Operative Management of Tendon Ruptures and Synovitis in the Rheumatoid Hand
Key Takeaway
Tendon rupture in the rheumatoid hand is a debilitating complication primarily driven by chronic tenosynovitis and bony attrition. Extensor tendons frequently rupture at the extensor retinaculum due to a dorsally subluxated distal ulna, while flexor tendons often fail secondary to infiltrative synovitis or carpal osteophytes. This guide details evidence-based surgical interventions, including tenosynovectomy, side-to-side tendon transfers, and tension band arthrodesis, optimizing functional outcomes for patients with advanced rheumatoid deformities.
PATHOPHYSIOLOGY OF TENDON RUPTURE IN THE RHEUMATOID HAND
Rupture of tendons is a major cause of profound deformity and functional disability in the rheumatoid hand. The etiology is multifactorial, primarily driven by chronic rheumatoid tenosynovitis. This hypertrophic synovial tissue acts through two distinct pathological mechanisms:
1. Infiltrative Degradation: Enzymatic destruction of the tendon substance by invasive tenosynovium (pannus).
2. Mechanical Attrition: Frictional wear of the tendon against roughened, eroded bony prominences, exacerbated by joint subluxation.
These ruptures can easily be overlooked during initial clinical evaluation, as they are frequently masked by more grotesque, generalized deformities elsewhere in the hand, such as severe ulnar drift, severe metacarpophalangeal (MCP) joint subluxation, or swan-neck deformities.
EXTENSOR TENDON RUPTURE
Extensor tendon ruptures in the rheumatoid patient classically present as a sudden loss of active digit extension, often without antecedent trauma. The long extensor tendons of the middle, ring, and little fingers frequently rupture as a sequential group—a phenomenon clinically recognized as Vaughan-Jackson syndrome.
Biomechanics and Pathoanatomy
Dorsal subluxation of the distal ulna (caput ulnae syndrome) is the primary mechanical contributor to the rupture of these ulnar-sided extensor tendons. As the distal radioulnar joint (DRUJ) is destroyed by synovitis, the distal ulna dislocates dorsally. The diseased, eburnated end of the ulnar head becomes a sharp, abrasive fulcrum. The extensor tendons, tightly constrained by the intact dorsal carpal ligament (extensor retinaculum), are forced to glide directly over this rough bony prominence.
Rupture typically initiates at the extensor digiti minimi (EDM) and progresses radially to involve the extensor digitorum communis (EDC) of the ring, middle, and occasionally index fingers. The extensor pollicis longus (EPL) is also highly susceptible to rupture, typically failing at the level of Lister's tubercle due to a combination of mechanical attrition and ischemic compression within the third dorsal compartment.
Clinical Pearl: Always differentiate a true extensor tendon rupture from a subluxated extensor tendon. In severe MCP joint ulnar drift, the extensor tendons may subluxate into the ulnar valleys between the metacarpal heads, resulting in an inability to actively extend the fingers. If passive extension of the MCP joint allows the patient to maintain extension, the tendon is likely intact but subluxated. If the finger drops, a rupture is present.
Surgical Management of Extensor Ruptures
Direct end-to-end repair of a ruptured rheumatoid tendon is almost universally impossible due to extensive substance loss and retraction. Surgical reconstruction relies on tendon transfers or side-to-side anastomoses to adjacent intact tendons. Furthermore, the underlying bony pathology must be addressed simultaneously (e.g., Darrach procedure or Sauvé-Kapandji procedure for the distal ulna) to prevent rupture of the repair.
