Cervical Masterclass: Posterior C1-C2 Fusion with Transarticular and Articular Mass Fixation
Key Takeaway
Welcome, fellows, to an immersive masterclass on posterior C1-C2 fusion. We'll delve into comprehensive atlantoaxial anatomy, meticulous preoperative planning, and precise patient positioning. This session provides a granular, real-time walkthrough of transarticular and articular mass screw fixation, emphasizing critical intraoperative execution, neurovascular precautions, and managing potential pitfalls. Prepare to master this challenging yet rewarding procedure.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater and to this definitive masterclass. Today, we are undertaking a rigorous examination of a critical and unforgiving procedure: posterior C1-C2 fusion and instrumentation utilizing transarticular and articular mass fixation techniques. The upper cervical spine is a region of immense anatomical complexity, demanding not only meticulous surgical precision but also a profound, three-dimensional understanding of regional osteology and neurovascular topography. The atlantoaxial joint is biomechanically unique within the human axial skeleton. It is designed to sacrifice intrinsic osseous stability in favor of an extraordinary range of motion. In a healthy cervical spine, the C1-C2 articulation is responsible for approximately 11.5 degrees of flexion, 10.9 degrees of extension, 6.7 degrees of lateral bending, and a remarkable 38.9 degrees of axial rotation to each side, accounting for nearly 50% of total cervical rotation.
This extensive kinematic profile, while essential for normal human function, renders the atlantoaxial complex highly susceptible to biomechanical failure and subsequent instability. Atlantoaxial instability is a broad, encompassing term that describes a pathological state where the normal anatomical relationships between the atlas and the axis are compromised, leading to aberrant motion under physiological loads. The clinical consequences of this instability exist on a spectrum, ranging from debilitating, intractable suboccipital neuralgia to catastrophic spinal cord compression, high cervical myelopathy, and sudden death due to respiratory arrest from medullary compression.
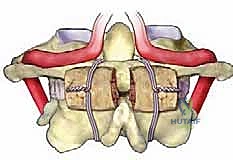
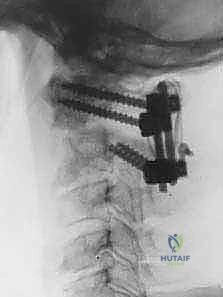
Historically, the surgical management of atlantoaxial instability relied on sublaminar wiring techniques, such as the Gallie, Brooks-Jenkins, and Dickman constructs. While these methods provided tension-band resistance against flexion, they offered universally poor control over axial rotation and extension, necessitating prolonged, highly morbid postoperative halo immobilization and suffering from unacceptably high pseudarthrosis rates. The paradigm shifted dramatically with the introduction of the Magerl transarticular screw technique in 1979, and subsequently, the Harms and Melcher (Goel-Harms) C1 lateral mass and C2 pedicle screw construct in 2001. Our primary objective today is to master these modern, rigid fixation techniques to restore immediate biomechanical stability, facilitate a robust arthrodesis, and definitively protect the neural elements.
The Evolution of Atlantoaxial Fixation
The historical progression of C1-C2 fixation is a testament to the relentless pursuit of biomechanical rigidity in the face of complex anatomy. Early posterior wiring techniques, while foundational, were inherently flawed due to their reliance on intact posterior elements and their inability to neutralize rotational forces. The Gallie technique, utilizing a single midline structural graft secured by a sublaminar wire, provided minimal rotational stability. The Brooks-Jenkins modification improved upon this by utilizing bilateral wedge grafts, yet still required rigid external orthosis.
The advent of the Magerl transarticular screw technique revolutionized the field by crossing the C1-C2 articulation directly, providing unparalleled immediate biomechanical rigidity. This technique effectively neutralized flexion, extension, and, crucially, axial rotation. However, the Magerl technique is technically demanding, requires near-perfect anatomical reduction prior to screw insertion, and is absolutely contraindicated in the presence of an aberrant, high-riding vertebral artery, which occurs in up to 20% of the population.
