Mastering the Chiari Medial Displacement Osteotomy: An Intraoperative Masterclass for Acetabular Dysplasia

Key Takeaway
This intraoperative masterclass details the Chiari medial displacement osteotomy for painful, unstable hip dysplasia. We cover comprehensive anatomy, meticulous preoperative planning, and granular, real-time surgical execution. Learn precise osteotomy techniques, neurovascular protection, and crucial pearls for optimal femoral head coverage and stability. Understand postoperative rehabilitation and complication management to achieve stable, pain-free hip function.
Comprehensive Introduction and Patho-Epidemiology
The Chiari medial displacement osteotomy of the pelvis remains one of the most intellectually fascinating and biomechanically profound salvage procedures in the armamentarium of the modern orthopedic hip surgeon. Originally described by Karl Chiari in 1955, this operation was designed not to restore normal anatomy, but to fundamentally alter the biomechanical environment of a dysplastic, painful, and often subluxated hip. It is primarily reserved for cases of severe acetabular dysplasia where standard reconstructive rotational osteotomies—such as the Bernese periacetabular osteotomy (PAO) or the Tönnis triple osteotomy—are contraindicated due to advanced arthrosis, severe femoral head asphericity, or inadequate articular cartilage. The Chiari osteotomy is a "salvage" procedure, aiming to delay the inevitable need for total hip arthroplasty (THA) by providing a stable, pain-free articulation through capsular interposition and mechanical medialization.
The pathophysiology of the conditions necessitating a Chiari osteotomy is complex and multifactorial. Most commonly, surgeons encounter developmental dysplasia of the hip (DDH) that has progressed to a state of painful subluxation. In these hips, the primary deficiency is typically located in the anterior and anterolateral acetabulum. However, the procedure is equally critical in the management of spastic hip dysplasia—often seen in patients with cerebral palsy—where the deficiency is predominantly lateral and posterolateral due to the relentless pull of spastic adductor and flexor musculature. Furthermore, the Chiari osteotomy is a powerful tool in the late sequelae of Legg-Calvé-Perthes disease (LCPD), where the surgeon is confronted with a severely deformed, enlarged (coxa magna), or flattened (coxa plana) femoral head that simply cannot be contained by a standard rotational reorientation of the native acetabulum.
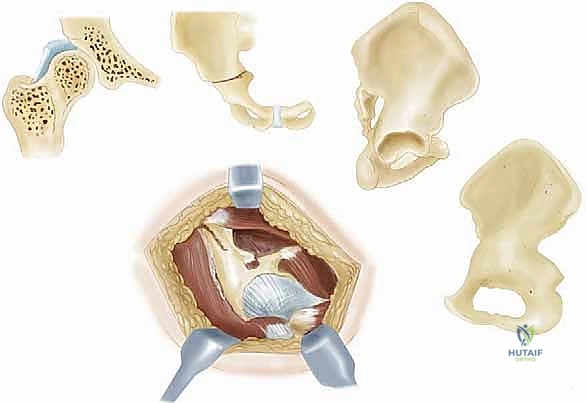
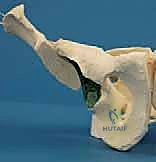
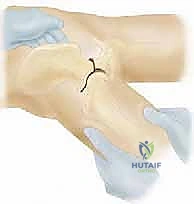
The genius of the Chiari osteotomy lies in its dual mechanism of action: biomechanical medialization and biological metaplasia. By performing a single pericapsular osteotomy through the ilium just superior to the acetabulum, and subsequently displacing the distal fragment (containing the acetabulum and the lower extremity) medially, the surgeon dramatically alters the joint's biomechanics. Medialization of the hip center of rotation decreases the lever arm of the body weight and simultaneously increases the effective lever arm of the hip abductors. This profoundly reduces the joint reactive forces across the hip.
