Thenar Space Abscesses: Surgical Anatomy, Drainage & Management
Key Takeaway
A thenar space abscess is a critical deep hand infection. Prompt surgical drainage, informed by precise anatomy and protection of vital neurovascular structures like the recurrent median nerve, is crucial. This intervention prevents severe sequelae such as permanent stiffness, nerve damage, and systemic sepsis.
Introduction and Epidemiology
Infections of the deep fascial spaces of the hand, while less common than superficial infections, represent critical surgical emergencies requiring prompt diagnosis and intervention to prevent debilitating sequelae. The lateral, or thenar, space is one such critical anatomical region prone to abscess formation. Infections in this space can arise from various etiologies, including direct penetrating trauma, spread from contiguous infections such as paronychia or felons, or through tenosynovitis of the flexor pollicis longus tendon sheath, particularly if the distal extent of Parona's space communicates with the thenar space.
The incidence of specific deep space infections like thenar space abscesses is not extensively reported in isolation but is encompassed within the broader category of severe hand infections. A delay in diagnosis or inadequate treatment can lead to significant morbidity, including widespread fascial necrosis, septic arthritis, osteomyelitis, permanent digital stiffness, contractures, nerve damage, and in severe cases, systemic sepsis. The unique anatomical constraints and vital neurovascular structures within the thenar region necessitate a thorough understanding of its surgical anatomy for effective and safe drainage. Early and accurate surgical drainage, coupled with appropriate antibiotic therapy, remains the cornerstone of management.
The microbial profile of deep space hand infections has evolved over the past two decades. While Staphylococcus aureus and Streptococcus pyogenes remain the most frequently isolated organisms, the prevalence of Methicillin-resistant Staphylococcus aureus (MRSA) has necessitated a shift in empiric antibiotic regimens. In cases involving animal bites, Pasteurella multocida must be considered, whereas human bites frequently yield polymicrobial cultures including Eikenella corrodens and various anaerobes. Immunocompromised patients, particularly those with poorly controlled diabetes mellitus or end-stage renal disease, present a higher risk for atypical mycobacterial or fungal pathogens, requiring a high index of suspicion and meticulous intraoperative tissue sampling.
Surgical Anatomy and Biomechanics
A precise understanding of the surgical anatomy of the thenar space is paramount for effective and safe drainage. The thenar space is one of the three major deep fascial spaces of the hand (along with the midpalmar space and Parona's space). Its boundaries are well-defined.
The radial border is formed by the thenar septum, a fibrous partition extending from the palmar aponeurosis to the palmar surface of the third metacarpal. The ulnar border is defined by the midpalmar septum, which originates from the palmar aponeurosis and inserts onto the palmar surfaces of the fourth and fifth metacarpals, separating the thenar space from the midpalmar space. The dorsal floor is composed of the adductor pollicis muscle, the first dorsal interosseous muscle, and the metacarpal bones. The volar roof consists primarily of the flexor pollicis longus tendon sheath and the intrinsic thenar muscles (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis). The deep surface of these thenar muscles contributes to the volar boundary. The proximal border is the distal aspect of the flexor retinaculum and the carpal tunnel, while the distal border comprises the first web space and the base of the thumb.
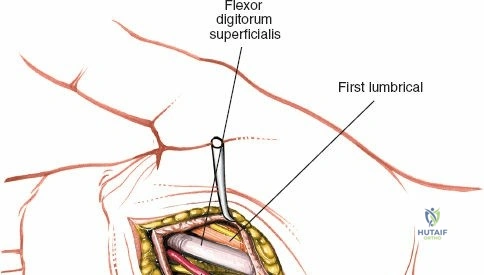
The lateral space typically contains the flexor pollicis longus tendon and its associated synovial sheath, the first metacarpal, and the adductor pollicis muscle. Infections within this space are often characterized by significant swelling of the thenar eminence, severe pain with thumb movement, and palpable tenderness. The relationship of the thenar space to other structures is crucial. Infections can spread to or from the flexor pollicis longus tendon sheath. Communication with the first web space distally is common, and rarely, infections can track proximally to Parona's space.
