Trimalleolar Fractures: Comprehensive Operative Management and Surgical Techniques
Key Takeaway
Trimalleolar fractures represent complex ankle injuries involving the medial, lateral, and posterior malleoli, often complicated by talar subluxation. Successful management requires meticulous preoperative planning, including mandatory CT imaging, to assess posterior fragment morphology. Anatomical reduction and rigid internal fixation are paramount, particularly for posterior fragments exceeding 25% of the articular surface or those contributing to syndesmotic instability, ensuring restoration of the ankle mortise and prevention of post-traumatic arthritis.
INTRODUCTION TO TRIMALLEOLAR FRACTURES
Trimalleolar fractures represent one of the most challenging intra-articular injuries managed by orthopedic surgeons. These injuries require open reduction and internal fixation (ORIF) more frequently than any other type of ankle fracture pattern. Despite meticulous surgical intervention, the clinical and functional results of treating trimalleolar fractures are historically not as favorable as those obtained for bimalleolar or unimalleolar fractures. This discrepancy is primarily due to the higher energy of the initial trauma, the extensive damage to the articular cartilage, and the inherent instability of the tibiotalar joint.
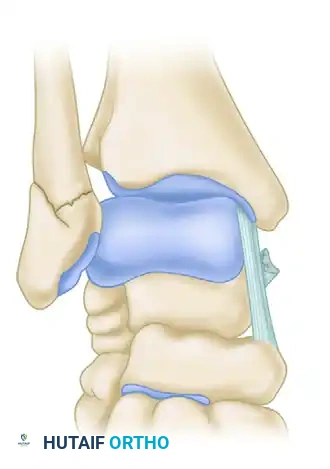
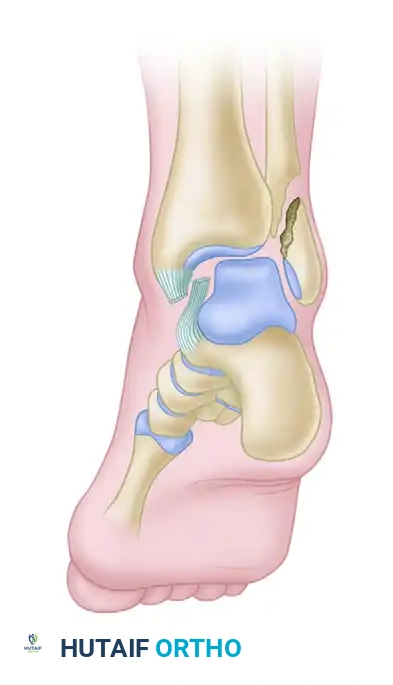
Trimalleolar fractures are typically the result of an abduction or external rotation injury mechanism, most commonly aligning with the Supination-External Rotation (SER) or Pronation-External Rotation (PER) patterns described in the Lauge-Hansen classification. In addition to the classic fractures of the medial malleolus and the fibula (lateral malleolus), the posterior lip of the articular surface of the distal tibia (the posterior malleolus) is fractured and displaced. This critical loss of posterior articular support allows for posterior and posterolateral subluxation of the talus, accompanied by external rotation and supination of the foot.
Clinical Pearl: In some variations of this injury pattern, the medial malleolus may remain radiographically intact. Instead of a bony avulsion, a complete rupture of the deltoid ligament occurs, creating a "deltoid equivalent" trimalleolar fracture. This must be recognized, as the medial instability is identical to that of a displaced medial malleolus fracture.
PATHOANATOMY AND SOFT TISSUE CONSIDERATIONS
The displacement of the ankle mortise in a trimalleolar fracture is rarely an isolated bony event; it is invariably accompanied by severe soft tissue disruption. The posterior and proximal displacement of the tibial fragment creates a significant step-off at the articular fracture line. With the foot displaced posteriorly, this irregularity in the articular surface of the tibia is brought directly against the weight-bearing dome of the talus. If left unreduced, the altered contact mechanics and point-loading will rapidly lead to severe, debilitating post-traumatic arthritis.
Soft Tissue Interposition
A critical factor that can impede closed or even open reduction is the interposition of soft tissues within the fracture site or the medial clear space. When the deltoid ligament is avulsed from its distal insertion on the medial malleolus or talus, it may become reflected proximally.
This proximal reflection creates a void that allows the posterior tibial tendon to subluxate anteriorly and laterally, becoming interposed between the medial malleolus and the talus.