Biologically, the procedure relies on the interposition of the superior hip capsule between the newly created overhanging iliac bony shelf and the femoral head. Under the influence of compressive weight-bearing forces, this highly vascularized capsular tissue undergoes a remarkable metaplastic transformation into dense fibrocartilage. This neo-articulation provides a congruent, load-bearing surface that stabilizes the femoral head, prevents further lateral subluxation, and significantly reduces the patient's pain profile. Understanding this reliance on capsular metaplasia is critical; it dictates that the joint capsule must never be violated or opened during the surgical approach, lest the biological foundation of the procedure be compromised.
Historical Context and Evolution of the Technique
Karl Chiari’s initial description utilized a straight osteotome, which often resulted in a flat, horizontal shelf that did not perfectly contour to the spherical (or aspherical) nature of the femoral head. Over the decades, the technique evolved. The introduction of the Gigli saw allowed for a curved osteotomy that better matched the contour of the capsular dome, providing a more congruent shelf. Furthermore, the understanding of the osteotomy's angulation has been refined. It is now universally accepted that the osteotomy must be angled 10 to 15 degrees cephalad. This upward angulation ensures that as the distal fragment is displaced medially, the newly created shelf slopes slightly downward, effectively preventing the femoral head from escaping laterally under load.
Detailed Surgical Anatomy and Biomechanics
Mastering the Chiari osteotomy requires an intimate, three-dimensional understanding of the pelvic anatomy, specifically the ilium, the sciatic notch, and the intricate neurovascular networks that traverse this region. The operation is performed on the outer (gluteal) and inner (pelvic) surfaces of the ilium, demanding precise dissection to avoid catastrophic complications. The primary landmarks include the anterior superior iliac spine (ASIS), the anterior inferior iliac spine (AIIS), the iliac crest, and the superior rim of the acetabulum. The osteotomy itself must be positioned precisely between the superior reflection of the hip joint capsule and the inferior border of the sacroiliac joint, aiming directly toward the greater sciatic notch.
The muscular intervals utilized for this approach typically involve a modified Smith-Petersen or an anterolateral Watson-Jones approach. Anteriorly, the surgeon develops the interval between the tensor fascia lata (innervated by the superior gluteal nerve) and the sartorius (innervated by the femoral nerve). Deep to this, the dissection proceeds between the gluteus medius and minimus laterally, and the rectus femoris medially. The rectus femoris, with its straight head originating from the AIIS and its reflected head originating from the superior acetabular rim and capsule, is a critical structure. The reflected head must be meticulously elevated or released to expose the superior joint capsule, which serves as the absolute inferior limit of the osteotomy.
Neurovascular vigilance is the hallmark of a master pelvic surgeon. The lateral femoral cutaneous nerve (LFCN) is the most frequently injured structure during the superficial dissection. It pierces the fascia lata near the ASIS and exhibits significant anatomic variability; it must be identified, mobilized, and protected to prevent debilitating meralgia paresthetica. Medially, the femoral nerve and vessels reside within the femoral triangle. While not directly in the path of the osteotomy, aggressive medial retraction or an uncontrolled medial break of the osteotome can jeopardize these structures.
Posteriorly, the anatomy becomes even more perilous. The superior gluteal nerve and vessels exit the pelvis through the greater sciatic notch, superior to the piriformis muscle. They course anteriorly between the gluteus medius and minimus. The osteotomy aims just inferior to their exit point, but errant retractor placement in the sciatic notch can cause compression or laceration, leading to catastrophic abductor paralysis. Inferiorly, the sciatic nerve exits the greater sciatic notch below the piriformis. When passing a Gigli saw or blunt retractors through the notch, the surgeon must stay strictly subperiosteal to ensure the sciatic nerve is protected by the bone and periosteum. The biomechanical success of the operation hinges on achieving at least 50% medial displacement of the distal fragment relative to the iliac width, which optimizes the abductor lever arm while relying on the intact symphysis pubis as a medial hinge.
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of success for the Chiari osteotomy. This procedure is not a prophylactic intervention; it is a meticulously calculated salvage operation. The ideal candidate is an adolescent or young adult (typically under 45 years of age) presenting with a painful, unstable, and subluxated hip secondary to severe dysplasia, where the femoral head is too deformed or the articular cartilage too degraded to permit a reorienting periacetabular osteotomy. In these patients, the goal is to alleviate pain, restore mechanical stability, and postpone the need for a total hip arthroplasty for a decade or more.