Critical Neurovascular Structures
Several critical neurovascular structures traverse or lie adjacent to the operative field during thenar space drainage, requiring meticulous dissection.
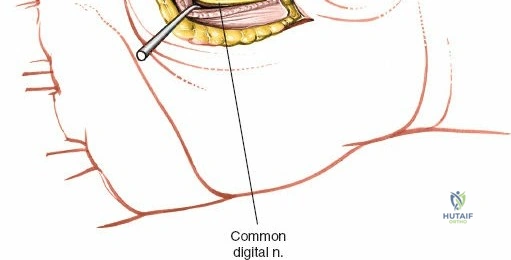
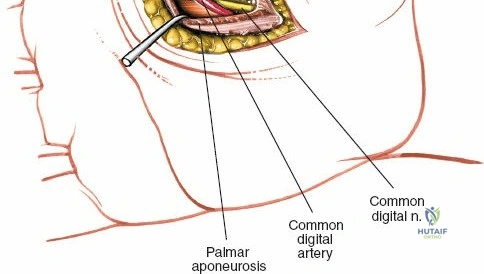
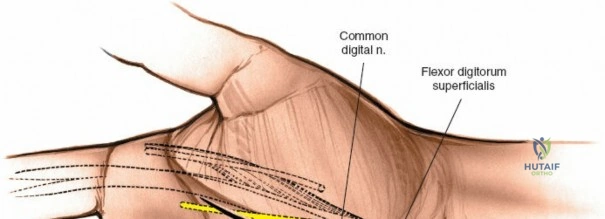
First, the digital nerves to the index finger, including the common palmar digital nerve to the radial side of the index finger and the proper palmar digital nerve to the ulnar side of the index finger, are located superficially within the subcutaneous tissue along the ulnar side of the thenar crease. These nerves are directly in line with the initial skin incision and must be identified and preserved to avoid permanent sensory deficits.
Second, the recurrent motor branch of the median nerve is of paramount importance. Often termed the "million-dollar nerve" due to the medicolegal and functional consequences of its transection, it typically branches from the radial aspect of the median nerve just distal to the transverse carpal ligament. It curves radially and proximally to innervate the thenar musculature. Surgeons must be acutely aware of its anatomical variations, which include extraligamentous, subligamentous, and transligamentous courses. An incision placed too far radially or proximally within the thenar crease places this structure at immediate risk.
Third, the superficial palmar arch and its contributing vessels lie in close proximity to the ulnar border of the thenar space. Furthermore, the princeps pollicis artery and the radialis indicis artery, branches of the deep palmar arch, course deep to the adductor pollicis muscle. While deeper and less likely to be injured during superficial dissection, aggressive blind probing or deep sharp dissection can result in significant hemorrhage from these vessels.
Biomechanical Considerations
Biomechanically, the thenar space is a potential space that expands significantly under the pressure of purulent accumulation. The adductor pollicis muscle acts as an unyielding dorsal floor. As pus accumulates, it forces the thumb into a characteristic resting posture of abduction and flexion. This position maximizes the volume of the thenar space and minimizes tension on the inflamed fascial boundaries, providing the patient with marginal pain relief. Passive adduction or extension of the thumb dramatically increases pressure within the space, eliciting severe pain—a hallmark clinical sign of a thenar space abscess.
Indications and Contraindications
The diagnosis of a thenar space abscess is primarily clinical, supported by appropriate imaging and laboratory studies. Surgical drainage is the definitive treatment and should be performed emergently upon diagnosis to prevent ischemic necrosis of the intrinsic musculature and proximal spread of the infection.
