Eponychial Marsupialization and Advanced Surgical Management of Paronychia
Key Takeaway
Eponychial marsupialization is a highly effective surgical intervention for recalcitrant chronic paronychia. By excising a crescentic wedge of proximal eponychial skin, the technique facilitates drainage, eradicates fibrotic tissue, and restores the physiological barrier of the nail fold. When combined with targeted antibiotic therapy and meticulous postoperative care, this procedure yields excellent clinical outcomes with minimal recurrence rates.
Comprehensive Introduction and Patho-Epidemiology
Infections of the fingertip and the perionychium represent a substantial proportion of the acute and chronic pathologies encountered in daily hand surgery practice. While acute paronychia is characteristically a straightforward, purulent bacterial infection highly amenable to simple incision, drainage, and targeted antimicrobial therapy, chronic paronychia presents a far more insidious and complex therapeutic challenge. Chronic paronychia is not merely a prolonged acute infection; rather, it is a multifactorial inflammatory dermatosis characterized by persistent induration, progressive fibrosis, and the catastrophic loss of the protective cuticular barrier. This condition is often driven by a synergistic combination of relentless mechanical irritation, environmental moisture exposure, fungal colonization (predominantly Candida albicans), and a shifting milieu of mixed bacterial flora.
The epidemiological profile of chronic paronychia is heavily skewed toward specific occupational and environmental demographics. Individuals subjected to constant moisture, chemical irritants, or repetitive microtrauma—such as dishwashers, bartenders, healthcare workers, florists, and housekeepers—are at exponentially higher risk. The chronic exposure to water and detergents leads to the maceration of the stratum corneum and the subsequent dissolution of the eponychial seal. Once this vital waterproof barrier is breached, a microscopic dead space is created between the proximal nail fold and the dorsal nail plate. This recess becomes a sanctuary for opportunistic pathogens, allowing debris, moisture, and microbes to accumulate, thereby initiating a vicious cycle of chronic inflammation, reactive hyperkeratosis, and progressive tissue fibrosis.
Microbiologically, the pathogenesis of chronic paronychia is distinct from its acute counterpart. While acute infections are overwhelmingly dominated by Staphylococcus aureus or Streptococcus pyogenes, chronic paronychia is classically associated with Candida species. However, contemporary microbiological analyses reveal that the condition is frequently polymicrobial. Fungal colonization often acts as the primary inflammatory catalyst, but secondary bacterial colonization with Staphylococcus, Pseudomonas aeruginosa, and various anaerobic species frequently supervenes, exacerbating the inflammatory cascade. The presence of a polymicrobial biofilm within the sub-eponychial recess further complicates conservative management, rendering topical and systemic antimicrobial therapies largely ineffective once structural tissue changes have occurred.
When rigorous conservative measures—encompassing strict avoidance of moisture, application of high-potency topical corticosteroids, judicious use of antifungal agents, and behavioral modification—fail to arrest the disease process after six to eight weeks, surgical intervention becomes an absolute mandate. The surgical philosophy hinges on the eradication of the fibrotic dead space, the excision of colonized, non-viable tissue, and the restoration of a healthy perionychial microenvironment. Eponychial marsupialization, originally championed by Keyser and Eaton and subsequently refined by Bednar and Lane, remains the unequivocal gold standard for recalcitrant cases. Concurrently, the advent of tissue-sparing modalities, such as the "Swiss roll" technique elucidated by Pabari et al., has significantly expanded the surgical armamentarium, offering innovative solutions that minimize iatrogenic morbidity while maximizing functional and aesthetic recovery.