The indications encompass a variety of complex pediatric and young adult hip deformities. Advanced developmental dysplasia of the hip (DDH) with a lateralized center of rotation and an uncovering of the femoral head is a classic indication. Similarly, the late stages of Legg-Calvé-Perthes disease often result in a large, mushroom-shaped femoral head (coxa magna) that hinges on the lateral acetabular rim during abduction. A Chiari osteotomy provides the necessary lateral coverage without requiring congruency between the native acetabulum and the deformed head. Neuromuscular hip dysplasia, particularly in ambulatory patients with cerebral palsy, represents another strong indication, as the procedure provides robust mechanical coverage against the persistent lateralizing forces of spastic musculature.
However, the surgeon must be equally aware of the strict contraindications. Severe, bone-on-bone osteoarthritis with complete loss of joint space and profound stiffness is an absolute contraindication; a Chiari osteotomy will not restore motion to a stiff, arthritic hip, and these patients are better served by arthroplasty or arthrodesis. Furthermore, a high dislocation of the hip (e.g., Crowe Type IV DDH) often presents a relative contraindication. In these cases, the femoral head has migrated so far proximally that the ilium above the neo-articulation is excessively thin. An osteotomy in this region will fail to provide a structurally sound bony shelf, leading to inadequate coverage and potential fracture of the proximal fragment.
Indications and Contraindications Matrix
| Category | Specific Conditions | Clinical Rationale / Considerations |
|---|---|---|
| Absolute Indications | Painful DDH with severe asphericity | Native joint cannot be concentrically reduced; salvage required to delay THA. |
| Absolute Indications | Late LCPD (Coxa Magna/Plana) | Hinge abduction present; requires lateral coverage without joint congruency. |
| Absolute Indications | Spastic Hip Dysplasia (Ambulatory) | Provides mechanical block to lateral subluxation driven by spastic adductors. |
| Relative Indications | Failed prior pelvic osteotomy | Used as a secondary salvage when rotational osteotomies have failed or subluxated. |
| Relative Contraindications | Age > 45-50 years | THA provides more reliable, definitive pain relief and functional restoration. |
| Relative Contraindications | High Proximal Dislocation | Iliac bone stock above the femoral head is too thin to create a viable, weight-bearing shelf. |
| Absolute Contraindications | Severe, stiff osteoarthritis | Procedure does not improve ROM; capsular metaplasia requires some baseline mobility. |
| Absolute Contraindications | Active joint infection | Hardware placement and extensive dissection in an infected field is strictly prohibited. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of the Chiari osteotomy is forged in the preoperative planning phase. A comprehensive radiographic evaluation is mandatory. Weight-bearing anteroposterior (AP) views of the pelvis provide a global assessment of pelvic obliquity, limb length discrepancy, and the lateral center-edge angle of Wiberg. A false profile view of the hip is essential for evaluating anterior coverage and the anterior joint space. Crucially, AP views of the hip in maximal abduction and internal rotation must be obtained. These dynamic views identify the presence of "hinge abduction"—a mechanical block where the deformed femoral head levers against the lateral acetabular rim rather than rotating concentrically. If hinge abduction is severe, a concurrent proximal femoral varus osteotomy may be required.

Advanced imaging has revolutionized the planning of pelvic osteotomies. A Computed Tomography (CT) scan with three-dimensional (3D) surface rendering is now considered standard of care. The 3D CT allows the surgeon to visualize the exact topography of the ilium, the thickness of the bone stock available for the shelf, and the precise three-dimensional orientation of the acetabular deficiency. Magnetic Resonance Imaging (MRI), particularly with radial sequencing, is highly recommended to assess the integrity of the labrum, the viability of the articular cartilage, and the condition of the superior joint capsule, which will soon become the new weight-bearing surface.