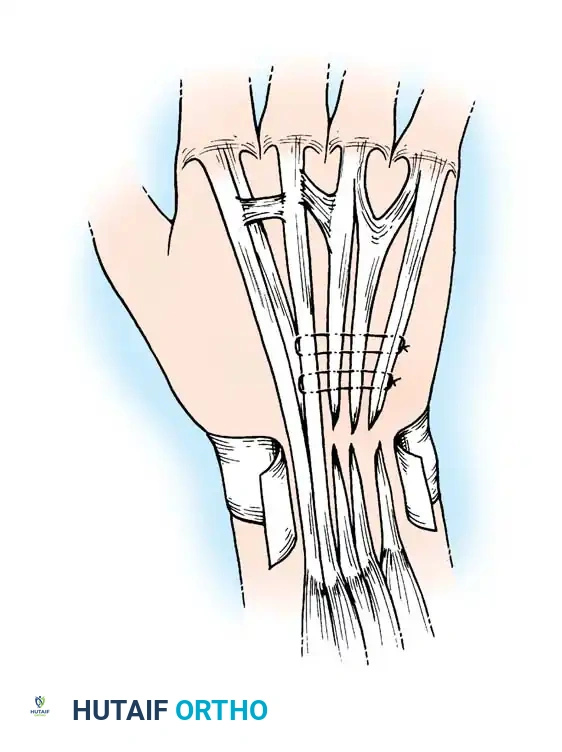
Technique: Side-to-Side Repair
When a single common extensor tendon is ruptured (e.g., EDC to the ring finger), the distal stump of the ruptured tendon can be woven into the adjacent intact EDC tendon of the middle finger.
1. Expose the extensor retinaculum via a dorsal longitudinal or gently curved incision.
2. Identify the ruptured tendon ends. Debride the degenerative proximal stump.
3. Perform a side-to-side anastomosis (pulvertaft weave or robust side-to-side suturing) of the distal stump to the adjacent intact extensor tendon under appropriate tension.
4. Resect the abrasive distal ulna if caput ulnae is present, and perform a dorsal tenosynovectomy.
FLEXOR TENDON RUPTURE
While less common than extensor tendon ruptures, flexor tendon ruptures in rheumatoid patients are significantly more difficult to treat surgically. The functional deficit is profound, and the reconstructive options are limited by the complex anatomy of the flexor fibro-osseous sheath.
Pathoanatomy and Clinical Presentation
Flexor ruptures occur via two primary mechanisms:
1. Wrist Level (Mechanical Attrition): Bony erosion of the tendon over carpal osteophytes. The most classic presentation is the Mannerfelt lesion, where the flexor pollicis longus (FPL) tendon ruptures due to attrition over a sharp osteophyte on the palmar aspect of the scaphoid or trapezium.
2. Digital Level (Infiltrative): Rupture within the digit is usually the result of severe, infiltrative tenosynovitis weakening the tendon substance.
Rupture of a single slip of the flexor digitorum superficialis (FDS) can cause a localized nodule that leads to triggering of the finger. Rupture of the flexor digitorum profundus (FDP) is easily demonstrated by the loss of active distal interphalangeal (DIP) joint flexion, but determining the exact level of the rupture clinically can be challenging. Both FDS and FDP ruptures rapidly lead to secondary joint stiffness.
Surgical Management of Flexor Ruptures
Surgical Warning: Tendon grafts for the reconstruction of ruptured flexor tendons within the digits of rheumatoid patients almost always fail. The scarred, poorly vascularized synovial bed and compromised pulley system preclude successful free tendon grafting.
Exceptions and Alternatives:
* FPL Rupture at the Wrist: A segmental free tendon graft (e.g., palmaris longus) can occasionally be used successfully to bridge an FPL defect at the wrist, provided the carpal floor is smoothed and the osteophytes excised.
* Arthrodesis: For FPL ruptures, arthrodesis of the interphalangeal (IP) joint of the thumb is often the most reliable and functional approach. If both the FDP and FDS are ruptured within a digit, arthrodesis of the proximal interphalangeal (PIP) and DIP joints is the preferred salvage procedure to provide a stable, functional post for pinch and grasp.
