Operative Management of Recalcitrant Plantar Fasciitis and Heel Pain Syndrome
Key Takeaway
Plantar fasciitis is the most common cause of inferior heel pain, typically resolving with conservative management. However, recalcitrant cases may require surgical intervention. This guide details the pathoanatomy, clinical evaluation, and operative management of chronic heel pain syndrome, focusing on the open release of the plantar fascia and decompression of the first branch of the lateral plantar nerve to achieve optimal postoperative outcomes.
INTRODUCTION AND PATHOANATOMY
Plantar fasciitis, more accurately termed plantar fasciosis, is the most prevalent cause of inferior heel pain in adults. Histological analysis of surgical specimens rarely demonstrates acute inflammatory cells; rather, the condition is characterized by angiofibroblastic hyperplasia, collagen necrosis, and chondroid metaplasia near the fascial origin at the medial calcaneal tuberosity. This degenerative cascade is primarily driven by repetitive microtrauma and mechanical overload of the plantar aponeurosis, particularly during the toe-off phase of the gait cycle when the windlass mechanism is maximally engaged.
Most patients presenting with heel pain are between 40 and 70 years of age. The condition is frequently observed in active individuals, though obesity remains a profound predisposing factor. Increased body mass index (BMI) exponentially increases the mechanical load on the longitudinal arch, making symptoms notoriously difficult to control in overweight patients. While the exact biomechanical influence of pes planus (flatfoot) or pes cavus (high arch) remains debated, both extremes of arch morphology alter load distribution and can predispose individuals to fascial microtearing.
Epidemiological data from U.S. military personnel (Scher et al.) identified female sex, Black race, and increasing age as independent risk factors for the development of plantar fasciitis, challenging the historical assumption of a strict male predominance.
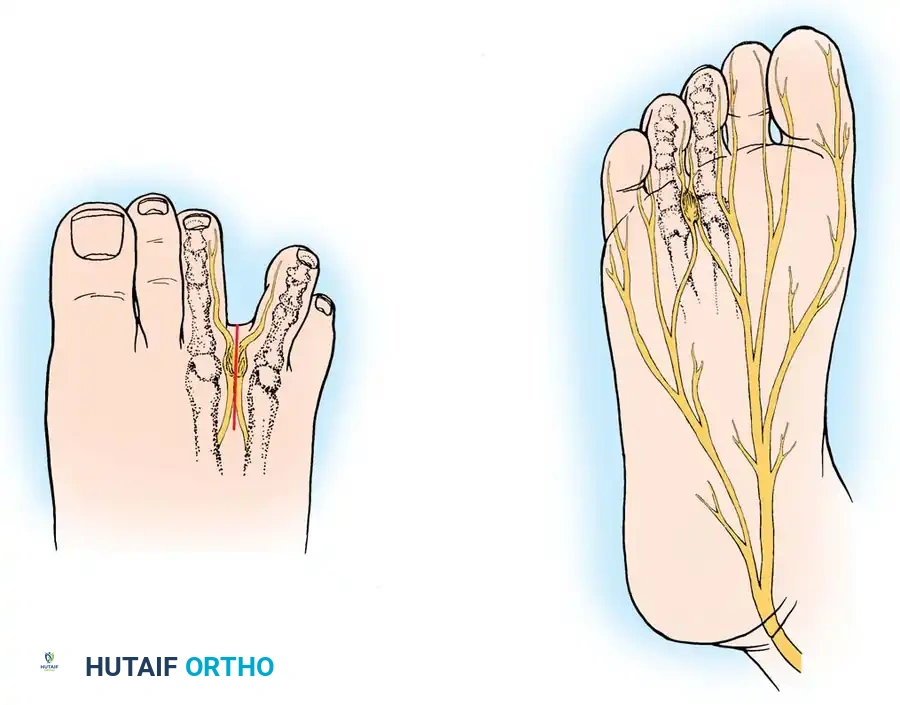
Furthermore, chronic heel pain syndrome is frequently multifactorial. In recalcitrant cases, mechanical fasciosis is often compounded by localized nerve entrapment. The first branch of the lateral plantar nerve (Baxter’s nerve) is particularly vulnerable to compression as it courses between the deep fascia of the abductor hallucis and the medial caudal border of the quadratus plantae.
