Felon (Pulp Space Infection): Advanced Surgical Drainage & Management
Key Takeaway
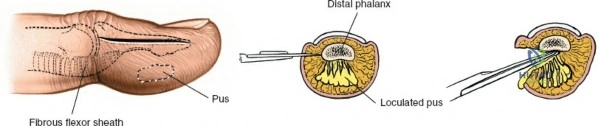
Pulp space infections (felons) are critical fingertip infections. Prompt surgical drainage is essential to decompress confined compartments, relieve acute pressure, and restore vascular perfusion. This prevents severe complications like tissue necrosis, osteomyelitis of the distal phalanx, and septic arthritis, thereby preserving crucial digital function.
Introduction and Epidemiology
Pulp space infections, commonly known as felons, represent one of the most prevalent and critical infections encountered in the hand, frequently necessitating surgical intervention. These infections are confined within the distal phalanx pulp, a unique fibro-fatty compartment susceptible to rapid pressure accumulation. The typical inciting event is a trivial penetrating injury, allowing inoculation of microorganisms into this confined space.
Epidemiologically, felons show a high incidence, particularly among individuals engaged in manual labor or those with compromised immunity such as patients with diabetes mellitus, chronic renal failure, or human immunodeficiency virus. While often considered a minor ailment, the distinct anatomy of the digital pulp predisposes to severe complications if not managed promptly and appropriately. The tightly packed fibrous septa that anchor the skin to the periosteum of the distal phalanx act as barriers, preventing proximal spread of infection but simultaneously limiting outward expansion of pus. This results in an acute rise in intra-compartmental pressure, which can rapidly compromise the vascular supply to the pulp tissue and the underlying distal phalanx, leading to tissue necrosis, osteomyelitis, or even septic arthritis of the distal interphalangeal joint.
Microbiology and Pathogenesis
The predominant causative organisms are Gram-positive cocci, primarily Staphylococcus aureus, including methicillin-resistant S aureus strains, and Streptococcus pyogenes. Less commonly, Gram-negative organisms may be involved, especially in immunocompromised patients, those with specific exposures such as freshwater injuries involving Aeromonas hydrophila, or polymicrobial infections resulting from human or animal bites. In cases of human bites or dental contamination, Eikenella corrodens and anaerobic species must be suspected, whereas Pasteurella multocida is a classic pathogen in feline or canine puncture wounds.
Early diagnosis and judicious management are paramount to prevent irreversible tissue damage and preserve digital function. Differential diagnoses include herpetic whitlow, which is characterized by coalescing vesicles and is typically managed non-surgically with antivirals. Incising a herpetic whitlow is strictly contraindicated as it can lead to viral dissemination, secondary bacterial superinfection, and delayed healing. Other differentials include cellulitis, which lacks a localized abscess, paronychia involving the perionychium and nail fold, and foreign body granulomas.
Surgical Anatomy and Biomechanics
A thorough understanding of the unique surgical anatomy of the fingertip pulp is fundamental to effective and safe surgical drainage of a felon. The distal finger pulp consists of a dense network of fibrous septa that extend radially from the periosteum of the distal phalanx to the dermis of the volar skin. These septa divide the pulp into numerous small, vertically oriented compartments, each containing fat, sweat glands, nerve endings, and a rich vascular supply.
The vascularity of the fingertip is robust, supplied by the terminal branches of the radial and ulnar digital arteries. These vessels form an extensive capillary network within the pulp. The close proximity of these delicate vessels to the unyielding fibrous septa is critical. Even a small collection of pus within one of these compartments can lead to a significant increase in local tissue pressure. This pressure elevation can quickly exceed capillary perfusion pressure, resulting in localized ischemia, infarction, and necrosis of the pulp tissue and potentially the underlying bone.
Osseous Vascularity and Osteomyelitis Risk
The distal phalanx lies directly beneath the pulp, making it vulnerable to osteomyelitis, particularly if the infection is deep-seated or inadequately drained. The vascular supply to the distal phalanx is highly specific and clinically relevant. The epiphyseal base of the distal phalanx receives its blood supply proximal to the fibrous septa of the pulp space. In contrast, the diaphyseal blood supply traverses directly through the pressurized pulp space. Consequently, an untreated felon with high compartmental pressure will typically cause ischemic necrosis and subsequent osteomyelitis of the diaphysis of the distal phalanx, while the epiphyseal base and the distal interphalangeal joint are initially spared.