FLEXOR TENOSYNOVITIS
Flexor tenosynovitis is a hallmark of the rheumatoid hand. Savill reported that 50% of patients with chronic rheumatoid arthritis exhibit flexor tenosynovitis, while Brewerton reported an incidence as high as 64%.
Clinical Presentation
Although flexor tenosynovitis at the wrist may not be as visually apparent as dorsal extensor swelling, its consequences are severe. The hypertrophic tenosynovium:
* Interferes with tendon excursion, causing a gradual decrease in active finger flexion.
* Compresses the median nerve within the rigid carpal tunnel, leading to secondary carpal tunnel syndrome.
* Leads to eventual tendon rupture.
In the digits, progressive fusiform swelling of the flexor tendon sheaths extends from the mid-palm to the DIP joint. The swelling is painful, and palpation reveals thickened synovium, palpable nodules, and crepitus with tendon excursion. Triggering frequently occurs as tenosynovium or tendon nodules catch on the annular pulleys or at the decussation of the FDS (Camper's chiasm).
Diagnostic Pearl: To differentiate joint stiffness from flexor tenosynovitis, assess passive versus active motion. If passive motion at the PIP joint is significantly greater than active motion, the primary pathology is likely tenosynovitis restricting tendon excursion rather than intra-articular joint destruction.
Synovectomy of the Flexor Tendon Sheaths (Technique 70-11)
Tenosynovectomy has a highly reliable and lasting effect. Brown and Brown reported only 7 recurrences after 173 tenosynovectomies at a mean follow-up of 70 months. Wheen et al. demonstrated that routine excision of the ulnar slip of the FDS further reduces recurrence and reoperation rates by providing more spatial volume for tendon excursion.

Step-by-Step Surgical Technique:
1. Incision: Make a long, discontinuous zigzag (Bruner) incision on the palmar surface of each involved finger, extending into the palm as needed.
2. Exposure: Elevate the skin flaps on each side. Crucial: Avoid damage to the neurovascular bundles, which lie anterolaterally, not strictly laterally.
3. Pulley Management: Expose the flexor tendon sheath. Excise portions of the pathological sheath, but strictly preserve the critical A2 and A4 pulleys. Leave these pulleys at least 1 cm wide at the middle of the proximal and middle phalanges to prevent bowstringing.
4. Synovectomy: Excise as much synovium as possible. Meticulously remove pannus from behind the slips of the FDS and from the interval between the FDP and FDS.
5. Triggering Release: If triggering is present, preserve the first annular (A1) pulley if possible, relying on thorough tenosynovectomy. If triggering persists, the A1 pulley may be released, provided the radial collateral ligament and MCP joint are stable.
6. FDS Slip Excision: To decompress the sheath and provide more room for tendon excursion, excise one slip (typically the ulnar slip) of the flexor digitorum superficialis.
7. Closure: Close the incision with interrupted non-absorbable sutures. Apply a bulky compression dressing and support the wrist with a volar plaster splint, keeping the hand elevated.
Postoperative Protocol:
Motion of the fingers is initiated as soon as tolerated, often within 24 to 48 hours, to prevent restrictive adhesions. Sutures are removed at 10 to 14 days. Supervised physical therapy focusing on active and passive range-of-motion exercises is critical and must continue until maximal excursion is achieved.
PERSISTENT SYNOVITIS OF THE PROXIMAL INTERPHALANGEAL JOINT
When synovitis of the PIP joint remains refractory to medical management, surgical synovectomy is a highly effective joint-preserving operation. It can be performed simultaneously on multiple digits.
Synovectomy of the PIP Joint (Technique 70-10)
- Approach: Make a midlateral incision centered over the PIP joint.
- Retinacular Release: Locate the transverse retinacular ligament, sever its attachment, and elevate the extensor hood dorsally.
- Joint Entry: Identify the collateral ligament. Enter the joint dorsal to this ligament and lateral to the central slip of the extensor tendon.