CLINICAL AND RADIOGRAPHIC FINDINGS
History and Physical Examination
The hallmark complaint of plantar fasciitis is severe, sharp pain beneath the heel that is most pronounced upon taking the first steps in the morning or after a prolonged period of sitting (post-static dyskinesia). As the plantar fascia stretches with ambulation, the sharp pain typically diminishes, allowing the patient to be reasonably comfortable during the day. However, toward the end of the day, or following prolonged weight-bearing, the discomfort transitions into a deep, throbbing ache that is only relieved by rest.
The most consistent physical finding is localized, exquisite tenderness at the inferomedial aspect of the calcaneal tuberosity—the anatomical origin of the central band of the plantar fascia.
Clinical Pearl: When evaluating heel pain, always compare the symptomatic heel with the asymptomatic contralateral side. Mild swelling and localized erythema may be apparent. Furthermore, carefully palpate the tibial nerve and its branches beneath the flexor retinaculum. A positive Tinel's sign or localized tenderness over the course of Baxter's nerve suggests a neuropathic component that may necessitate surgical decompression.
Diagnostic Imaging
While plantar fasciitis is primarily a clinical diagnosis and one of exclusion, imaging modalities are invaluable for ruling out competing pathologies (e.g., calcaneal stress fractures, tarsal tunnel syndrome, osteomyelitis) and guiding surgical planning in recalcitrant cases.
- Radiographs: Weight-bearing lateral radiographs reveal a plantar calcaneal spur in approximately 50% of patients. It is critical to understand—and to educate the patient—that the spur is a traction osteophyte located within the origin of the flexor digitorum brevis, not the plantar fascia itself. The spur is a radiographic marker of chronic tension, not the primary pain generator.
- Magnetic Resonance Imaging (MRI): MRI is the gold standard for delineating soft tissue and bony anatomy. In a review of 50 patients with persistent heel pain, MRI confirmed the diagnosis in 76%. Pathognomonic findings include fascial thickening (>4 mm), intrasubstance signal changes, and adjacent calcaneal marrow edema. MRI is particularly useful for identifying atypical pathology, such as partial or complete plantar fascia ruptures, plantar fibromatosis, or arteriovenous malformations.
- Bone Scintigraphy (Technetium-99m): Bone scans demonstrate focal isotope uptake at the anteroinferior medial aspect of the calcaneus. This modality is highly sensitive and is particularly useful in patients with equivocal diagnoses or to definitively rule out a calcaneal stress fracture.
- Electromyography (EMG): EMG and nerve conduction studies of the abductor digiti minimi muscle may be indicated if symptoms persist for several months and Baxter's nerve entrapment is suspected.
EVIDENCE-BASED CONSERVATIVE MANAGEMENT
Surgical intervention is rarely the first-line treatment for a painful heel. Literature consistently demonstrates that over 90% of patients with plantar fasciitis can be successfully managed nonoperatively. A comprehensive, multimodal conservative protocol must be exhausted for a minimum of 6 to 12 months before considering surgical release.
First-Line Modalities:
* Mechanical Support: Silicone heel cups, arch pads, and rigid or semi-rigid orthoses reduce dynamic tension on the fascial origin.
* Pharmacotherapy: Oral nonsteroidal anti-inflammatory drugs (NSAIDs) provide symptomatic relief of the secondary inflammatory response.
* Physical Therapy: A specific, directed plantar fascia and Achilles tendon stretching regimen is the cornerstone of conservative care.