| Indication Category | Specific Clinical Scenarios |
|---|---|
| Operative Indications | Clinically evident thenar space abscess (fluctuance, ballooning of thenar eminence). |
| Severe pain with passive adduction or extension of the thumb. | |
| Failure of early cellulitis to improve after 24-48 hours of intravenous antibiotics. | |
| Concomitant flexor pollicis longus purulent tenosynovitis. | |
| Evidence of gas in the soft tissues on radiographs. | |
| Systemic signs of sepsis secondary to hand infection. | |
| Non Operative Indications | Early, superficial cellulitis without evidence of deep space fluid collection. |
| Patient medically unfit for any surgical intervention (requires aggressive medical management and aspiration). | |
| Contraindications | Lack of appropriate surgical facilities or anesthesia support (transfer required). |
| Blind percutaneous aspiration in the absence of ultrasound guidance (relative contraindication due to neurovascular risk). |
Non-operative management is strictly reserved for the earliest stages of infection where only cellulitis is present, and no discrete fluid collection has formed. Once an abscess is established, antibiotics alone are insufficient due to poor penetration into the avascular purulent cavity and the escalating compartment pressures.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning ensures a safe and efficient surgical procedure. While the diagnosis is clinical, adjunctive studies are highly beneficial for surgical mapping and ruling out complications.
Diagnostic Imaging and Laboratory Studies
Standard posteroanterior, lateral, and oblique radiographs of the hand should be obtained to rule out retained radiopaque foreign bodies, underlying fractures, or established osteomyelitis, which would alter the surgical plan. Evidence of soft tissue gas suggests infection with gas-producing organisms or anaerobes, mandating aggressive debridement.
Point-of-care ultrasound is highly sensitive for identifying fluid collections within the deep fascial spaces and differentiating an abscess from severe cellulitis. It can also map the proximity of the abscess to the flexor pollicis longus tendon sheath. Magnetic Resonance Imaging (MRI) is rarely indicated in the acute setting due to time constraints, but it may be useful in subacute or chronic cases to delineate complex fistulous tracts or subtle osteomyelitis.
Laboratory evaluation should include a complete blood count with differential, C-reactive protein, and erythrocyte sedimentation rate. In patients exhibiting systemic signs of toxicity, aerobic and anaerobic blood cultures must be drawn prior to the administration of empiric intravenous antibiotics.
Anesthesia and Positioning
The procedure is best performed under regional anesthesia (axillary or supraclavicular brachial plexus block) or general anesthesia. Local infiltration anesthesia is strongly contraindicated. The acidic environment of the infected tissue neutralizes local anesthetics, rendering them ineffective. Furthermore, injecting fluid into an already pressurized compartment exacerbates pain and risks disseminating the infection into adjacent, uninvolved fascial spaces.
The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination of the limb using an Esmarch bandage is contraindicated to prevent proximal milking of purulent material; instead, the arm should be elevated for three to five minutes prior to tourniquet inflation. The tourniquet is typically inflated to 250 mmHg or 100 mmHg above the patient's systolic blood pressure.
Detailed Surgical Approach and Technique
Drainage of a thenar space abscess can be achieved via a volar approach, a dorsal approach, or a combined through-and-through approach depending on the extent of the infection and the surgeon's preference. The combined approach is often favored for severe infections to facilitate continuous postoperative irrigation.
Volar Approach Dissection
The volar approach provides direct access to the primary cavity of the thenar space.
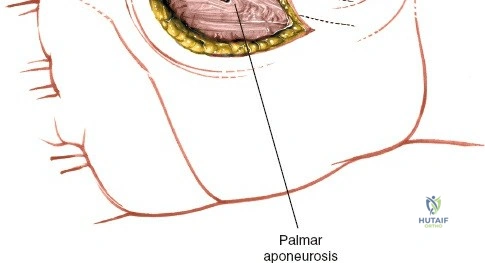
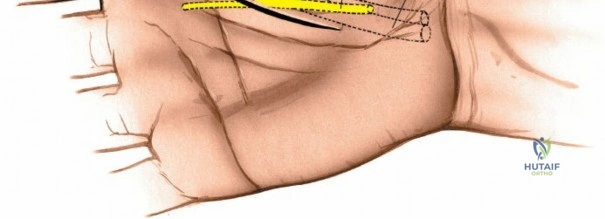
The incision is planned parallel to, and slightly on the thenar side of, the thenar crease. It should not cross the flexion creases at right angles to prevent future flexion contractures. The incision typically begins near the proximal palmar crease and extends distally toward the first web space.