Templating is performed meticulously using digital software. The surgeon plots the osteotomy starting just superior to the capsular reflection, angling 10 to 15 degrees cephalad in the coronal plane. The degree of expected medial displacement is calculated—typically aiming for 50% to 60% of the iliac width—to ensure adequate coverage of the femoral head. In cases where the femoral head is severely subluxated proximally, a period of preoperative skeletal traction (2 to 3 weeks) may be planned to bring the femoral head down to the level of the true acetabulum, thereby ensuring the osteotomy is performed through thicker, more robust iliac bone.
Operative Suite Setup and Patient Positioning
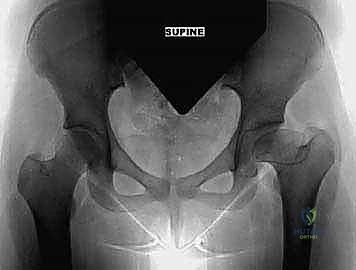
Intraoperative execution relies heavily on optimal patient positioning and unhindered fluoroscopic access. The patient is placed supine on a fully radiolucent Jackson or OSI table. A rolled blanket or a specialized radiolucent bump is positioned under the operative hemipelvis. This slight elevation (approximately 15 to 20 degrees) tilts the pelvis, bringing the lateral aspect of the ilium into better view and facilitating the eventual medial displacement of the distal fragment by allowing gravity to assist in lateralizing the proximal fragment.
Meticulous padding is non-negotiable. The contralateral iliac crest, sacrum, and all peripheral bony prominences must be protected to prevent decubitus ulcers during this lengthy procedure. A Foley catheter is inserted prior to draping; this not only monitors fluid balance but critically decompresses the bladder, protecting it from injury during medial dissection and retractor placement in the true pelvis. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered within 60 minutes prior to skin incision. The C-arm fluoroscopy unit is brought in from the contralateral side, and a sterile drape is applied. The surgeon must verify that perfect AP and obturator oblique views of the operative hemipelvis can be obtained effortlessly before the first incision is made.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with a modified Smith-Petersen (iliofemoral) incision. A bikini-type incision can be utilized for cosmetic purposes in younger patients, following the Langer lines obliquely distal and lateral to the ASIS. Alternatively, a longitudinal incision starting at the anterior half of the iliac crest, extending over the ASIS, and curving distally along the medial border of the tensor fascia lata is highly effective. The superficial fascia is incised, and the interval between the tensor fascia lata and the sartorius is developed. At this juncture, the lateral femoral cutaneous nerve (LFCN) must be meticulously identified, mobilized, and gently retracted medially with a vessel loop to prevent stretch neuropraxia.

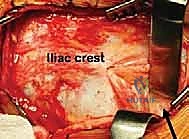
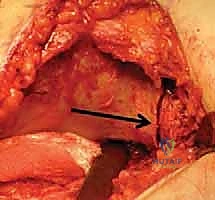
Deep dissection involves elevating the iliac apophysis (in skeletally immature patients) or stripping the periosteum and the origins of the gluteus medius and minimus off the outer table of the ilium. This subperiosteal dissection is carried posteriorly toward the greater sciatic notch. Medially, the iliacus muscle is elevated off the inner table of the ilium, exposing the true pelvis down to the pelvic brim. The rectus femoris is identified; its straight head is detached from the AIIS, and its reflected head is carefully elevated from the superior joint capsule. Crucial technical point: The hip joint capsule must remain absolutely intact. Any violation of the capsule will compromise the metaplastic transformation of the tissue into fibrocartilage, leading to direct bone-on-cartilage wear and rapid failure of the procedure.

Preparation for the osteotomy requires precise retractor placement. Blunt, curved retractors (such as Taylor retractors) are passed strictly subperiosteally into the greater sciatic notch from both the inner and outer tables of the ilium. These retractors meet in the notch, protecting the superior gluteal neurovascular bundle superiorly and the sciatic nerve inferiorly. Fluoroscopy is utilized to confirm the level of the proposed osteotomy. The starting point is exactly at the superior reflection of the capsule. Using a combination of osteotomes and an oscillating saw, or alternatively a Gigli saw passed through the sciatic notch, the osteotomy is initiated.