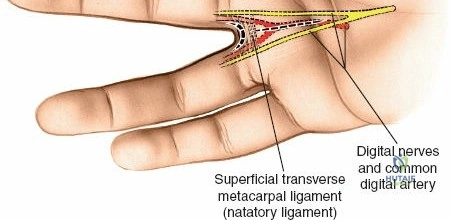
Sensory innervation is provided by the terminal branches of the digital nerves, which are highly concentrated in the fingertips, contributing to their exquisite tactile sensitivity. The pulp contains a high density of Meissner corpuscles, Pacinian corpuscles, and free nerve endings. Incisions must be planned meticulously to avoid damage to these neurovascular structures, particularly the main digital neurovascular bundles that run along the lateral aspects of the digits, slightly volar to the mid-lateral line. Furthermore, the nail matrix, responsible for nail growth, is located at the base of the nail and can be inadvertently damaged by aggressive surgical techniques or proximal extension of the infection, leading to permanent nail deformity.
Indications and Contraindications
The decision to proceed with surgical drainage versus conservative management hinges on the presence of a localized abscess or fluctuance, the duration of symptoms, and the patient's systemic response. Early presentations characterized entirely by cellulitis without a discrete fluid collection may be managed with aggressive intravenous or oral antibiotics, elevation, and close observation. However, once a distinct abscess cavity forms, or if the digital pulp becomes tense, exquisitely tender, and throbbing, surgical decompression is absolutely indicated to prevent ischemic necrosis and osteomyelitis.
Operative and Non Operative Decision Matrix
| Clinical Presentation | Recommended Management | Rationale |
|---|---|---|
| Early cellulitis without fluctuance | Non-Operative | Antibiotics and elevation are sufficient before abscess consolidation. |
| Tense throbbing pulp with fluctuance | Operative Drainage | Relieves compartment pressure and prevents diaphyseal ischemia. |
| Visible purulence or pointing abscess | Operative Drainage | Evacuation of necrotic debris and bacterial load is required. |
| Herpetic Whitlow clear vesicles | Non-Operative | Incision causes secondary bacterial infection and viral spread. |
| Failure of 48 hours of antibiotics | Operative Drainage | Suggests occult abscess formation requiring mechanical decompression. |
| Presence of foreign body | Operative Drainage | Source control requires physical extraction of the nidus. |
Contraindications to surgical drainage primarily revolve around misdiagnosis. The most critical absolute contraindication is the presence of a herpetic whitlow. Surgical intervention in herpetic whitlow provides no benefit and significantly increases morbidity. Relative contraindications include profound bleeding diatheses or severe peripheral vascular disease where incisions may fail to heal, though the risk of leaving a pressurized infection usually outweighs the risks of surgical intervention. In such ischemic digits, careful consultation with vascular surgery and meticulous technique are required.
Pre Operative Planning and Patient Positioning
Thorough preoperative evaluation is necessary to optimize surgical outcomes and minimize complications. Standard anterior-posterior and lateral radiographs of the affected digit are mandatory. Imaging serves to rule out pre-existing osteomyelitis, identify radiopaque foreign bodies, and assess for any underlying fractures or joint involvement. If osteomyelitis is identified preoperatively, the surgical plan must be expanded to include aggressive bone debridement or potential partial amputation, depending on the extent of osseous destruction.
Anesthesia and Hemostasis
Adequate anesthesia is critical for a thorough exploration and decompression. A digital block utilizing a long-acting local anesthetic, such as bupivacaine or ropivacaine, is standard. The use of epinephrine in digital blocks remains a topic of academic debate. While modern literature supports the safety of epinephrine in healthy digits, many hand surgeons avoid its use in the setting of a felon. The digital pulp is already suffering from microvascular compromise due to elevated compartmental pressure; adding a vasoconstrictive agent may theoretically exacerbate ischemia and precipitate tissue necrosis. Therefore, plain local anesthetics are generally preferred.
Hemostasis is achieved through the use of a digital tourniquet. A sterile Penrose drain or a commercial rolled digit tourniquet can be applied to the base of the finger. Care must be taken to avoid excessive pressure, and the tourniquet must be removed promptly after the procedure to restore perfusion. Forearm or arm tourniquets are generally unnecessary for isolated felon drainage but may be utilized if more extensive proximal exploration is anticipated.
