Extensor Tendon Repair: Zone I & Mallet Finger Guide
Key Takeaway
Zone I extensor tendon injuries, commonly known as mallet fingers, result from the disruption of the terminal extensor tendon at the distal interphalangeal (DIP) joint. Management depends on whether the injury is a closed rupture, an open transection, or involves a bony avulsion. This guide details evidence-based protocols for conservative splinting, acute surgical repair techniques, and postoperative rehabilitation to optimize functional outcomes and prevent chronic deformities.
EXTENSOR TENDON REPAIR: PRINCIPLES AND ANATOMY
The extensor mechanism of the hand is a highly complex, finely balanced biomechanical system. Unlike the flexor tendons, which are robust and enclosed within a well-defined synovial sheath, the extensor tendons are broad, flat, and rely on an intricate network of retinacular ligaments, sagittal bands, and intrinsic muscle contributions to function effectively. Successful extensor tendon repair requires not only meticulous surgical technique but also a profound understanding of this delicate anatomical balance.
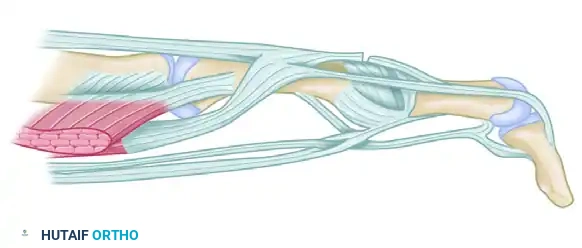
Anatomy of the Extensor Apparatus
The extensor apparatus of the fingers is formed by the confluence of the extrinsic extensor tendons (extensor digitorum communis, extensor indicis proprius, extensor digiti minimi) and the intrinsic muscles (lumbricals and interossei).
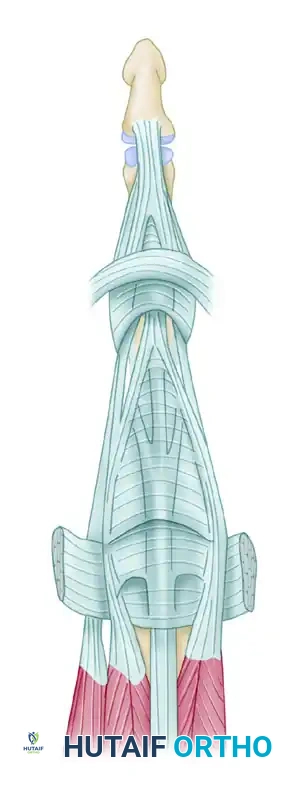
Dorsal view of the extensor apparatus anatomy.
At the level of the metacarpophalangeal (MCP) joint, the extrinsic tendon is centralized by the sagittal bands. As the tendon proceeds distally over the proximal phalanx, it divides into a central slip and two lateral bands. The central slip inserts into the dorsal base of the middle phalanx, extending the proximal interphalangeal (PIP) joint.

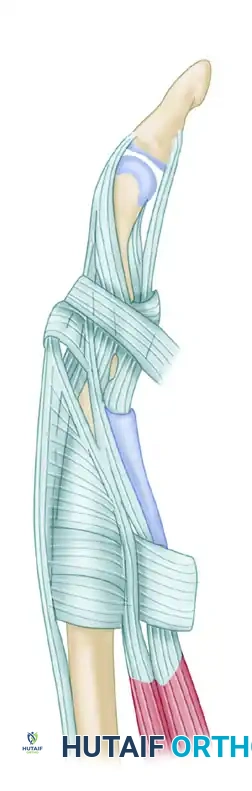
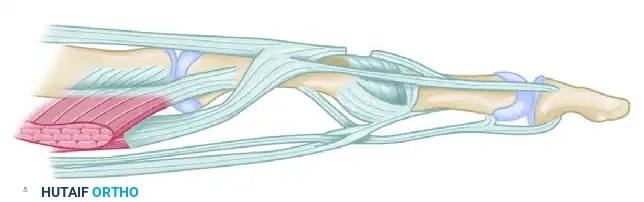
Lateral view of the extensor apparatus, highlighting the intrinsic contributions and retinacular ligaments.
The lateral bands receive contributions from the intrinsic muscles, converge dorsally over the middle phalanx, and unite to form the terminal extensor tendon, which inserts into the dorsal base of the distal phalanx to extend the distal interphalangeal (DIP) joint.
