion.
Classification Systems and Templating
Translating two-dimensional imaging into a three-dimensional surgical blueprint is the essence of preoperative templating. While numerous classifications exist (Evans, Kyle, AO/OTA), the Russell-Taylor classification remains exceptionally pragmatic for guiding implant selection in proximal femoral nailing. Group I fractures feature an intact greater trochanteric region. Type IA are essentially high diaphyseal fractures, often amenable to standard interlocking nails. Type IB fractures involve the diaphyseal-metaphyseal junction with medial instability but an intact lateral wall, making them ideal candidates for standard cephalomedullary nails via a trochanteric or piriformis entry.
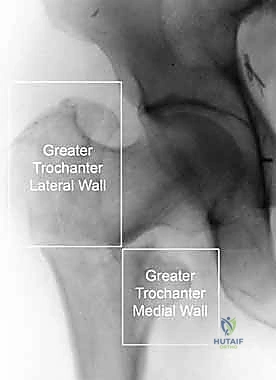
Group II fractures are significantly more challenging, characterized by extension into the greater trochanter. Type IIA fractures involve the greater trochanter and lateral wall but permit restoration of medial cortical stability. Reverse obliquity patterns frequently fall into this category. If the greater trochanter is massively displaced, open reduction and stabilization may be required, and trochanteric portal nails are generally preferred. Type IIB fractures represent the most unstable configuration, with profound involvement of the greater trochanteric region and complete loss of medial cortical stability. These demand masterful reduction techniques and robust trochanteric cephalomedullary nails, or occasionally, conversion to fixed-angle plate constructs if intramedullary stability cannot be guaranteed.




Templating dictates our precise implant selection. We must determine nail length (short vs. long), nail diameter (measuring the narrowest part of the isthmus and subtracting 1-1.5mm to accommodate reaming), and the appropriate neck-shaft angle (typically 125, 130, or 135 degrees) to match the patient's native anatomy. The entry portal is a critical decision. Piriformis portal nails, often associated with reconstruction-style nails, have a straight proximal shaft in the AP plane. Trochanteric portal nails (e.g., Gamma3, TFNA, InterTAN) feature a lateral bend (typically 4 to 5 degrees) to accommodate entry through the tip or slightly medial to the tip of the greater trochanter. Finally, we must select our femoral head fixation strategy, choosing between traditional single lag screws, integrated dual-screw systems (like the InterTAN), or spiral blade devices, depending on bone density and rotational stability requirements.
Patient Positioning and Operating Room Setup
Proper patient positioning is arguably the most critical step before the incision; a poor setup guarantees a difficult operation. The patient is typically placed supine on a radiolucent fracture table. The operative leg is secured in a traction boot, while the contralateral leg is either scissored (extended and dropped posteriorly) or placed in a hemi-lithotomy position to allow unobstructed access for the C-arm fluoroscope. The C-arm must be positioned to effortlessly obtain perfect AP and true lateral views of the proximal femur and femoral neck without moving the base of the machine, relying solely on orbital rotation.
Traction is applied incrementally to restore length, while the leg is internally rotated (usually 10 to 15 degrees) to correct the external rotation deformity and bring the femoral neck parallel to the floor, optimizing the lateral fluoroscopic view. The torso should be adducted slightly away from the operative side to allow clear access to the proximal entry point, preventing the guidewire and reamers from impinging on the patient's flank. Before prepping and draping, the surgeon must verify that acceptable closed reduction has been achieved on both AP and lateral fluoroscopic views. If closed reduction is inadequate, the surgeon must be fully prepared to execute percutaneous joystick techniques or formal open reduction.





Step-by-Step Surgical Approach and Fixation Technique
Achieving Anatomical Reduction
I cannot overstate this fundamental orthopedic truth: a poorly reduced fracture cannot be salvaged by a perfectly placed implant. The cephalomedullary nail is a stabilization device, not a reduction tool. Prior to any incision, meticulous attention must be paid to achieving an anatomical or slightly valgus reduction on the AP view, and a collinear reduction on the lateral view. Mild valgus impaction is mechanically stable and acceptable; varus reduction is a biomechanical disaster that drastically increases the risk of implant cut-out and failure.
If closed traction and internal rotation fail to achieve reduction, we immediately escalate to percutaneous techniques. A Steinmann pin or a Schanz pin can be inserted into the proximal fragment as a joystick to correct flexion and rotation. For stubborn anterior translation of the proximal fragment on the lateral view, a blunt bone tamp or a crutch placed anteriorly can provide the necessary downward force. If these percutaneous maneuvers fail, do not hesitate to make a small lateral incision to utilize a collinear clamp, a pointed reduction forceps, or a bone hook to manually manipulate the fragments. Only when the reduction is deemed perfect on biplanar fluoroscopy do we proceed to the entry point.




Establishing the Entry Point and Canal Preparation
The incision is typically made 3 to 5 centimeters proximal to the greater trochanter, in line with the femoral shaft. The fascia lata is incised, and the abductor musculature is split bluntly to access the tip of the trochanter. For modern trochanteric nails, the ideal entry point is located precisely at the tip of the greater trochanter or slightly medial to it on the AP view, and centered perfectly in the anterior-posterior dimension on the lateral view. A lateral entry point is a critical error; it forces the nail into varus upon insertion, distracting the medial cortex and setting the stage for catastrophic failure.
Once the entry point is localized with a guide pin, an opening reamer is used to breach the proximal cortex. The ball-tipped guidewire is then passed down the medullary canal, ensuring it remains central within the distal fragment and does not inadvertently pass out of a fracture gap. Reaming is performed sequentially, usually 1.0 to 1.5 millimeters larger than the selected nail diameter, to prevent excessive hoop stresses during insertion. The surgeon must listen carefully to the "chatter" of the reamer; excessive resistance indicates the need to downsize the reamer or slow the advancement rate to prevent iatrogenic thermal necrosis or cortical blow-out.