Such entrapment not only blocks anatomical reduction of the talus within the mortise but also severely impairs the spontaneous healing of the deltoid ligament.
Surgical Warning: Persistent widening of the medial clear space after fibular reduction is highly suspicious for soft tissue interposition. The posterior tibial tendon or a flipped osteochondral fragment from the medial malleolus must be surgically extracted from the joint space before definitive fixation.
PREOPERATIVE EVALUATION AND IMAGING
Standard radiographic evaluation includes anteroposterior (AP), lateral, and mortise views of the ankle. A 50-degree external rotation view may be utilized for the most accurate plain-film assessment of the size and displacement of the posterior malleolar fragment.
However, plain radiography is notoriously unreliable for assessing the true articular involvement and morphology of the posterior malleolus. Therefore, preoperative CT scans are mandatory for the evaluation of trimalleolar fractures. CT imaging provides critical information regarding:
* The exact size and location of the posterior malleolar fragment(s).
* The presence of marginal impaction or comminution of the posterior articular surface.
* The trajectory of the fracture lines (e.g., posterolateral vs. posteromedial extension), which dictates the optimal surgical approach.
* The presence of intra-articular loose bodies.
INDICATIONS FOR OPERATIVE INTERVENTION
The overarching principles and indications for open reduction of bimalleolar fractures apply equally to trimalleolar fractures: restoration of fibular length, anatomical reduction of the articular surface, and stabilization of the syndesmosis.
The indications for specific open reduction and internal fixation of the posterior malleolus depend chiefly on its size, displacement, and contribution to syndesmotic stability:
- Fragment Size: Historically, if the fragment of the posterior malleolus involves more than 25% to 30% of the weight-bearing articular surface on the lateral radiograph, it should be anatomically reduced and held with internal fixation. Fragments constituting less than 25% were often deemed inconsequential if the anterior part of the tibial articular surface was large enough to provide a stable weight-bearing surface.
- Articular Step-off: Even if the fragment is small, any persistent step-off or gap of more than 2 to 3 mm after fibular reduction warrants open reduction. The slightest posterior subluxation of the talus on the articular surface of the tibia is unacceptable.
- Syndesmotic Instability: Modern biomechanical understanding emphasizes the posterior malleolus as the primary attachment site for the posterior inferior tibiofibular ligament (PITFL). Gardner et al. demonstrated in a cadaveric model that anatomical fixation of the posterior malleolus imparts syndesmotic stability to a significantly greater extent than traditional trans-syndesmotic screws. Therefore, even smaller fragments may require fixation if syndesmotic instability persists.
In fractures with posterior malleolar fragments constituting 25% or more of the joint, studies by Harper and Hardin found no clinical differences between fractures that were reduced and fixed versus those that were not, provided that the lateral malleolar fracture was anatomically reduced and fixed. Often, satisfactory indirect reduction of the posterior tibial fragment occurs with rigid fixation of the fibula, because this fragment is most often posterolateral and remains attached to the fibula via the intact PITFL (ligamentotaxis). However, direct visualization and fixation are increasingly favored to ensure absolute articular congruity.
SURGICAL APPROACHES
The approach to the posterior malleolus depends heavily on the fracture morphology identified on the preoperative CT scan and what additional open reductions are required.
1. The Posterolateral Approach
This is the workhorse approach for most trimalleolar fractures, as it allows simultaneous access to the fibula and the posterolateral aspect of the distal tibia through a single incision.
* Positioning: The patient is placed in the prone or lateral decubitus position.
* Incision: A longitudinal incision is made midway between the posterior border of the fibula and the lateral border of the Achilles tendon.
* Dissection: The lesser saphenous vein and sural nerve must be identified and protected. The deep fascia is incised, and the interval between the peroneal tendons (retracted laterally) and the flexor hallucis longus (FHL) muscle belly (retracted medially) is developed.
* Exposure: Retracting the FHL medially protects the posteromedial neurovascular bundle and exposes the posterior aspect of the distal tibia and the posterior malleolar fragment.
2. The Posteromedial Approach
If the preoperative CT indicates that the posterior fragment is located more medially, or if there is a large posteromedial extension, a posteromedial approach is utilized.
* Incision: Made adjacent to the posteromedial border of the tibia.