Topographical Classification: The Extensor Zones
To emphasize the different anatomical relationships of the extensor tendons and their attachments, the extensor surface of the hand and wrist has been universally divided into distinct topographical zones.
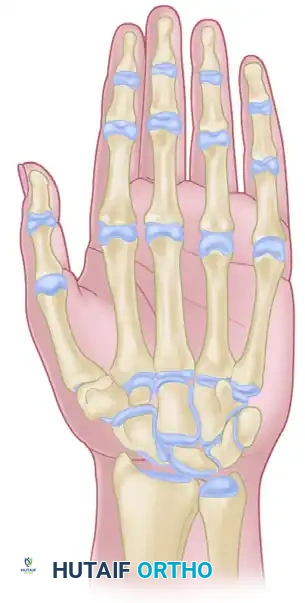
Overview of the extensor tendon zones of the hand and wrist.
The classification system follows a logical anatomical progression: even-numbered zones are located over bones (phalanges, metacarpals, radius/ulna), while odd-numbered zones are located over joints. The forearm area, containing the extensor muscle bellies, is designated as the ninth zone.
- Zone I:
 Distal interphalangeal (DIP) joint.
Distal interphalangeal (DIP) joint. - Zone II:
 Middle phalanx.
Middle phalanx. - Zone III:
 Proximal interphalangeal (PIP) joint.
Proximal interphalangeal (PIP) joint. - Zone IV:
 Proximal phalanx.
Proximal phalanx. - Zone V:
 Metacarpophalangeal (MCP) joint.
Metacarpophalangeal (MCP) joint. - Zone VI:
 Metacarpals.
Metacarpals. - Zone VII:
 Dorsal retinaculum and radiocarpal joint.
Dorsal retinaculum and radiocarpal joint. - Zone VIII: Distal forearm (musculotendinous junctions).
- Zone IX: Proximal forearm (muscle bellies).
The acute (primary) and chronic (delayed, secondary) management of extensor tendon injuries are dictated entirely by the zone of injury. This guide focuses extensively on the pathology, biomechanics, and surgical management of Zone I injuries.
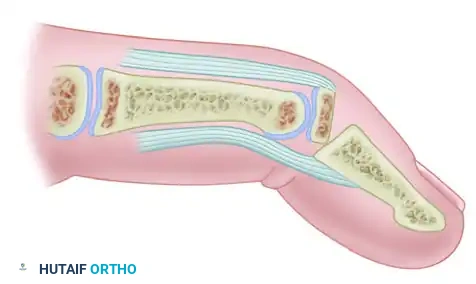
ZONE I INJURIES: THE MALLET FINGER
Zone I is located at the level of the distal interphalangeal (DIP) joint. Disruption of the terminal extensor tendon at this level results in a characteristic flexion deformity of the DIP joint, universally known as a "mallet finger."
Pathoanatomy and Clinical Presentation
Mallet finger deformities usually result from a sudden, forceful flexion of an actively extended DIP joint—commonly occurring when a ball strikes the tip of an outstretched finger. This mechanism leads to a closed avulsion of the terminal tendon insertion. The injury may be purely tendinous, or it may involve an avulsion fracture of the dorsal base of the distal phalanx.
Clinically, the patient presents with pain, swelling over the dorsal DIP joint, and an inability to actively extend the distal phalanx. If left untreated, the biomechanical imbalance can lead to a secondary swan-neck deformity. The loss of terminal tendon tension causes the extensor mechanism to retract proximally, concentrating the extensor force on the central slip at the PIP joint, leading to PIP hyperextension and DIP flexion.
Clinical Pearl: Always assess the PIP joint in a patient with a mallet finger. A supple PIP joint that passively corrects indicates an early, flexible deformity. A rigid PIP joint suggests a chronic, fixed swan-neck deformity requiring more complex reconstruction.
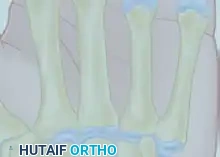
Pediatric Considerations: Physeal Injuries
In the pediatric population, a mallet finger posture is rarely caused by a pure tendon rupture. Instead, it is frequently the result of a traumatic separation of the distal phalanx epiphysis (a Salter-Harris type I or II fracture).
Displacement of the epiphysis of the distal phalanx causing a mallet finger posture in a child.
These deformities can be readily recognized with standard orthogonal radiographs. The terminal extensor tendon inserts into the epiphysis, while the deep flexor tendon inserts into the metaphysis. A forced flexion injury separates the physis, resulting in the characteristic clinical droop.