Using a No. 15 scalpel blade, the skin and superficial fascia are incised. Meticulous hemostasis is maintained using bipolar electrocautery. The subcutaneous tissue is carefully spread using blunt dissecting scissors. The surgeon must immediately identify and protect the palmar cutaneous branch of the median nerve proximally and the digital nerves to the index finger distally.
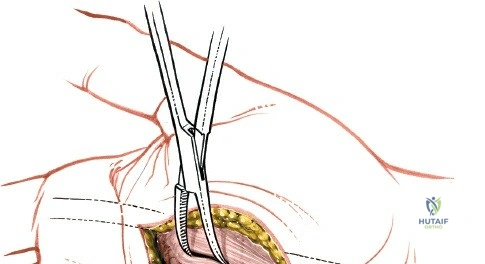
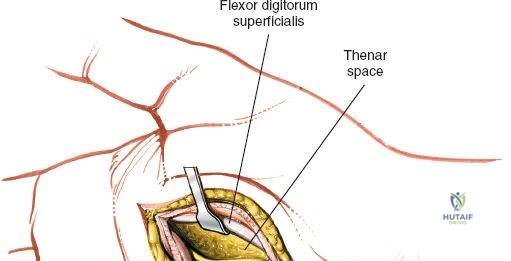
Once the superficial fascia is breached, blunt dissection is utilized to enter the thenar space, which lies deep to the thenar musculature and superficial to the adductor pollicis muscle. A curved hemostat is gently introduced and spread parallel to the neurovascular structures. Entry into the abscess cavity is confirmed by the egress of purulent material.
Dorsal Approach Dissection
For extensive abscesses, or when dependent drainage is desired, a dorsal approach is utilized, often in conjunction with the volar incision.
A longitudinal incision is made on the dorsum of the first web space, overlying the first dorsal interosseous muscle. The incision is carried through the skin and subcutaneous tissue. The dissection proceeds bluntly between the first dorsal interosseous muscle and the adductor pollicis muscle. A hemostat can be passed from the volar incision, through the thenar space, and directed dorsally over the distal edge of the adductor pollicis to tent the dorsal skin, guiding the exact placement of the dorsal incision.
Irrigation and Debridement
Once the space is accessed and purulence is evacuated, comprehensive tissue cultures (aerobic, anaerobic, mycobacterial, and fungal) must be obtained before irrigation begins. Swab cultures are inferior to fluid aspirates or tissue biopsies and should be avoided if possible.
The cavity is then subjected to copious, low-pressure irrigation using several liters of sterile normal saline. Any necrotic fascial or muscular tissue must be sharply debrided until healthy, bleeding margins are encountered. The flexor pollicis longus tendon sheath should be inspected; if it is tense or purulent, a separate incision for flexor tenosynovitis drainage is mandated.
Drain Placement and Closure
Primary closure of the skin is strictly contraindicated in the setting of a deep space hand abscess. The wound must be left open to allow for continued drainage and to prevent reaccumulation of pus.
A passive drain, such as a corrugated Penrose drain, or an active continuous irrigation system utilizing a pediatric feeding tube, is placed through the cavity. If a combined volar-dorsal approach was used, the drain is passed through-and-through. The drain is secured to the skin using a non-absorbable suture. The wound is packed loosely with moist sterile gauze, ensuring that the packing does not create a seal that would impede drainage.
Complications and Management
Despite prompt surgical intervention, complications can arise due to the aggressive nature of the infection or iatrogenic injury during dissection.
Iatrogenic nerve injury is the most feared intraoperative complication. Transection of the recurrent motor branch of the median nerve results in a devastating loss of thumb opposition. Injury to the digital nerves causes painful neuromas and sensory deficits. Vascular injury to the superficial palmar arch or the radialis indicis artery can lead to significant hemorrhage or digital ischemia.