* Dissection: The posterior tibial tendon and flexor digitorum longus are retracted anteriorly, while the neurovascular bundle and FHL are retracted posteriorly. This provides excellent access to the posteromedial distal tibia.
3. The Anteromedial Approach
Most often, a standard anteromedial incision is made to fix a fractured medial malleolus. This is usually performed with the patient supine, requiring repositioning if a prone posterolateral approach was used first, or it can be done simultaneously if the patient is in a "floppy lateral" position.
COMPLEX VARIATIONS: THE BOSWORTH FRACTURE-DISLOCATION
A rare but severe variant of the ankle fracture-dislocation is the Bosworth fracture. This injury is characterized by a severe external rotation force that results in the proximal fibular fragment becoming entrapped behind the posterior tubercle of the distal tibia.
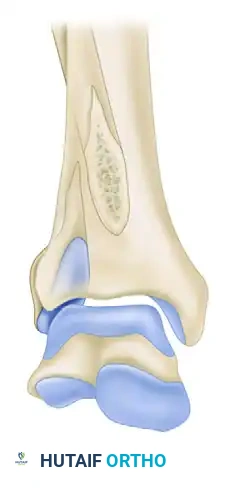
FIGURE 54-11 A: Anteroposterior view demonstrating the Bosworth fracture with entrapment of the fibula behind the tibia.
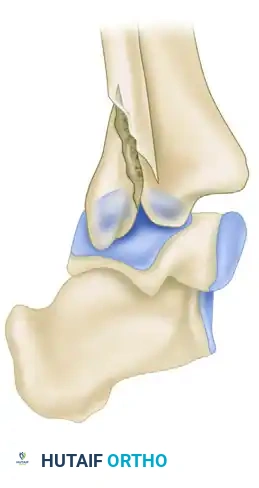
FIGURE 54-11 B: Lateral view showing severe posterior displacement and fibular entrapment.
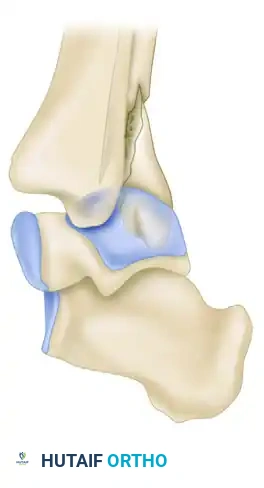
FIGURE 54-11 C: Lateral view highlighting the mechanical block to reduction.
Closed reduction of a Bosworth fracture is almost always impossible due to the mechanical block created by the entrapped fibula. Forceful attempts at closed reduction can lead to iatrogenic skin necrosis or neurovascular injury. Immediate open reduction is required. The fibula must be carefully levered out from behind the tibia using a periosteal elevator or bone hook before standard fracture sequence fixation can commence.
STEP-BY-STEP SURGICAL TECHNIQUE
Sequence of Reduction
The traditional sequence of fixation has been the lateral malleolus, followed by the medial malleolus, and finally the posterior malleolus. However, modern techniques advocate for a different approach when direct fixation of the posterior malleolus is planned.
Surgical Pearl: If internal fixation of the posterior malleolus is necessary, it should be reduced and internally fixed before the reduction of either the medial or the lateral malleolus.
The objective is to anatomically restore the articular surface of the distal tibia. Reduction and fixation of either the medial or lateral malleolus reduces the distractibility of the tibial and talar joint surfaces, making exposure and reduction of the posterior fragment significantly more difficult.
Joint Distraction Techniques
If the joint is tight, distraction of the tibiotalar joint can be increased by inserting a large Steinmann pin transversely through the calcaneus, to which a traction bow is applied. An assistant can distract the tibiotalar joint significantly using this technique, provided neither malleolus has been reattached. Alternatively, a large femoral distractor spanning from the tibial shaft to the calcaneus or talar neck may be of immense benefit for visualizing the posterior articular surface.
Techniques for Posterior Malleolar Fixation
Once the posterior fragment is reduced, provisional fixation is achieved with K-wires. The definitive fixation construct depends on the size and comminution of the fragment.
1. Anterior-to-Posterior (AP) Lag Screws:
If the posterior malleolar fragment is small or if a direct posterior approach is not utilized, a screw directed from anterior to posterior can be used.
* Pitfall: A partially threaded screw placed from anterior to posterior may leave screw threads crossing the fracture site, preventing compression. A fully threaded screw placed by lag technique (overdrilling the near cortex) is preferred.