- Excision: Explore the joint and meticulously excise all visible synovium. Remove pannus from the recess behind the volar plate and inferior to the collateral ligament. If necessary for exposure, the accessory collateral ligament may be divided, but the main proper collateral ligament must be preserved.
- Closure: Relocate the lateral band and repair the transverse retinacular ligament to prevent dorsal subluxation of the lateral bands (which would cause a swan-neck deformity). Close the skin and apply a short arm volar splint.
Postoperative Protocol:
Sutures are removed at 10 to 14 days. Active and passive range-of-motion exercises begin immediately under therapist supervision to prevent stiffness.
ARTHRODESIS OF THE FINGER JOINTS
Arthrodesis is indicated when a joint has been irreversibly destroyed by rheumatoid disease, rendering it painful, grossly deformed, or unstable. In the rheumatoid hand, motion often becomes a liability rather than an asset if it lacks stability.
Indications and Optimal Positioning
Arthrodesis is most frequently employed for the PIP and DIP joints. If the MCP joint is destroyed but the extrinsic and intrinsic musculature remains functional, silicone arthroplasty is generally preferred over arthrodesis to preserve hand span and grasp.
Preferred Angles of Fusion:
* Metacarpophalangeal (MCP) Joint: 20 to 30 degrees of flexion.
* Proximal Interphalangeal (PIP) Joint: Cascading flexion is preferred. Fix the index finger at 25 degrees of flexion, increasing progressively to almost 40 degrees in the small finger. This cascade optimizes grip strength and pinch kinematics.
* Distal Interphalangeal (DIP) Joint: 15 to 20 degrees of flexion.
Fixation Biomechanics
Various internal fixation techniques exist, including crossed Kirschner wires (K-wires), intra-osseous wiring, Herbert screws, and tension band constructs.
Tension band arthrodesis, popularized by Lister and Stern et al., provides exceptional biomechanical stability. It converts dorsal tensile forces (created by active flexion attempts) into volar compressive forces across the arthrodesis site. Stern et al. reported a 97% fusion rate using this technique, making it the gold standard for PIP and MCP joint fusions in osteopenic rheumatoid bone.
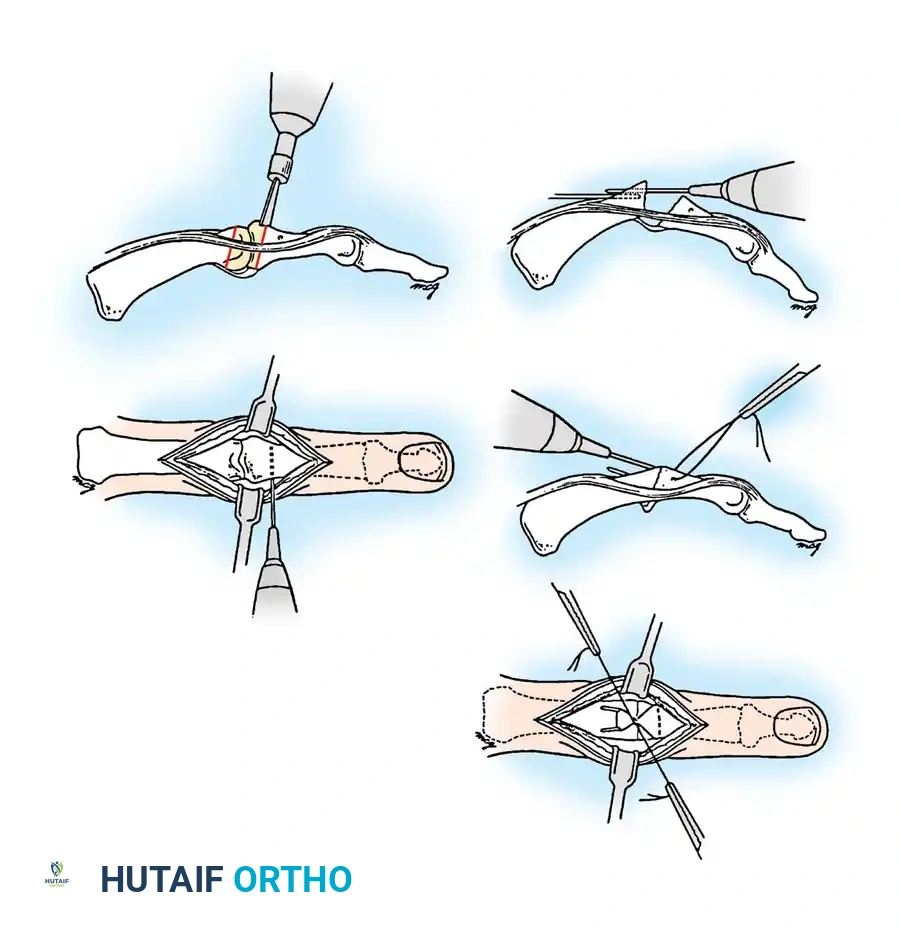
Metacarpophalangeal Joint Arthrodesis (Technique 70-12: Stern et al., Modified)
- Exposure: Make a transverse dorsal incision over the MCP joint. Split the extensor hood and joint capsule longitudinally through the center of the central tendon.
- Preparation: Release the collateral ligaments to allow full joint flexion. Resect all remaining articular cartilage and subchondral bone down to healthy, bleeding cancellous bone.