The introduction of the C1 lateral mass and C2 pedicle/pars screw construct by Goel, and later popularized by Harms and Melcher, offered a modular, highly versatile alternative. This technique decouples the fixation of C1 and C2, allowing for intraoperative reduction of the atlantoaxial joint after screw placement. It is less dependent on preoperative alignment and can be safely executed even in the presence of complex vertebral artery anomalies, provided meticulous preoperative templating is performed. Today, the Harms-Goel technique is widely considered the gold standard, though mastery of both techniques remains essential for the comprehensive cervical spine surgeon.
Pathophysiology of Atlantoaxial Instability
Understanding the underlying pathophysiology driving atlantoaxial instability is paramount for selecting the appropriate surgical intervention. The stability of the C1-C2 joint is entirely reliant on its ligamentous restraints, as the osseous articulations are relatively flat and offer minimal intrinsic resistance to translation. The primary stabilizer is the transverse atlantal ligament, a thick, robust band that spans the inner arch of the atlas, effectively trapping the odontoid process against the anterior arch and preventing anterior translation of C1 on C2.
Disruption of the transverse ligament, whether through acute high-energy trauma, chronic inflammatory degradation (as seen in rheumatoid arthritis), or congenital laxity (such as in Down syndrome or Marfan syndrome), leads to immediate and profound anterior atlantoaxial subluxation. Secondary stabilizers include the alar ligaments, which connect the superolateral aspect of the dens to the medial aspect of the occipital condyles, primarily limiting axial rotation and lateral bending. The apical ligament and the facet capsules provide supplementary, albeit minor, stabilizing forces.
When these ligamentous structures fail, the instantaneous axis of rotation shifts, resulting in abnormal translation during physiological motion. This aberrant motion leads to repetitive microtrauma to the articular cartilage, accelerating degenerative changes, and, more critically, dynamic narrowing of the spinal canal. The resulting mechanical compression of the upper cervical spinal cord and the cervicomedullary junction manifests clinically as myelopathy, characterized by hyperreflexia, gait ataxia, loss of fine motor dexterity, and, in severe cases, quadriparesis and sphincter dysfunction.
Detailed Surgical Anatomy and Biomechanics
Let us now systematically deconstruct the intricate anatomy that makes this region both surgically challenging and intellectually fascinating. A profound, three-dimensional spatial awareness of the osseous and neurovascular structures is the absolute prerequisite for safe instrumentation in the upper cervical spine.
Osteology of the Atlas and Axis
The Atlas (C1): Observe the bony architecture of the first cervical vertebra. The atlas is an evolutionary anomaly; it is entirely devoid of a vertebral centrum (body) and a spinous process, a stark contrast to the subaxial spine. Instead, it forms a complete osseous ring, comprised of a slender anterior arch and a thicker posterior arch, bridged by two massive, wedge-shaped lateral articular masses.
FIG 1 • A. The atlas consists of an anterior and posterior arch connected by two robust articular masses. Note the lack of a vertebral body.
The superior articular facets are concave and kidney-shaped, articulating with the occipital condyles to form the atlanto-occipital joint, which is primarily responsible for cranial flexion and extension (the "nodding" motion). The inferior articular facets are relatively flat and circular, articulating with the axis. On the superior surface of the C1 posterior arch, immediately posterior to the lateral mass, lies a distinct anatomical sulcus. This groove is of paramount surgical importance, as it intimately houses the V3 segment of the vertebral artery, the first cervical nerve root (suboccipital nerve), and a dense, often troublesome, venous plexus. In approximately 15% of the population, this groove is partially or completely ossified, forming a bony bridge known as the ponticulus posticus (or arcuate foramen). Failure to recognize this variant on preoperative CT can lead to catastrophic intraosseous vertebral artery injury during C1 lateral mass screw placement if the arch is mistaken for normal lateral mass anatomy.
The Axis (C2): We now turn our attention to the axis.

FIG 1 • C. Anterior view of the axis, demonstrating the odontoid process projecting upward from the vertebral body.