2. Posterior-to-Anterior (PA) Lag Screws:
When utilizing a posterolateral approach, direct PA lag screw fixation is biomechanically superior.
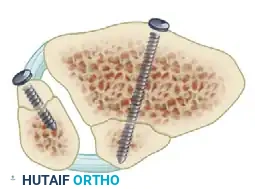
FIGURE 54-12 A: Anteroposterior view of a 4-mm lag screw utilized for posterior malleolar fixation.
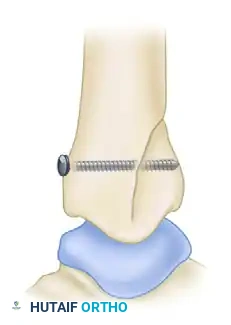
FIGURE 54-12 B: Lateral view demonstrating the trajectory of the 4-mm anteroposterior lag screw.
3. Multiple Lag Screws for Comminution:
Larger or slightly comminuted fragments may require multiple lag screws to achieve rotational stability and adequate compression across the broad fracture face.
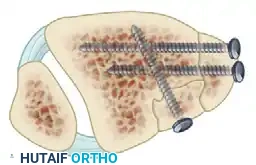
FIGURE 54-12 C: Multiple lag screw fixation of a comminuted posterior malleolar fracture.
4. Avulsion Fracture Fixation:
Small avulsion fractures, particularly at the insertion of the anterior or posterior tibiofibular ligaments, can also be addressed with targeted lag screw fixation to restore syndesmotic tension.
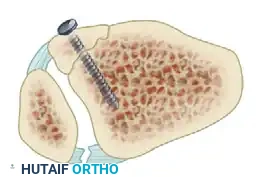
FIGURE 54-12 D: Lag screw fixation of an avulsion fracture at the insertion of the anterior tibiofibular ligament from the distal tibia.
5. Posterior Buttress Plating:
For large, vertically oriented posterior malleolar fractures, or those with metaphyseal comminution, lag screws alone may fail to resist the shear forces of the talus. In these instances, a posterior antiglide or buttress plate (e.g., a 1/3 tubular plate or pre-contoured posterior tibial plate) applied directly to the posterior cortex provides the most biomechanically robust construct.
Finalizing the Construct
Following posterior malleolar fixation, the fibula is reduced and fixed using standard AO principles (lag screw and neutralization plate, or bridging plate for comminution). Finally, the medial malleolus is addressed. The joint is thoroughly irrigated to remove any osteochondral debris. The syndesmosis is then dynamically stressed (Cotton test or external rotation stress test) under fluoroscopy. If the posterior malleolus has been rigidly fixed, the syndesmosis is often stable; however, if widening occurs, trans-syndesmotic screw or suture-button fixation is required.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of trimalleolar fractures must balance the need for early range of motion to prevent stiffness with the necessity of protecting the complex articular reconstruction.
- Phase I (0-2 Weeks): The patient is placed in a well-padded, short-leg posterior splint with the ankle in neutral dorsiflexion. Strict non-weight-bearing (NWB) status is enforced. Elevation and edema control are paramount.
- Phase II (2-6 Weeks): At the first postoperative visit, sutures are removed. If the wounds are healing well and fixation is robust, the patient is transitioned to a removable controlled ankle motion (CAM) boot. Active and active-assisted range of motion (ROM) exercises for the ankle and subtalar joints are initiated. The patient remains NWB.
- Phase III (6-12 Weeks): Radiographs are obtained at 6 weeks to assess for callus formation and maintenance of the mortise. If clinical and radiographic signs of healing are present, progressive weight-bearing is initiated, transitioning from partial to full weight-bearing in the CAM boot, and eventually to a supportive shoe.
- Phase IV (3-6 Months): Physical therapy focuses on proprioception, strengthening of the peroneal and posterior tibial musculature, and gait normalization.
COMPLICATIONS
Despite optimal surgical management, trimalleolar fractures carry a higher complication rate than simpler ankle injuries.
* Post-Traumatic Osteoarthritis: The most significant long-term complication. The risk correlates directly with the energy of the initial injury, the degree of initial talar dislocation, and the accuracy of the articular reduction.
* Stiffness: Loss of dorsiflexion is common, often due to capsular scarring or subtle anterior impingement. Early ROM protocols mitigate this risk.