Advanced Nonoperative Modalities:
* Corticosteroid Injections (CSI): Local CSI provides rapid, albeit sometimes temporary, pain relief. However, patients must be explicitly warned about the risk of iatrogenic plantar fascia rupture and plantar fat pad atrophy.
* Biologics: Prospective, randomized controlled trials comparing intralesional autologous blood or Platelet-Rich Plasma (PRP) injections with CSI have shown that while CSI offers superior immediate onset of relief, biologic injections provide sustained reduction in pain and tenderness without the risk of fascial rupture.
* Extracorporeal Shock Wave Therapy (ESWT): High-energy ESWT has demonstrated efficacy in stimulating neovascularization and tissue regeneration in recalcitrant cases, though large-scale randomized consensus remains variable.
SURGICAL INDICATIONS AND DECISION MAKING
Surgery is indicated only for patients whose symptoms persist over an extended period (typically >12 months) despite exhaustive conservative management, and whose pain significantly impairs their quality of life.
Surgical Warning: Preoperative patient counseling is paramount. The patient must be made fully aware that surgery carries no absolute guarantee of symptom resolution. Furthermore, if the chosen procedure does not involve the excision of an existing calcaneal spur, the patient must be informed beforehand to prevent postoperative psychological dissatisfaction.
Historically, numerous procedures have been described, including elevation of the heel pad, isolated neurolysis, calcaneal osteotomy, and simple calcaneal drilling ("decompression"). Today, the standard of care revolves around the partial release of the plantar fascia, with or without the decompression of the first branch of the lateral plantar nerve.
Open vs. Endoscopic Approaches
- Endoscopic Plantar Fasciotomy (EPF): EPF allows for a limited release of the central cord of the fascia with minimal soft tissue dissection. Saxena reported excellent results in athletic populations, allowing return to sports within 3 months. However, EPF does not allow for direct visualization and decompression of Baxter's nerve.
- Open Plantar Fascia and Nerve Release: Most patients with chronic heel pain syndrome who ultimately require surgery exhibit clinical evidence of Baxter's nerve entrapment. Therefore, an open approach (as described by Schon and Baxter) is preferred. This allows for a comprehensive procedure: partial plantar fasciotomy, neurolysis of the nerve to the abductor digiti minimi, and, if necessary, excision of the calcaneal spur.
SURGICAL TECHNIQUE: OPEN PLANTAR FASCIOTOMY AND NERVE DECOMPRESSION (SCHON; BAXTER)
The following technique details a comprehensive single-incision approach for the release of the plantar fascia, neurolysis of the nerve to the abductor digiti minimi, release of the flexor digitorum brevis, and optional excision of the anterior tuberosity of the calcaneus.
1. Preoperative Setup and Positioning
- Anesthesia: The procedure can be performed under general anesthesia, regional block (popliteal or ankle block), or local anesthesia with intravenous sedation.
- Positioning: Place the patient supine on the operating table. The affected lower extremity is externally rotated to provide unhindered access to the medial aspect of the heel.
- Hemostasis: A thigh or calf tourniquet may be utilized based on surgeon preference. If a tourniquet is omitted, place the patient in a slight Trendelenburg position to reduce venous backflow.
- Visualization: The use of 2.5× surgical loupe magnification is routinely recommended to safely identify and protect the delicate neural structures.
- Prophylaxis: Administer prophylactic intravenous antibiotics prior to incision.
2. Incision and Superficial Dissection
- Incision Planning: Locate the starting point by bisecting a longitudinal axial line running 1 cm posterior to the posterior edge of the medial malleolus.
- Make an oblique 3- to 4-cm incision along the medial aspect of the heel. The incision should overlie the anatomical course of the first branch of the lateral plantar nerve and the proximal edge of the abductor hallucis muscle belly. Direct the incision obliquely in a distal and plantar direction, terminating at the junction of the plantar and medial skin.
- Subcutaneous Dissection: Carry sharp dissection through the subcutaneous fat.