Detailed Surgical Anatomy and Biomechanics
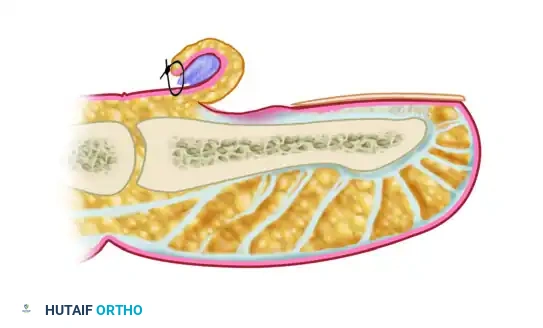
A profound, three-dimensional understanding of fingertip and perionychial anatomy is the fundamental prerequisite for executing perionychial surgery. The perionychium is a highly specialized anatomical complex comprising the nail bed and the surrounding soft tissue envelope (the paronychium). The nail bed itself is functionally and histologically delineated into two distinct zones: the proximal germinal matrix and the distal sterile matrix. The germinal matrix, extending proximally beneath the eponychial fold, is the primary engine of nail generation, responsible for synthesizing approximately 90% of the nail plate's volume. The sterile matrix, extending distally from the lunula to the hyponychium, contributes to the adherence and the deep cellular layers of the nail plate, ensuring its structural integrity and tight apposition to the underlying distal phalanx.
The eponychium constitutes the proximal nail fold, and its most distal, specialized extension forms the cuticle. The cuticle is a critical anatomical structure; it functions as a highly effective, waterproof gasket that hermetically seals the potential space between the dorsal skin and the keratinized nail plate. In the pathomechanics of chronic paronychia, the destruction of this cuticular seal is the primary inciting event. The resulting dead space allows the ingress of exogenous irritants and pathogens beneath the eponychial fold, leading to chronic induration, profound fibrosis, and marked hypertrophy of the proximal nail fold. This hypertrophic tissue acts as a mechanical barrier, preventing the re-establishment of a normal cuticular seal even if the underlying infection is temporarily suppressed by medical therapy.
The vascular and neural anatomy of the perionychium is equally intricate and demands meticulous surgical respect. The arterial supply is derived from the terminal branches of the proper palmar digital arteries, which arborize to form robust proximal and distal subungual arcades. These arcades provide a rich, redundant blood supply that facilitates rapid tissue healing but also necessitates meticulous hemostasis during surgical dissection to maintain a clear operative field. Innervation is supplied by the terminal branches of the proper digital nerves, which provide dense sensory coverage to the perionychium. This high density of nociceptors explains the exquisite, often debilitating pain associated with acute perionychial infections and necessitates profound regional anesthesia prior to any surgical manipulation.
Deep to the perionychium lies the structurally unique digital pulp. The volar aspect of the distal phalanx is engineered to withstand immense compressive and shear forces during pinch and grasp. The subcutaneous tissue of the distal pulp is meticulously partitioned into multiple, tiny, semi-rigid compartments by strong fibrous septa. These septa traverse vertically from the volar dermis to the periosteum of the distal phalanx. A transverse fibrous curtain is also present at the level of the distal flexor finger crease, effectively isolating the distal pulp space from the more proximal digital compartments and the flexor tendon sheath. Because of these unyielding fibrous septa, any inflammatory swelling or purulence within the pulp space precipitates an immediate, exponential rise in compartmental pressure. This localized compartment syndrome results in the severe, throbbing pain pathognomonic of a felon, and if left surgically unaddressed, leads to rapid microvascular compromise, pressure necrosis, and potential osteomyelitis of the distal phalanx.
Exhaustive Indications and Contraindications
The decision to transition from conservative medical management to surgical intervention in the treatment of chronic paronychia and associated perionychial infections must be guided by strict clinical criteria. Surgery is not a first-line therapy for chronic paronychia; it is reserved for cases that have proven definitively refractory to a comprehensive, prolonged trial of non-operative modalities. The primary indication for eponychial marsupialization is chronic paronychia that has persisted despite six to eight weeks of rigorous conservative management, including the use of topical steroids, antifungals, and strict environmental modifications. Patients presenting with a markedly hypertrophic, indurated eponychial fold that experiences recurrent acute, purulent exacerbations are prime candidates for surgical excision of the diseased bursa.
Furthermore, the status of the nail plate is a critical determinant in the surgical decision-making process. The presence of severe nail plate irregularities, such as profound transverse ridging (Beau's lines), discoloration, structural dystrophy, or clinical evidence of subungual debris, indicates that the chronic inflammatory process has deeply penetrated and disrupted the function of the germinal matrix. In these instances, surgical intervention, explicitly coupled with partial or total nail plate avulsion, is indicated to remove the colonized keratinous substrate and allow the germinal matrix to regenerate a healthy, uninfected nail plate. The failure to address a dystrophic nail plate during marsupialization is a primary driver of postoperative recurrence.