* Wound Complications: Particularly high in patients with diabetes, peripheral vascular disease, or those who smoke. Meticulous soft tissue handling and delaying surgery until the "wrinkle sign" appears are critical preventative measures.
* Malunion/Nonunion: Rare with modern rigid fixation techniques, but can occur, particularly at the medial malleolus if soft tissue interposition is missed.
In conclusion, the successful management of trimalleolar fractures demands a profound understanding of ankle biomechanics, rigorous preoperative CT planning, and meticulous surgical execution. By prioritizing the anatomical restoration of the posterior malleolus and the syndesmotic complex, the orthopedic surgeon can optimize functional outcomes and delay the onset of post-traumatic arthropathy in these challenging injuries.
📚 Medical References
- Trimalleolar fractures, South Med J 58:1292, 1965.
- Watson JT: Tibial pilon fractures, Tech Orthop 11:150, 1996.
- Watson JT, Karges DE, Cramer KE, et al: Analysis of failure of hybrid external fi xation techniques for the treatment of distal tibial pilon fractures. Paper presented at the annual meeting of the Orthopaedic Trauma Association, San Antonio, Tex, Oct 14, 2000.
- Watson JT, Moed BR, Karges DE, et al: Pilon fractures: treatment protocol based on severity of soft tissue injury, Clin Orthop 375:78, 2000.
- Weber BG: Die verletzungen des oberen sprunggelenkes, 2nd ed, Bern, 1972, Verlag Hans Huber. Whitelaw GP, Sawka MW, Wetzler M, et al: Unrecognized injuries of the lateral ligaments associated with lateral malleolar fractures of the ankle, J Bone Joint Surg 71A:1396, 1989.
- Williams TM, Marsh JL, Nepola JV, et al: External fi xation of the tibial plafond fractures: is routine plating of the fi bula necessary? J Orthop Trauma 12:16, 1998.
- Williams TM, Nepola JV, DeCoster TA, et al: Factors affecting outcome in tibial plafond fractures, Clin Orthop Relat Res 423:93, 2004.
- Wilson FC: The pathogenesis and treatment of ankle fractures: classifi cation, Instr Course Lect 39:79, 1990.
- Wilson FC: The pathogenesis and treatment of ankle fractures: historical studies, Instr Course Lect 39:73, 1990.
- Wilson FC Jr, Skilbred LA: Long-term results in the treatment of displaced bimalleolar fractures, J Bone Joint Surg 48A:1065, 1966.
- Wiss DA, Gilbert P, Merritt PO, et al: Immediate internal fi xation of open ankle fractures, J Orthop Trauma 2:265, 1988.
- Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: a randomized, prospective study, J Bone Joint Surg 78A:1646, 1996.
- Yablon IG: Ankle fractures: internal fi xation, I: reduction of displaced bimalleolar ankle fractures, Instr Course Lect 28:72, 1979.
- Yablon IG, Heller FG, Shouse L: The key role of the lateral malleolus in displaced fractures of the ankle, J Bone Joint Surg 59A:169, 1977.
- Yang L, Nayagam S, Saleh M: Stiffness characteristics and interfragmentary displacements with different hybrid external fi xators, Clin Biomech 18:166, 2002.
- Yde J, Kristensen KD: Ankle fractures: supination-eversion fractures of stage II—primary and late results of operative and nonoperative treatment, Acta Orthop Scand 51:695, 1980.
- Yde J, Kristensen KD: Ankle fractures: supination-eversion fractures of stage IV—primary and late results of operative and nonoperative treatment, Acta Orthop Scand 51:981, 1980.
- Zadik FR: Primary internal fi xation of compound fractures: proceedings of the British Orthopaedic Association, J Bone Joint Surg 35B:146, 1953.
- Tibial Shaft Anderson LD, Hutchins WC: Fractures of the tibia and fi bula treated with casts and transfi xing pins, South Med J 59:1026, 1966.
- Anderson LD, Hutchins WC, Wright PE, et al: Fractures of the tibia and fi bula treated by casts and transfi xing pins, Clin Orthop Relat Res 105:179, 1974.
- Archdeacon MT, Wyrick JD: Reduction plating for provisional fracture fi xation, J Orthop Trauma 20:206, 2006.
- Austin RT: The Sarmiento tibial plaster: a prospective study of 145 fractures, Injury 13:10, 1981.
- Bach AW, Hansen ST Jr: Plates versus external fi xation in severe open
You Might Also Like