Hyperextension of the phalanx usually affords satisfactory reduction of the displaced epiphysis.
Early detection allows for straightforward closed reduction via hyperextension of the DIP joint. The finger is splinted for 3 to 4 weeks. Because this is a bony/physeal injury, healing is rapid compared with a true tendinous injury. Growth disturbance (premature physeal closure) is possible but rare.
Surgical Warning: Be highly suspicious of a Seymour fracture in pediatric mallet injuries. If there is an associated nail bed laceration or the nail plate is avulsed proximal to the eponychial fold, this is an open fracture. It requires formal irrigation, debridement, nail bed repair, and often K-wire fixation to prevent osteomyelitis and growth arrest.
MANAGEMENT OF CLOSED ZONE I INJURIES
For a closed extensor tendon rupture from its insertion into the distal phalanx, the gold standard of treatment is nonsurgical.
Splinting Protocols and Biomechanics
The objective of conservative management is to approximate the torn ends of the terminal tendon and allow them to heal via intrinsic and extrinsic fibroplasia. This is achieved by continuously holding the DIP joint in slight hyperextension.
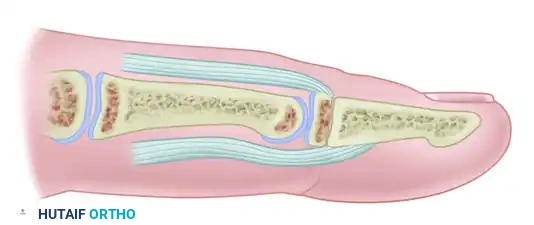
A standard Stack splint utilized for conservative management of Zone I mallet finger injuries.
The Splinting Regimen:
1. Continuous Immobilization: The DIP joint must be held in extension or slight hyperextension continuously for 6 to 8 weeks.
2. Night Splinting: Following the initial continuous phase, night splinting is recommended for an additional 1 to 2 weeks, or during high-risk sporting activities.
3. PIP Joint Freedom: The splint must only immobilize the DIP joint. The PIP joint must be left free to allow active flexion and extension. Active PIP motion pulls the lateral bands proximally, which paradoxically helps advance the terminal tendon distally toward its insertion.
Pitfall: The most common cause of conservative treatment failure is patient non-compliance. Patients must be explicitly instructed that if the splint is removed for hygiene and the DIP joint is allowed to flex even once, the healing tissue is disrupted, and the 6-to-8-week clock restarts at day zero.
Outcomes of Conservative Management:
Splint treatment initiated within 2 weeks of injury has been found to be highly effective. Remarkably, this treatment can also be successful in patients presenting up to 3 months after the initial injury. High patient satisfaction is routinely reported at an average of 5 years post-treatment, regardless of whether the injury was purely tendinous or involved a small bony avulsion.
While the last few degrees of extreme active extension may be permanently lost (a mild extensor lag of 5-10 degrees), the functional deficit is negligible. Osteoarthritic changes are seen in approximately 48% of cases at long-term follow-up, almost exclusively associated with intra-articular fracture variants rather than pure tendinous ruptures.
SURGICAL MANAGEMENT OF ACUTE OPEN TRANSECTIONS
While closed injuries are managed conservatively, an acute open transection of the extensor tendon in Zone I mandates formal surgical exploration and repair.
Indications for Surgery
- Open lacerations with transection of the terminal tendon.
- Closed mallet fingers with a large volar subluxation of the distal phalanx (indicating a massive dorsal bony avulsion >30-50% of the articular surface).
- Failure of conservative splinting (chronic cases).
Surgical Technique: Step-by-Step Open Repair
1. Preparation and Positioning:
* The patient is positioned supine with the arm on a radiolucent hand table.
* A digital block or regional anesthesia is administered.
* A digital tourniquet (or forearm tourniquet) is applied to ensure a bloodless surgical field.
2. Exposure and Mobilization:
* The traumatic skin laceration is irrigated and debrided.
* If exposure is inadequate, the laceration is extended proximally and distally using mid-axial or lazy-S incisions to avoid dorsal scar contractures.
* The proximal stump of the terminal tendon often retracts slightly but is usually tethered by the triangular ligament. It is grasped gently with fine forceps and mobilized to its insertion at the distal phalanx.
3. Tendon Repair:
* Because the terminal tendon is extremely thin and flat (often less than 1 mm thick), standard core sutures (like the modified Kessler) are impossible to place and will pull out.