Patient Positioning
The patient is typically positioned supine with the affected upper extremity extended on a radiolucent hand table. The hand should be prepped and draped in a standard sterile fashion. The surgeon should be seated comfortably with adequate lighting, and loupe magnification is highly recommended to visualize the delicate fibrous septa, digital nerves, and to ensure complete evacuation of the abscess cavity without iatrogenic injury.
Detailed Surgical Approach and Technique
The surgical management of a felon requires precise technique to achieve adequate decompression while minimizing functional and cosmetic morbidity. The primary goal is the complete division of the fibrous septa within the infected compartment to allow free drainage of purulent material and relieve pressure.
Incision Selection
The choice of incision is dictated by the location of the abscess and the pointing of the infection. Several historical incisions, such as the fish-mouth, hockey-stick, and through-and-through incisions, have been largely abandoned due to unacceptably high rates of complications, including painful neuromas, unstable fingertip pads, and severe vascular compromise.
Modern surgical practice advocates for one of two primary approaches:
- Volar Longitudinal Incision: This is currently the most widely accepted approach for a centrally located felon. The incision is made directly over the point of maximal fluctuance or pointing. It should not cross the distal interphalangeal joint flexion crease to prevent flexion contractures. The advantage of this approach is direct access to the abscess and minimal disruption of uninvolved tissue planes. The primary disadvantage is the potential for a tender volar scar, although careful technique minimizes this risk.
- High Lateral Incision: This approach is utilized when the infection is localized to one side of the pulp or when aiming to avoid a volar scar. The incision is placed dorsal to the neurovascular bundle, approximately 0.5 cm distal to the distal interphalangeal joint crease, and extends distally parallel to the nail edge. The incision must remain dorsal to the tactile pad to prevent a painful neuroma on the working surface of the digit.
Dissection and Decompression
Once the skin is incised using a No. 15 or No. 11 scalpel blade, blunt dissection is strictly employed to enter the pulp space. A fine hemostat or blunt scissors is introduced into the wound. The instrument is gently spread to break the loculations created by the fibrous septa. It is imperative to divide these septa thoroughly to convert the multiple small compartments into a single cavity, ensuring complete decompression.
During dissection, the surgeon must be acutely aware of the depth and trajectory of the instruments. The dissection must not violate the distal interphalangeal joint capsule proximally or the flexor tendon sheath. Iatrogenic penetration of the flexor tendon sheath will convert a localized felon into a catastrophic purulent flexor tenosynovitis. Furthermore, aggressive scraping of the distal phalanx periosteum should be avoided unless frank osteomyelitis is present and debridement is required.
Irrigation and Wound Management
Following complete septal release and evacuation of purulence, deep tissue cultures should be obtained, particularly in immunocompromised patients, those with atypical exposures, or recurrent infections. The cavity is then copiously irrigated with sterile saline.
The wound is left open to heal by secondary intention. To prevent premature closure of the skin edges and re-accumulation of pus, a small wick or loose packing is placed into the cavity. Iodoform gauze, plain fine mesh gauze, or a small piece of a silicone drain can be utilized. The packing must be placed loosely; tight packing will recreate the compartment syndrome effect and induce further ischemia. A bulky, non-compressive sterile dressing is applied, and the digit is splinted in a functional position to protect the wound and provide pain relief.
Complications and Management
Despite appropriate surgical intervention, complications can arise from delayed presentation, virulent organisms, or technical errors during drainage. Recognizing and managing these complications promptly is essential for preserving digital function.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology and Salvage Strategy |
|---|---|---|
| Osteomyelitis of Distal Phalanx | 5-10% | Caused by prolonged pressure ischemia to the diaphyseal blood supply. Management requires aggressive surgical debridement of necrotic bone, targeted prolonged intravenous antibiotics, and occasionally terminal amputation if destruction is severe. |
| Skin and Pulp Necrosis | 2-5% | Results from delayed decompression or excessively tight postoperative packing. Requires sharp debridement of non-viable tissue. Small defects heal by secondary intention; larger defects may require local advancement flaps (e.g., V-Y plasty) once the infection clears. |
| Purulent Flexor Tenosynovitis | < 1% | Iatrogenic complication from plunging instruments too proximally during drainage. Requires immediate return to the operating room for formal flexor sheath irrigation and catheter placement. |
| Painful Neuroma | 1-3% | Caused by sharp transection of terminal digital nerve branches, often associated with historical fish-mouth incisions. Managed initially with desensitization therapy. Refractory cases may require surgical neuroma excision and burying of the nerve stump. |
| Septic Arthritis of DIP Joint | < 1% | Results from proximal extension of a neglected infection or iatrogenic capsular violation. Necessitates formal arthrotomy, joint irrigation, and potential arthrodesis if the articular cartilage is destroyed. |
Osteomyelitis remains the most significant osseous complication. If suspected postoperatively due to persistent drainage or lack of clinical improvement, repeat radiographs or magnetic resonance imaging should be obtained. Treatment mandates formal bone debridement, sending deep bone margins for culture and histopathology to confirm eradication.