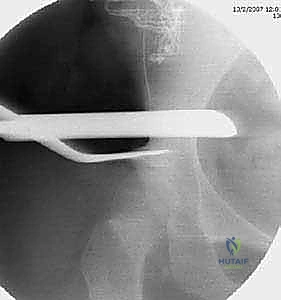


The trajectory of the cut is paramount. It must be directed 10 to 15 degrees cephalad (upward) in the coronal plane. This angle ensures that when the distal fragment is displaced medially, the newly formed shelf slopes downward, mechanically capturing the femoral head and preventing lateral escape. In the sagittal plane, the cut is directed toward the greater sciatic notch, exiting just below the sacroiliac joint. If using a Gigli saw, the surgeon maintains tension and uses long, smooth strokes, ensuring the saw does not bind or deviate distally into the joint.

Once the osteotomy is complete, the critical step of medial displacement begins. The operative leg is abducted, which uses the intact symphysis pubis as a hinge. The surgeon applies direct medial pressure to the greater trochanter or the distal iliac fragment while simultaneously levering the proximal iliac fragment laterally. The goal is to achieve 50% to 60% medial translation of the distal fragment relative to the proximal fragment. Fluoroscopy is utilized to confirm the displacement and ensure the femoral head is adequately covered by the new proximal bony shelf.
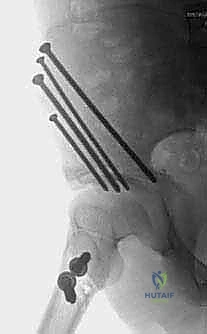
Fixation is achieved to maintain this precise displacement. Typically, two or three stout, fully threaded Steinmann pins or large-fragment cannulated screws are driven from the proximal iliac fragment, across the osteotomy site, and into the dense bone of the distal fragment (the supra-acetabular corridor). Care must be taken to ensure these implants do not penetrate the hip joint.



Once stable fixation is confirmed radiographically, the wound is thoroughly irrigated. The rectus femoris is reattached, and the gluteal muscles and iliacus are sutured back to the iliac crest over a closed suction drain. The superficial tissues and skin are closed in layers.


Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, the Chiari osteotomy is a technically demanding procedure associated with a distinct profile of potential complications. The surgeon must be prepared to identify and manage these intraoperatively and postoperatively. Nerve injury is a primary concern. The lateral femoral cutaneous nerve (LFCN) is the most frequently injured structure, with incidences of meralgia paresthetica reported between 5% and 15%. While often transient, it can cause significant patient dissatisfaction. Sciatic nerve injury is less common (1-3%) but far more devastating, typically resulting from errant retractor placement in the sciatic notch or excessive medial displacement placing tension on the nerve.
Intra-articular penetration of the osteotomy is a catastrophic technical error. If the osteotomy is initiated too far inferiorly, it will violate the superior joint capsule and cut directly into the articular cartilage of the femoral head or the native acetabulum. This destroys the potential for capsular metaplasia and guarantees rapid, painful chondrolysis, often necessitating early conversion to a total hip arthroplasty. Similarly, inadequate medial displacement (less than 30%) fails to optimize the abductor lever arm and provides insufficient coverage, leading to persistent subluxation and failure of the procedure.
Delayed union or nonunion at the osteotomy site occurs in approximately 2% to 5% of cases, more commonly in older patients or those with compromised bone stock. This is usually managed with prolonged protected weight-bearing, but may occasionally require revision internal fixation and autologous bone grafting. Heterotopic ossification (HO) is also a recognized complication, particularly if extensive muscle stripping or a concurrent trochanteric advancement was performed. While severe HO limiting motion is rare, prophylactic measures such as postoperative indomethacin may be considered in high-risk patients.