Conversely, absolute and relative contraindications must be meticulously evaluated to prevent catastrophic postoperative complications. The most significant absolute contraindication to elective perionychial surgery is the presence of profound digital ischemia. Patients with severe peripheral vascular disease, advanced scleroderma, Raynaud's phenomenon with active digital ulceration, or other microvascular insufficiencies are at an unacceptably high risk of postoperative tissue necrosis, non-healing wounds, and subsequent digital amputation. In these patients, the surgical trauma of marsupialization can tip a tenuous vascular supply into overt gangrene.
Relative contraindications include uncontrolled systemic comorbidities, such as poorly managed diabetes mellitus, which severely impairs wound healing and increases the risk of postoperative deep space infections. Additionally, the presence of an acute, fulminant, ascending cellulitis or active lymphangitis necessitates the delay of elective marsupialization until the acute systemic infection has been aggressively managed with intravenous antibiotics and, if necessary, simple preliminary drainage. Finally, patient non-compliance is a profound relative contraindication. The success of eponychial marsupialization is heavily dependent on a rigorous, demanding postoperative soaking and wound care regimen; patients unwilling or unable to adhere to this protocol will almost certainly experience a recurrence of their chronic paronychia.
| Clinical Parameter | Indications for Surgical Intervention | Contraindications to Surgical Intervention |
|---|---|---|
| Duration of Symptoms | Refractory to >6-8 weeks of conservative care | Acute, isolated infection (<2 weeks) responding to medical therapy |
| Tissue Morphology | Hypertrophic, indurated, fibrotic eponychial fold | Normal eponychial contour without significant fibrosis |
| Nail Plate Status | Severe dystrophy, ridging, subungual debris | Healthy, firmly adherent, non-dystrophic nail plate |
| Vascular Status | Normal capillary refill, palpable/dopplerable digital pulses | Severe peripheral vascular disease, active digital ischemia, scleroderma |
| Systemic Health | Optimized comorbidities, immunocompetent | Uncontrolled diabetes, severe immunosuppression, active ascending lymphangitis |
| Patient Compliance | Willing and able to perform rigorous daily post-op soaks | Inability or refusal to adhere to strict postoperative wound care protocols |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential to ensure a safe, effective, and complication-free surgical outcome. The initial phase of planning involves a meticulous clinical evaluation to definitively confirm the diagnosis of chronic paronychia and to rule out more sinister or atypical pathologies that may mimic perionychial infection. The surgeon must maintain a high index of suspicion for neoplastic processes, particularly squamous cell carcinoma and amelanotic melanoma, which can present as chronic, non-healing perionychial erythema and induration. If the lesion exhibits atypical features, ulceration, or fails to respond to standard surgical management, an intraoperative tissue biopsy is mandatory. Additionally, plain film radiography (anteroposterior, lateral, and oblique views of the affected digit) must be obtained routinely to evaluate for underlying osteomyelitis of the distal phalanx, osteoarthritic spurring of the distal interphalangeal joint, or the presence of a subungual exostosis, any of which would necessitate a radical alteration in the surgical approach.
Anesthesia management is a critical component of the preoperative setup. Given the dense sensory innervation of the perionychium, profound regional anesthesia is required. A standard digital block is typically administered using a 50/50 mixture of 1% lidocaine (for rapid onset) and 0.5% bupivacaine (for prolonged postoperative analgesia). The block can be performed via a traditional dorsal web-space approach or a volar subcutaneous approach at the level of the proximal phalanx flexor crease. The use of epinephrine in digital blocks remains a topic of historical controversy; however, contemporary hand surgery literature supports the safety of low-dose epinephrine (1:100,000 or 1:200,000) in healthy digits to assist with hemostasis and prolong the duration of the block. Epinephrine should, however, be strictly avoided in patients with known vasospastic disorders or severe peripheral vascular disease.