Nail Insertion and Proximal Fixation
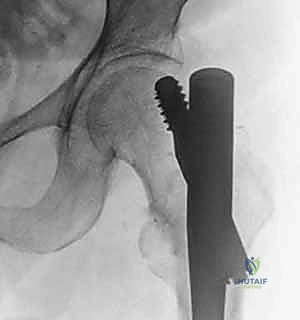
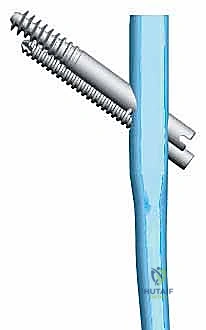
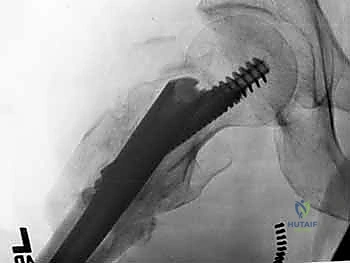
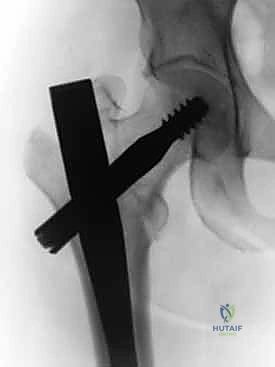
The selected cephalomedullary nail is mounted to the targeting jig and inserted manually over the guidewire. Avoid heavy mallet strikes; the nail should slide smoothly into the reamed canal. If significant resistance is encountered, remove the nail, re-evaluate the reduction, and consider additional reaming. The depth of insertion is critical and is dictated by the planned trajectory of the proximal fixation screw into the femoral head. The targeting arm should align the guide pin for the lag screw perfectly into the lower half of the femoral neck on the AP view, and centrally within the femoral head on the lateral view.
The concept of Tip-Apex Distance (TAD), popularized by Baumgaertner, is the most critical predictor of lag screw cut-out. The TAD is the sum of the distance from the tip of the lag screw to the apex of the femoral head on both the AP and lateral radiographs, corrected for magnification. A TAD of less than 25 millimeters is the gold standard and drastically reduces the risk of mechanical failure. The lag screw or helical blade is inserted over the guide pin, ensuring it is advanced to within 5 to 10 millimeters of the subchondral bone. Once optimal position is confirmed, the traction is released slightly, and the lag screw is compressed to close the fracture gap, providing rigid, stable fixation.





Distal Locking and Final Fluoroscopic Verification
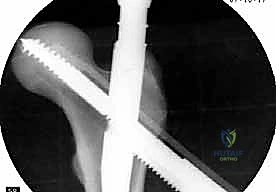
Distal locking is essential to control rotation and maintain length, particularly in unstable patterns or subtrochanteric extensions. Depending on the fracture morphology, the surgeon may choose static locking (preventing any axial translation) or dynamic locking (allowing controlled axial sliding to promote fracture impaction). Modern targeting jigs are highly accurate for short nails, allowing percutaneous placement of distal interlocking screws. For long nails, freehand technique utilizing the "perfect circles" fluoroscopic method is required to accurately target the distal holes.
Following the placement of all interlocking screws, a meticulous final fluoroscopic survey is mandatory. The surgeon must obtain perfect AP and lateral views of the hip, ensuring the TAD remains optimal, the fracture reduction is maintained, and there is no intra-articular penetration of the hardware. The entire length of the femur must be scanned to verify the integrity of the distal cortex and ensure no iatrogenic fractures occurred during nail insertion. The wounds are then copiously irrigated and closed in a layered fashion, paying particular attention to a watertight fascial closure to minimize hematoma formation.




Complications, Incidence Rates, and Salvage Management
Mechanical Failures and Hardware Complications
Despite advancements in implant design and surgical technique, complications following cephalomedullary nailing remain a formidable challenge. The most dreaded mechanical complication is implant cut-out, where the proximal lag screw or blade migrates through the superior aspect of the femoral head, destroying the articular cartilage. Cut-out occurs in approximately 2% to 6% of cases and is almost exclusively the result of a poor initial reduction (varus malalignment) or an unacceptable Tip-Apex Distance (>25mm). When cut-out occurs, the joint is compromised, and salvage typically necessitates conversion to a total hip arthroplasty (THA), a highly complex procedure given the compromised abductor mechanism and proximal bone loss.
Another significant mechanical issue is the "Z-effect" and "reverse Z-effect," phenomena unique to dual-screw cephalomedullary systems. In the Z-effect, the inferior
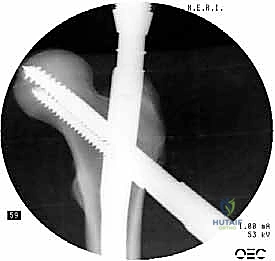
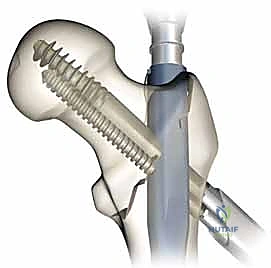
Clinical & Radiographic Imaging Archive