- Shaping: Shape the articular surfaces using a cup-and-cone reamer system or make flat cuts with an oscillating saw to achieve the desired 20 to 30-degree angle. The cup-and-cone method is preferred as it allows micro-adjustments in rotation and angulation without sacrificing additional bone length.
- Wire Placement: Drill a transverse hole 5 to 10 mm distal to the fusion site in the proximal phalanx, slightly dorsal to the midaxial line. Thread a 25- or 26-gauge stainless steel wire through this hole.
- K-wire Fixation: Drive two 0.028-inch or 0.035-inch K-wires retrograde into the metacarpal, exiting dorsally 10 to 15 mm proximal to the fusion site.
- Compression: Compress the cancellous bone surfaces together, ensuring absolute control of rotation. Drive the K-wires antegrade into the proximal phalanx, seating them firmly in the palmar cortex without penetrating the volar soft tissues.
- Tension Banding: Loop the stainless steel wire around the proximal ends of the K-wires in a figure-of-eight fashion. Tighten the wire with a needle holder to compress the arthrodesis site.
- Finalization: Bend the proximal ends of the K-wires over the steel wire loop and cut them flush to the bone to prevent soft tissue irritation. Close the extensor mechanism and skin.
Proximal Interphalangeal Joint Arthrodesis (Technique 70-13)
- Exposure: Open the joint through a dorsal midline incision. Incise the extensor tendon and capsule longitudinally.
- Release: Release the central slip of the extensor tendon from its insertion on the base of the middle phalanx. Release the collateral ligaments to fully expose the joint surfaces.
- Shaping: Prepare the surfaces using a ball-and-socket reamer or flat osteotomies to achieve the cascade angle (25° index to 40° small finger).
- Fixation: Utilize the tension band technique described above, or alternatively, use one longitudinal 0.045-inch K-wire combined with an interfragmentary intra-osseous wire.
- Closure: Leave the palmar cartilaginous plate intact if possible to act as a volar hinge. Close the dorsal structures securely.
Postoperative Protocol for Arthrodesis:
A protective dorsal splint is applied to block extension. The splint is removed at 3 to 5 days to allow active motion of the adjacent, unfused joints. Skin sutures are removed at 7 to 10 days. Internal fixation is typically left in place permanently unless symptomatic hardware prominence occurs. Serial radiographs are obtained at 4, 8, and 12 weeks to confirm solid bony union, which may take several months in patients with advanced rheumatoid arthritis and systemic immunosuppression.
You Might Also Like