Postoperatively, the most common complication is stiffness of the thumb and index finger due to prolonged immobilization, edema, and subsequent fibrosis. Severe infections can lead to adductor contractures, significantly limiting the first web space span.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Recurrent Motor Nerve Injury | Rare (<1%) | Prevention: Strict adherence to landmarks; avoid proximal/radial extension of the thenar crease incision; blunt dissection deep to fascia. Salvage: Immediate microsurgical epineurial repair. Late presentation requires tendon transfer (e.g., EIP to APB). |
| Digital Nerve Injury | 1-3% | Prevention: Identify nerves superficially before deep dissection. Salvage: Microsurgical repair if recognized intraoperatively. Late reconstruction with nerve grafting if symptomatic. |
| Recurrent Infection / Incomplete Drainage | 5-10% | Prevention: Adequate incision length; thorough loculation breakdown; copious irrigation; avoidance of primary closure. Salvage: Return to the operating room for repeat formal irrigation and debridement. |
| First Web Space Contracture | 10-20% | Prevention: Early active range of motion; appropriate splinting in thumb abduction. Salvage: Aggressive hand therapy. Severe cases may require surgical release (Z-plasty) and adductor fractional lengthening. |
| Osteomyelitis | 2-5% | Prevention: Early initial drainage; directed prolonged antibiotic therapy. Salvage: Surgical debridement of infected bone; prolonged intravenous antibiotics; potential reconstructive bone grafting once infection is cleared. |
Post Operative Rehabilitation Protocols
The postoperative management of a thenar space abscess is as critical as the surgical decompression itself. The goals are to eradicate the infection, maintain functional anatomy, and prevent stiffness.
Immediately postoperatively, the hand is placed in a bulky, non-compressive dressing. A volar resting splint is applied to maintain the hand in the position of safe function (James position).
The wrist is extended 20 to 30 degrees, the metacarpophalangeal joints are flexed 70 to 90 degrees, and the interphalangeal joints are maintained in full extension. Crucially, the thumb must be positioned in wide palmar abduction to prevent adduction contracture of the first web space.
The patient is typically admitted for intravenous antibiotics and elevation of the affected extremity. The initial dressing is taken down at 24 to 48 hours postoperatively. If a continuous irrigation system was utilized, it is generally discontinued at this time, provided the effluent is clear and clinical signs of inflammation have subsided. Drains are advanced or removed based on the volume of drainage.
Once the acute inflammatory phase subsides, early active range of motion is initiated under the guidance of a certified hand therapist. Tendon gliding exercises and web space stretching are paramount. The wounds are allowed to heal by secondary intention, or, if the tissue bed is exceptionally clean and granulating well, delayed primary closure or skin grafting may be considered at 7 to 10 days postoperatively.
Summary of Key Literature and Guidelines
The foundational understanding of the deep fascial spaces of the hand stems from the seminal cadaveric injection studies by Allen B. Kanavel in the early 20th century. Kanavel's meticulous definitions of the thenar, midpalmar, and lumbrical spaces remain the anatomical bedrock for modern hand surgery. His descriptions of the cardinal signs of flexor tenosynovitis and the pathways of infection spread dictate current surgical approaches.
Contemporary literature emphasizes the changing microbiology of hand infections. Guidelines from the Infectious Diseases Society of America (IDSA) strongly recommend empiric coverage for MRSA in all purulent hand infections, particularly in endemic regions or in patients with risk factors such as recent hospitalization or intravenous drug use. Intravenous Vancomycin, Daptomycin, or Linezolid are standard first-line agents pending final culture and sensitivity results.
Recent surgical literature debates the necessity of continuous postoperative irrigation versus simple open drainage. While some retrospective studies suggest continuous irrigation may reduce the need for secondary debridements in severe cases, prospective randomized trials are lacking. The consensus dictates that thorough intraoperative debridement and leaving the wound open for dependent drainage are the most critical factors in preventing recurrence. Furthermore, multidisciplinary management involving orthopedic hand surgeons, infectious disease specialists, and specialized hand therapists is universally recommended to optimize functional outcomes and minimize the long-term morbidity associated with thenar space abscesses.