Achieving a bloodless surgical field is paramount for the safe execution of perionychial surgery, particularly to allow for the precise identification and protection of the germinal matrix. Following exsanguination of the digit by elevation, a sterile digital tourniquet is applied to the base of the finger. This can be achieved using a commercial sterile silicone ring tourniquet (e.g., T-Ring), a tightly wrapped Penrose drain secured with a hemostat, or the rolled finger of a sterile surgical glove. The surgeon must meticulously document the tourniquet inflation time, ensuring it does not exceed the safe ischemic threshold of the digit, which is generally considered to be 20 to 30 minutes for a digital tourniquet, though the procedure rarely requires this duration.
Patient positioning and the optimization of the surgical environment are the final steps in preoperative preparation. The patient is positioned supine on the operating table with the affected upper extremity extended on a radiolucent hand table. The hand and forearm are widely prepped with a standard surgical antiseptic solution, typically chlorhexidine gluconate or povidone-iodine, and draped in a standard sterile fashion, isolating the operative field. Crucially, the surgeon must utilize loupe magnification (minimum 2.5x to 3.5x) and focused, high-intensity coaxial illumination (a surgical headlight). The anatomical tolerances within the proximal nail fold are measured in millimeters, and the failure to use adequate magnification significantly increases the risk of iatrogenic transection of the germinal matrix, leading to catastrophic, irreversible nail dystrophy.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of recalcitrant perionychial infections demands meticulous technique, profound anatomical respect, and the precise execution of the chosen operative modality. The two primary techniques utilized by orthopedic hand surgeons are the traditional eponychial marsupialization and the tissue-sparing "Swiss roll" technique.
Eponychial Marsupialization
The fundamental principle of eponychial marsupialization is the radical excision of the diseased, fibrotic tissue of the proximal nail fold. This decompresses the infected sub-eponychial space, promotes aerobic conditions hostile to anaerobic and fungal pathogens, and allows the wound to heal by secondary intention, thereby regenerating a healthy, tight cuticular seal.
Step 1: Incision and Excision
Following the establishment of profound anesthesia and a bloodless field, the surgeon utilizes a #15 or #11 scalpel blade to carefully map out a crescent-shaped wedge of skin over the proximal nail fold. The excision should be approximately 3 to 4 mm wide at its central apex, running perfectly parallel to the curve of the eponychium. The incision must extend laterally from the radial border of the nail fold to the ulnar border, ensuring the entire diseased bursa is encompassed within the excision.

Step 2: Depth of Dissection and Matrix Protection
The depth of the excision represents a critical point of technical divergence in the surgical literature. The classic technique described by Keyser and Eaton advocates for the aggressive, full-thickness removal of all thickened, fibrotic tissue from the epidermis down to the level of the proximal nail plate. This ensures the complete eradication of the diseased bursa but carries a higher risk of matrix injury. Conversely, the Bednar and Lane modification recommends a more conservative approach, excising the diseased skin but deliberately leaving the underlying subcutaneous fat intact. Bednar and Lane demonstrated that this modification is equally effective in curing chronic paronychia while significantly reducing the risk of iatrogenic injury to the underlying germinal matrix. Regardless of the chosen depth, the surgeon must exercise extreme caution; any inadvertent penetration into the germinal matrix, which lies immediately deep to the proximal nail fold, will result in permanent, irreversible nail dystrophy.
Step 3: Management of the Nail Plate
A critical evaluation of the nail plate is mandatory. If significant nail irregularities, profound ridging, discoloration, or subungual purulent debris are present, the nail plate must be removed. Bednar and Lane definitively noted that in the presence of nail dystrophy, removing the nail leads to optimal healing without recurrence, as it eliminates the colonized keratinous substrate and allows the matrix to regenerate a new, healthy plate. A Freer elevator is gently introduced beneath the nail plate to separate it from the sterile and germinal matrices, and the plate is carefully avulsed using a straight hemostat, applying steady, atraumatic traction.
Step 4: Dressing and Marsupialization
The crescentic surgical wound is intentionally left open; it is not closed primarily. Instead, it is allowed to heal by secondary intention (marsupialization). The excised defect is covered with a non-adherent, antimicrobial dressing, such as petroleum/bismuth tribromophenate–impregnated gauze (Xeroform). Crucial Step: If the nail plate was removed, a thin strip of this Xeroform gauze must be meticulously tucked beneath the proximal nail fold, resting directly on the germinal matrix. This prevents the formation of synechiae (fibrous adhesions) between the raw eponychial undersurface and the germinal matrix during the early phases of wound healing.