C2 acts as the transitional vertebra between the highly specialized craniocervical junction and the subaxial spine. It is characterized by thick, robust laminae and a massive, typically bifid spinous process that serves as the primary attachment site for the powerful extensor musculature of the neck (rectus capitis posterior major, obliquus capitis inferior). Its defining morphological feature is the odontoid process, or dens, a peg-like structure projecting superiorly from the vertebral body, acting as the primary pivot point for C1 rotation.
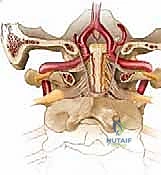
FIG 1 • D. Posterior view of the axis. The pedicle connects the lamina and the vertebral body, projecting superomedially. The pars interarticularis lies between the superior and inferior articular processes.
The osseous anatomy of the C2 lateral mass is complex and frequently misunderstood. The C2 pars interarticularis is defined as the portion of bone connecting the superior and inferior articular processes. The C2 pedicle, conversely, is the anatomical cylinder of bone connecting the posterior elements to the vertebral body, located anterior to the pars. The distinction between a pars screw and a pedicle screw is critical; a pedicle screw requires a more medial and superior trajectory, offering superior biomechanical pull-out strength but carrying a higher risk of vertebral artery injury if the medial wall is breached.
Ligamentous Restraints and Kinematics
As previously established, the integrity of the atlantoaxial joint is dictated by its ligamentous complex. The transverse ligament is the paramount structure. It is a thick, inelastic band of collagenous tissue that arises from a small tubercle on the medial aspect of one C1 lateral mass and traverses posterior to the dens to attach to the contralateral tubercle. It effectively creates an osteoligamentous ring that confines the dens against the fovea dentis of the C1 anterior arch.
The biomechanical threshold for transverse ligament failure is critical knowledge. In an adult, an anterior atlantodental interval (AADI)—the distance between the posterior cortex of the C1 anterior arch and the anterior cortex of the dens—greater than 3.5 mm on a lateral radiograph is highly suggestive of transverse ligament incompetence.
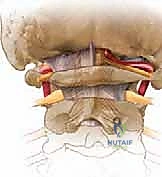
FIG 2 • A. An anterior atlantodental interval greater than 5 mm indicates likely injury to the transverse ligament and necessitates operative stabilization.
When the AADI exceeds 5.0 mm, it implies catastrophic failure not only of the transverse ligament but also of the secondary stabilizers, including the alar and apical ligaments. This degree of displacement is a definitive indication for surgical stabilization, as the spinal cord is at imminent risk of dynamic compression between the posterior aspect of the dens and the posterior arch of C1.
The alar ligaments are robust, paired cords arising from the superolateral aspect of the dens and diverging superiorly and laterally to insert onto the medial aspect of the occipital condyles. They function as the primary check-reins against excessive axial rotation and lateral bending. Unilateral rupture of an alar ligament results in a significant increase in contralateral axial rotation. The apical ligament is a thin, rudimentary structure extending from the tip of the dens to the basion (anterior margin of the foramen magnum) and offers negligible biomechanical stability.
Neurovascular Topography and the Vertebral Artery
The neurovascular anatomy of the atlantoaxial region is notoriously treacherous. The vertebral artery is the single most critical structure to master.

FIG 1 • E & F. The vertebral artery ascends through the foramina transversaria, takes a sharp lateral turn at C2, and courses medially over the C1 ring before entering the foramen magnum.
The artery ascends through the foramina transversaria of the subaxial spine (V2 segment). Upon exiting the C2 foramen transversarium, it takes a sharp, lateral deviation to enter the laterally displaced C1 foramen transversarium. This segment, between C2 and C1, is highly vulnerable during lateral dissection and transarticular screw placement.
After traversing the C1 foramen, the artery (now the V3 segment) curves sharply posteromedially, lying horizontally within the vertebral groove on the superior surface of the C1 posterior arch. It is here that the artery is most at risk during superior subperiosteal dissection of the C1 arch. The artery then pierces the posterior atlanto-occipital membrane and the dura mater to enter the foramen magnum (V4 segment), ultimately joining its contralateral counterpart to form the basilar artery.