* Instead, a roll stitch (figure-of-eight) or a dermotenodermal suture is utilized.
* Using a 4-0 or 5-0 non-absorbable monofilament (e.g., Prolene or Nylon), the suture incorporates the skin, the proximal tendon stump, the distal tendinous insertion (or periosteum), and exits the skin. This technique uses the dermis to bolster the fragile tendon repair.
4. Transarticular Fixation:
* To protect the tenuous repair, the DIP joint is temporarily arthrodesed.
* A 0.035-inch or 0.045-inch Kirschner wire (K-wire) is driven longitudinally or obliquely across the DIP joint, holding it in neutral to slight hyperextension.
* Surgical Tip: Ensure the K-wire does not violate the PIP joint. Confirm placement with intraoperative fluoroscopy.
5. Closure and Postoperative Protocol:
* The wound is closed with interrupted non-absorbable sutures.
* The finger is temporarily splinted for comfort and to avoid additional trauma.
* At 3 weeks: The dermotenodermal or roll sutures are removed.
* At 4 to 6 weeks: The transarticular K-wire is removed in the clinic.
* Weeks 6 to 10: The finger is protected with a mallet splint for an additional 2 to 4 weeks, particularly during activity. Progressive active motion exercises are initiated and continued until maximal function is achieved.
MANAGEMENT OF CHRONIC MALLET DEFORMITIES
Patients presenting with chronic mallet deformities (greater than 3 months old) or those who have failed conservative management present a unique reconstructive challenge. The terminal tendon is often scarred, attenuated, and incapable of primary repair.
The Fowler Tenotomy
For a chronic mallet finger with a supple DIP joint and an associated swan-neck deformity, a central slip tenotomy (Fowler procedure) can rebalance the extensor apparatus.
Tenotomy of the central slip (Fowler procedure) to correct a chronic mallet finger. This results in proximal retraction of the extensor apparatus, increasing tension on the terminal tendon.
Biomechanical Rationale:
By surgically dividing the central slip of the extensor tendon at its insertion on the middle phalanx, the entire extensor mechanism is allowed to slide proximally. This proximal migration increases the resting tension on the lateral bands and the terminal tendon. Consequently, the extensor force is redirected from the PIP joint to the DIP joint, correcting both the PIP hyperextension and the DIP flexion lag.
Technique Overview:
1. A dorsal longitudinal or curved incision is made over the PIP joint.
2. The extensor apparatus is exposed, and the central slip is identified.
3. The central slip is sharply transected just proximal to its insertion on the middle phalanx. Crucially, the lateral bands must remain completely intact.
4. The PIP joint is pinned in slight flexion, and the DIP joint is pinned in extension for 3 to 4 weeks to allow the mechanism to reset at its new tension length.
Arthrodesis
In cases of chronic mallet finger with severe secondary osteoarthritis of the DIP joint, fixed joint contractures, or failed soft-tissue reconstructions, a primary DIP joint arthrodesis is the salvage procedure of choice. The joint is fused in neutral to 5 degrees of flexion, providing a stable, pain-free, and cosmetically acceptable digit.
POSTOPERATIVE REHABILITATION AND OUTCOMES
Whether managed conservatively or surgically, the rehabilitation phase is critical to the success of Zone I extensor tendon repairs.
- Phase I (Immobilization: Weeks 0-6): Strict adherence to DIP extension. Unrestricted active range of motion of the MCP and PIP joints is encouraged to prevent stiffness and promote tendon gliding.
- Phase II (Weaning: Weeks 6-8): Splint wear is reduced to nighttime and high-risk activities. Gentle active flexion of the DIP joint is initiated. Passive flexion is strictly avoided to prevent stretching the fragile repair.
- Phase III (Strengthening: Weeks 8-12): Progressive resistance exercises are introduced. If an extensor lag begins to recur during this phase, the patient must immediately revert to continuous splinting for an additional 2 to 3 weeks.
Complications:
Complications in Zone I repairs include dorsal skin necrosis (due to overly tight splinting or surgical tension), transient nail deformities, pin-tract infections from K-wires, and residual extensor lags. A residual lag of up to 10 degrees is common, functionally insignificant, and should be discussed with the patient preoperatively to manage expectations. Strict adherence to biomechanical principles and meticulous tissue handling remain the cornerstones of successful extensor tendon surgery.
You Might Also Like