The "Swiss Roll" Technique
Described by Pabari, Iyer, and Khoo, the "Swiss roll" technique offers an innovative, tissue-sparing alternative for the treatment of both acute and chronic paronychia, avoiding the morbidity of tissue excision and total nail avulsion.
Step 1: Exposure and Irrigation
Following digital block and tourniquet application, the eponychial fold is carefully elevated off the underlying nail plate using a periosteal elevator or a flat McDonald dissector. This blunt dissection exposes the inflamed germinal matrix and the infected sub-eponychial space without excising any overlying tissue. The exposed area is then thoroughly irrigated with copious amounts of sterile saline to mechanically remove purulence, fungal debris, and biofilm.

Step 2: The "Swiss Roll" Retraction
A small, tightly wound roll of nonadherent dressing (such as Mepitel or a tightly rolled piece of Xeroform gauze) is prepared on the back table. The elevated proximal nail fold is then reflected proximally over this nonadherent dressing roll. This action effectively rolls the skin back upon itself, much like a "Swiss roll" pastry, widely opening the sub-eponychial space.
Step 3: Securing the Fold
The rolled eponychial fold is then secured to the dorsal skin of the distal phalanx using a nonabsorbable monofilament suture (e.g., 4-0 or 5-0 Prolene). The suture passes through the proximal dorsal skin, over the rolled fold, and anchors it in a continuously retracted position. This technique keeps the sub-eponychial space widely open for continuous drainage and aeration without excising any native tissue, preserving the eventual contour of the finger.
Surgical Drainage of a Concurrent Felon
Because chronic paronychia can occasionally be complicated by, or misdiagnosed as, a deep space infection of the distal pulp, the surgeon must be adept at managing a felon. Treatment consists of prompt surgical incision and drainage. A high lateral (mid-axial) incision is generally preferred, placed dorsal to the tactile volar pad to prevent painful scarring. The incision is deepened, and a hemostat is bluntly spread through the vertical fibrous septa across the entire pulp space to ensure complete decompression. Extreme care must be taken not to violate the transverse fibrous curtain at the distal flexor crease to avoid iatrogenic purulent flexor tenosynovitis. The wound is loosely packed with a small wick to maintain patency and allowed to heal by secondary intention.
Complications, Incidence Rates, and Salvage Management
While eponychial marsupialization and advanced tissue-sparing techniques generally yield excellent outcomes with high rates of patient satisfaction, the perionychium is an unforgiving anatomical region. Complications, when they occur, can be functionally debilitating and aesthetically devastating. The surgeon must be acutely aware of potential pitfalls, their incidence rates, and the appropriate salvage strategies.
The most feared and devastating complication of perionychial surgery is iatrogenic nail dystrophy. This occurs secondary to inadvertent surgical trauma to the germinal matrix during the excision of the eponychial fold or during overly aggressive debridement of the sub-eponychial space. The incidence of clinically significant nail dystrophy following marsupialization is reported to be between 2% and 5%, heavily dependent on the surgeon's experience and the use of adequate loupe magnification. Dystrophy can manifest as severe longitudinal splitting, complete cessation of nail growth, or the formation of a pterygium (a V-shaped extension of the eponychium attaching to the nail bed). Unfortunately, once the germinal matrix is structurally destroyed, the dystrophy is largely irreversible. Salvage management is exceptionally challenging; while split-thickness sterile matrix grafts can address sterile matrix defects, they cannot regenerate a destroyed germinal matrix. In cases of severe, painful, or cosmetically unacceptable dystrophy, the ultimate salvage procedure is complete surgical ablation of the remaining nail matrix and the application of a full-thickness skin graft or healing by secondary intention, leaving the patient permanently anonychia.