Complications and Management Matrix
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| LFCN Neuropraxia | 5% - 15% | Superficial dissection near ASIS; aggressive medial retraction. | Identify and protect nerve early. Manage with gabapentinoids; usually resolves spontaneously. |
| Sciatic Nerve Injury | 1% - 3% | Retractor misplacement in sciatic notch; excessive medialization. | Strict subperiosteal retractor placement. If foot drop noted post-op, immediate brace; consider exploration if severe. |
| Intra-articular Osteotomy | < 2% | Starting osteotomy too inferiorly; downward deviation of saw. | Precise fluoroscopic guidance. If recognized intra-op, abort medialization and consider alternative salvage. |
| Inadequate Displacement | 5% - 10% | Failure to mobilize distal fragment; intact medial pelvic fascia. | Ensure complete osteotomy to the notch. Release soft tissues as needed. Aim for >50% displacement. |
| Nonunion / Delayed Union | 2% - 5% | Poor bone stock; inadequate internal fixation; early weight-bearing. | Rigid fixation with stout pins/screws. Treat with prolonged NWB; revision with bone graft if symptomatic >6 months. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a Chiari osteotomy is a delicate balance between protecting the osteotomy site to ensure bony union and initiating early motion to stimulate the critical capsular metaplasia into fibrocartilage. The protocol is rigidly phased and requires strict patient compliance and close monitoring by both the surgical team and specialized physical therapists.
Phase I: Immediate Postoperative Period (Weeks 0-6)
The primary goals in the first six weeks are pain control, wound healing, prevention of deep vein thrombosis (DVT), and protection of the fixation. Patients are typically restricted to toe-touch weight-bearing (TTWB) or completely non-weight-bearing (NWB) on the operative extremity using crutches or a walker. Deep vein thrombosis prophylaxis is mandatory, utilizing low-molecular-weight heparin or direct oral anticoagulants, given the pelvic surgery and altered mobility. Continuous Passive Motion (CPM) machines or gentle, therapist-assisted active-assisted range of motion (AAROM) is initiated immediately. Flexion is typically limited to 90 degrees, and extreme adduction is avoided to prevent undue stress on the osteotomy and the newly forming capsular shelf.
Phase II: Intermediate Healing and Strengthening (Weeks 6-12)
At the six-week mark, AP and lateral radiographs of the pelvis are obtained to assess bridging callus and the stability of the fixation. If radiographic signs of early union are present, the patient is graduated to partial weight-bearing, progressing slowly to full weight-bearing over the next month. This controlled introduction of compressive load is the mechanical trigger required for the superior joint capsule to undergo metaplasia into dense, weight-bearing fibrocartilage. Physical therapy shifts focus toward active range of motion and the initiation of isometric and isotonic strengthening of the hip abductors (gluteus medius and minimus), which are often profoundly weak preoperatively and further inhibited by the surgical approach.
Phase III: Advanced Rehabilitation and Gait Normalization (Months 3-6)
Once full bony union is achieved and the patient is fully weight-bearing, the focus shifts to normalizing gait mechanics and maximizing functional capacity. The Trendelenburg gait, common due to preoperative dysplasia and surgical alteration of the abductor lever arm, is aggressively targeted with advanced closed-kinetic-chain exercises, balance training, and core stabilization. Aquatic therapy is highly beneficial in this phase. The hardware (Steinmann pins or screws) is generally left in situ unless it becomes prominent and symptomatic, in which case removal can be considered after 6 to 12 months. Patients are counseled that maximal medical improvement and the full maturation of the fibrocartilaginous shelf may take up to a year or more.
Summary of Landmark Literature and Clinical Guidelines
The clinical efficacy and long-term survivorship of the Chiari osteotomy are well-documented in the orthopedic literature, cementing its role as a durable salvage procedure. Karl Chiari’s original publications in the 1950s laid the biomechanical foundation, but it is the long-term follow-up studies from major European and North American centers that guide modern clinical decision-making.
Landmark studies by Windhager, Kotz, and others out of the Vienna school have provided the most robust long-term data. Their analyses demonstrate that in properly selected patients—specifically those under the age of 40 with reasonable preoperative hip range of motion and without severe arthrosis—the survivorship of the native hip can exceed 75% at 15 years and 50% at 25 years. This is a profound achievement for a joint that was otherwise destined for imminent arthroplasty. The literature consistently highlights that the degree of medial displacement is directly correlated with long-term success; patients achieving greater than 50% displacement of the iliac width demonstrate statistically significant improvements in pain scores and delayed progression