The neural elements also demand meticulous respect. The C1 nerve root (suboccipital nerve) is primarily motor, exiting between the occiput and the C1 posterior arch to innervate the suboccipital triangle. The C2 nerve root is unique; it possesses a massive dorsal root ganglion that occupies the space between the posterior arches of C1 and C2, directly posterior to the lateral atlantoaxial joint. It exits posterior to the joint capsule, unlike subaxial roots which exit through a true neural foramen. The dorsal ramus of C2 continues as the greater occipital nerve, providing sensory innervation to the posterior scalp. Mobilization, retraction, or deliberate transection of the C2 nerve root is often required to achieve adequate exposure of the C1-C2 joint for decortication and screw placement, a maneuver that frequently results in postoperative occipital numbness or, less commonly, painful dysesthesia.
Exhaustive Indications and Contraindications
Fellows, technical mastery of screw placement is irrelevant if the surgical indication is flawed. The decision to fuse the atlantoaxial joint must be based on a rigorous assessment of instability, neurological risk, and patient-specific pathoanatomy.
Traumatic Etiologies
Trauma remains a primary indication for C1-C2 arthrodesis. The mechanism of injury typically involves high-energy axial loading, hyperflexion, or hyperextension.
* Transverse Ligament Rupture: As discussed, an AADI > 3.5 mm (or > 5 mm indicating multi-ligamentous failure) is a hallmark of instability.

FIG 2 • B. An avulsion of the transverse ligament from the ring of C1 indicates profound instability.
Mid-substance tears of the transverse ligament (Dickman Type I) possess virtually no healing potential with external orthosis and universally require surgical fusion. Bony avulsions (Dickman Type II) may heal with rigid halo immobilization, but surgery is often preferred to avoid the morbidity of the halo.
* Odontoid Fractures:

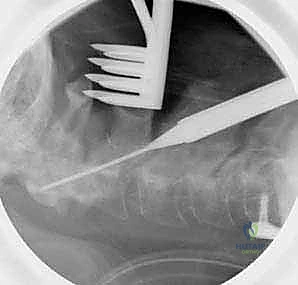
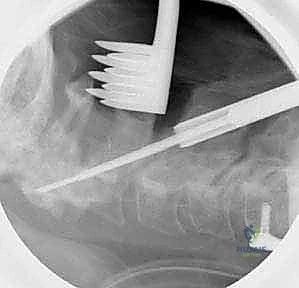
FIG 3 • A. Displaced odontoid fractures (type 2) have a high likelihood of nonunion.
Type II odontoid fractures (fractures through the waist of the dens) are notorious for high nonunion rates due to the watershed vascular supply of the dens and the constant shear forces at the fracture site. Indications for primary posterior C1-C2 fusion in Type II fractures include displacement > 5 mm, angulation > 10 degrees, comminution at the base, inability to achieve or maintain closed reduction, and patient age > 65 years (where nonunion rates approach 50-80% with conservative management). Type III fractures (extending into the C2 body) generally heal well with orthosis, but fusion is indicated if they remain unstable or fail to unite.
* Jefferson Fractures (C1 Ring Fractures): Isolated C1 ring fractures are typically managed conservatively. However, if the lateral masses are displaced outward by more than 6.9 mm on an open-mouth odontoid radiograph (the Rule of Spence), it implies a concomitant rupture of the transverse ligament, necessitating stabilization.
Degenerative Inflammatory and Congenital Pathologies
Nontraumatic etiologies often present insidiously, requiring a high index of suspicion and advanced imaging.
* Rheumatoid Arthritis (RA): The atlantoaxial joint is the most frequently involved spinal segment in RA. Chronic synovial inflammation leads to the formation of a destructive pannus.