Recurrence of chronic paronychia is the most common complication, with incidence rates ranging from 10% to 20% in long-term follow-up studies. Recurrence is almost universally secondary to one of three factors: inadequate surgical excision of the fibrotic bursa, failure to remove a colonized or dystrophic nail plate at the time of index surgery, or poor patient compliance with the rigorous postoperative soaking regimen. If the fibrotic dead space is not completely eradicated, or if the wound is allowed to close prematurely, the anaerobic, moisture-rich environment is immediately recreated, leading to a rapid relapse of the infection. Salvage management for recurrence involves a thorough re-evaluation of the patient's compliance, followed by a revision marsupialization. During the revision surgery, the surgeon must be more aggressive in excising the recurrent fibrotic tissue and must ensure total avulsion of the nail plate if it was previously retained.
Deep space infections, specifically osteomyelitis of the distal phalanx or purulent flexor tenosynovitis, are rare but catastrophic complications, with an incidence of less than 1%. These typically occur if a concurrent deep space infection (such as a felon) was missed during the initial preoperative evaluation or was inadequately decompressed during surgery, allowing the virulent infection to penetrate the periosteum or track proximally through the flexor tendon sheath. Salvage management for osteomyelitis requires aggressive surgical debridement of the infected bone, which may necessitate a partial or complete terminal amputation of the distal phalanx, coupled with a prolonged course (4 to 6 weeks) of culture-directed intravenous antibiotics.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Nail Dystrophy | 2% - 5% | Iatrogenic injury to germinal matrix during excision | Matrix grafting (rarely successful); complete matrix ablation and skin grafting |
| Recurrence of Paronychia | 10% - 20% | Inadequate excision, retained dystrophic nail, non-compliance | Revision marsupialization, total nail avulsion, strict enforcement of soaking protocol |
| Synechiae Formation | 5% - 10% | Failure to pack the sub-eponychial fold postoperatively | Surgical lysis of adhesions, repacking with non-adherent gauze |
| Osteomyelitis of Distal Phalanx | < 1% | Missed concurrent felon, deep extension of infection | Aggressive bone debridement, potential terminal amputation, prolonged IV antibiotics |
| Flexor Tenosynovitis | < 1% | Iatrogenic violation of the distal flexor crease | Emergent operative washout of the flexor tendon sheath, IV antibiotics |
Phased Post-Operative Rehabilitation Protocols
Meticulous, patient-driven postoperative care is arguably as critical as the technical execution of the surgery in preventing the recurrence of chronic paronychia and ensuring optimal tissue regeneration. The rehabilitation protocol must be phased, structured, and communicated to the patient with absolute clarity, as compliance is the primary determinant of long-term success.
The immediate postoperative phase encompasses days 0 through 3. Following the surgical procedure, a bulky, non-compressive soft dressing is applied to the digit to absorb initial serosanguinous exudate and provide mechanical protection. The patient is instructed to keep the hand strictly elevated above the level of the heart to minimize dependent edema and throbbing pain. Adequate oral analgesia is prescribed, typically a short course of NSAIDs combined with acetaminophen, or a mild opioid for breakthrough pain. Empiric antimicrobial therapy is initiated immediately postoperatively. An oral antibiotic targeting Staphylococcus aureus and common skin flora, such as a first-generation cephalosporin (cephalexin) or a macrolide (erythromycin) for penicillin-allergic patients, is standard. Intraoperative swabs must always be sent for aerobic, anaerobic, and fungal cultures.
The intermediate phase, beginning on postoperative day 3, marks the initiation of the critical wound care regimen. The patient is instructed to remove the bulky surgical dressings down to the Xeroform layer. From this point forward, the patient must adhere to a rigorous, non-negotiable soaking protocol. The affected finger is soaked in a warm, dilute solution of hydrogen peroxide and water (or sterile saline) for 15 minutes, followed by gentle but thorough washing with a chlorhexidine gluconate skin cleanser (Hibiclens). This process must be repeated three to four times daily. The mechanical action of the washing is essential to debride accumulating eschar, prevent the premature closure of the marsupialized wound edges, and ensure the wound heals properly from the base upward by secondary intention. Following each soak, a fresh, light, non-adherent dressing is applied.
Antibiotic stewardship during this intermediate phase is dictated by the intraoperative culture results. If the cultures