Soft tissue complications, such as pulp sloughing, require patience. The fingertip has a remarkable capacity for healing by secondary intention. Once the infection is eradicated, aggressive wound care and eventual reconstruction with local flaps can be considered for functionally limiting defects.
Post Operative Rehabilitation Protocols
The postoperative management of a felon is as critical as the surgical decompression itself. The initial postoperative check should occur within 48 to 72 hours. At this visit, the bulky dressing and the surgical wick are removed. The wound is inspected for signs of residual loculations, progressing necrosis, or surrounding cellulitis.
Wound Care and Therapy
Once the wick is removed, it is generally not replaced unless a massive cavity remains. Instead, the patient is instructed to begin warm water or dilute povidone-iodine soaks two to three times daily. These soaks facilitate mechanical debridement of residual exudate, promote local vasodilation to enhance healing, and prevent the skin edges from closing prematurely. Following each soak, a simple dry sterile dressing or a non-adherent dressing is applied.
Early mobilization is a cornerstone of hand surgery rehabilitation. As soon as clinical pain allows, usually within the first few days postoperatively, the patient must begin active range of motion exercises for the distal interphalangeal, proximal interphalangeal, and metacarpophalangeal joints. Prolonged immobilization leads to rapid joint stiffness and tendon adhesions. Hand therapy may be formally prescribed if the patient demonstrates apprehension or difficulty achieving full excursion.
Healing and Return to Function
The wound typically heals by secondary intention over a period of two to four weeks. During the proliferative phase of wound healing, hypergranulation tissue may occasionally develop, protruding beyond the skin margins and impeding epithelialization. This can be effectively managed with topical application of silver nitrate in the clinic setting.
Return to work and normal activities is dictated by the patient's occupation and the rate of healing. Manual laborers or those exposed to heavily contaminated environments may require modified duties until complete epithelialization occurs to prevent secondary infection. Desensitization protocols, involving tapping, massage, and exposure to various textures, should be initiated once the wound is closed to mitigate scar hypersensitivity.
Summary of Key Literature and Guidelines
The foundational principles of hand infection management were established by Kanavel in the early 20th century. While his classic text primarily focused on flexor tenosynovitis and deep fascial space infections, the core tenets of early diagnosis, precise anatomical incisions, and adequate drainage remain directly applicable to the management of felons.
Modern literature has significantly refined the surgical approach to pulp space infections. Historical texts frequently described the fish-mouth and hockey-stick incisions; however, contemporary outcome studies have universally condemned these approaches. Evidence demonstrates that these extensive incisions compromise the blood supply to the distal pulp, leading to a high incidence of pulp necrosis, unstable tactile pads, and debilitating neuromas. Current guidelines strongly advocate for the volar longitudinal incision or the high lateral incision, emphasizing minimal soft tissue disruption and targeted decompression.
Infectious Diseases Society of America guidelines provide critical frameworks for the antimicrobial management of hand infections. Given the rising prevalence of community-acquired methicillin-resistant Staphylococcus aureus, empiric antibiotic therapy following surgical drainage must routinely include agents with anti-MRSA activity, such as trimethoprim-sulfamethoxazole, doxycycline, or clindamycin, pending definitive culture and susceptibility results. Furthermore, literature regarding animal and human bites dictates specific empiric coverage, such as amoxicillin-clavulanate, to address Pasteurella and Eikenella species, respectively.
Academic consensus underscores that antibiotics are an adjunct to, not a replacement for, adequate surgical decompression in the presence of a formed abscess. Failure to achieve mechanical source control inevitably leads to treatment failure, prolonged morbidity, and escalation of complications. Continuous adherence to meticulous surgical technique and evidence-based postoperative protocols ensures optimal functional recovery for patients presenting with these challenging infections.