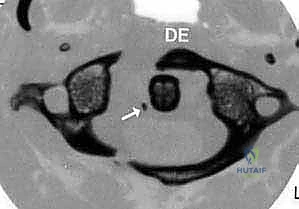
FIG 3 • C. Pseudo-pannus formation behind the dens in RA leads to severe cervical stenosis.
This pannus enzymatically degrades the transverse ligament and the odontoid process, leading to anterior subluxation. In RA, the Posterior Atlantodental Interval (PADI)—the distance from the posterior aspect of the dens to the anterior aspect of the posterior C1 arch—is a more reliable prognostic indicator than the AADI. A PADI < 14 mm is highly correlated with the development of myelopathy and is an absolute indication for surgical decompression and fusion.

FIG 3 • D. Pre-operative MRI showing severe brainstem compression from RA pannus.
Furthermore, vertical subluxation (cranial settling), where the dens migrates proximally through the foramen magnum, poses an immediate threat to the cervicomedullary junction and requires urgent occipitocervical fusion.
* Congenital Anomalies: Conditions such as os odontoideum (an independent ossicle cranial to the axis body) behave biomechanically like an ununited Type II odontoid fracture and frequently require fusion if symptomatic or demonstrating dynamic instability. Down syndrome patients exhibit a high prevalence of ligamentous laxity, necessitating careful screening and potential fusion prior to high-risk activities or general anesthesia.
| Indication Category | Specific Pathology | Radiographic / Clinical Criteria for Fusion |
|---|---|---|
| Trauma | Transverse Ligament Rupture | AADI > 3.5 mm (adult), Dickman Type I tear. |
| Trauma | Odontoid Fracture (Type II) | Displacement > 5mm, angulation > 10°, age > 65, nonunion. |
| Trauma | Jefferson Fracture | Lateral mass overhang > 6.9 mm (Rule of Spence). |
| Inflammatory | Rheumatoid Arthritis | PADI < 14 mm, neurologic deficit, intractable pain. |
| Congenital | Os Odontoideum | Dynamic instability on flexion/extension, myelopathy. |
| Contraindications | Absolute: Active local infection, destruction of target osseous anatomy (e.g., tumor). | Relative: Poor bone quality (osteoporosis requires technique modification), aberrant VA anatomy (dictates technique selection). |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a C1-C2 fusion is largely determined before the skin is even incised. Meticulous preoperative planning is the hallmark of a master surgeon.
Advanced Neuroimaging and Vascular Templating
Standard plain radiographs (AP, lateral, open-mouth, and dynamic flexion-extension views) provide a baseline assessment of alignment and gross instability. However, a high-resolution, thin-cut (1 mm) Computed Tomography (CT) scan with multiplanar reconstructions (sagittal and coronal) is absolutely mandatory for all patients undergoing posterior upper cervical instrumentation.
FIG 4 • A. Preoperative CT scan demonstrating osseous anatomy.
FIG 4 • B. Sagittal reconstruction is vital for evaluating the C2 pedicle trajectory.

FIG 4 • C. Axial CT is used to measure the width of the C2 pedicle.
The CT scan must be scrutinized to evaluate the osseous dimensions of the C1 lateral mass and the C2 pedicle/pars. A C2 pedicle width of less than 4.0 mm is generally considered a contraindication to standard 3.5 mm pedicle screw placement, as it leaves an unacceptably thin cortical margin, risking medial breach (spinal cord) or lateral breach (vertebral artery).
Crucially, a CT Angiogram (CTA) or Magnetic Resonance Angiogram (MRA) must be obtained to delineate the course of the vertebral arteries. The surgeon must specifically look for a "high-riding" vertebral artery, defined as an artery that loops superiorly and medially into the C2 body, severely narrowing the osseous corridor of the C2 pedicle and pars.

FIG 4 • D. CTA demonstrating a high-riding vertebral artery, a contraindication to transarticular fixation on the affected side.
If a high-riding vertebral artery is identified unilaterally, transarticular or pedicle screw placement on that side is absolutely contraindicated. The surgeon must pivot to alternative fixation strategies,
Clinical & Radiographic Imaging Archive