- Crucial Step: Pay meticulous attention to identifying and protecting the superficial medial calcaneal nerve branches. Retract these sensory branches gently. Note that a layer of subcutaneous fascia is often encountered before the true superficial fascia of the abductor hallucis; do not confuse the two.
3. Deep Dissection and Fascial Identification
- Identify the true superficial fascia of the abductor hallucis muscle. Insert a self-retaining retractor to maintain exposure.
- To locate the plantar fascia, pass a Freer elevator from the medial distal edge of the abductor hallucis in a plantar and lateral direction.
- Insert a small, toothed lamina spreader at the junction of the abductor fascia and the plantar fascia. Place a Senn retractor distally between the two arms of the lamina spreader to optimize visualization of the plantar fascial band.
4. Release of the Abductor Hallucis and Nerve Decompression
- With exposure secured, use a scalpel to sharply release the superficial fascia of the abductor hallucis.
- Using a Freer elevator, carefully identify the deep fascia of the abductor hallucis. This fascial layer is distinctly concave and must be clearly visualized before any release is attempted.
- Use a Senn retractor to retract the abductor muscle belly superiorly. Carefully release the deep fascia of the abductor with a scalpel.
- Anatomical Safe Zone: Directly beneath this deep fascia lies a fat pad, an artery, a vein, and the first branch of the lateral plantar nerve (Baxter's nerve).
- Reposition the Senn retractor superiorly and retract the abductor muscle distally. This permits a complete, unhindered release of the deep fascia from this vector, effectively decompressing the lateral plantar nerve.
Surgical Pearl: In approximately 20% of patients, Baxter's nerve is directly visible without further dissection. It is highly recommended not to routinely dissect out the nerve itself. Overzealous dissection causes unnecessary bleeding, devascularization, and iatrogenic trauma that can lead to severe postoperative perineural fibrosis. Decompression is achieved purely through the meticulous release of the overlying fascia.
- Ensure careful fascial release when the sharp edge of the medial caudal border of the quadratus plantae is palpated, as this is a primary site of nerve entrapment.
5. Partial Plantar Fasciotomy
- Direct attention to the inferior aspect of the surgical wound, where the medial band of the plantar fascia is clearly visible.
- Perform a partial fasciotomy, releasing only the medial 30% to 50% of the plantar fascia from its calcaneal origin.
Surgical Pitfall: Never perform a complete (100%) release of the plantar fascia. Complete transection catastrophically destabilizes the longitudinal arch, abolishes the windlass mechanism, and predictably leads to lateral column overload, cuboid stress fractures, and acquired pes planus.
- If preoperative planning and patient discussion dictated the removal of a prominent calcaneal spur, use a rongeur or an osteotome to resect the exostosis at this stage. Use a rasp to smooth the remaining calcaneal surface.
- Irrigate the wound copiously with sterile saline.
- Deflate the tourniquet (if used) and achieve meticulous hemostasis using electrocautery.
- Close the subcutaneous tissue with absorbable sutures and the skin with non-absorbable horizontal mattress sutures or a subcuticular closure, depending on surgeon preference.
POSTOPERATIVE REHABILITATION PROTOCOL
Optimal postoperative care is essential to prevent stiffness and ensure a successful return to function.
- Phase I (Weeks 0-2): The patient is placed in a bulky, soft compressive dressing and a short-leg controlled ankle motion (CAM) boot. Weight-bearing is typically restricted to touch-down or partial weight-bearing with crutches to protect the incision and allow soft tissue healing. Elevation and cryotherapy are strictly enforced to minimize edema.
- Phase II (Weeks 2-6): Sutures are removed at 10 to 14 days. The patient is transitioned to weight-bearing as tolerated (WBAT) in the CAM boot. Gentle, active range-of-motion (ROM) exercises for the ankle and toes are initiated. Deep friction massage over the incision site is encouraged to prevent restrictive scar tissue formation.
- Phase III (Weeks 6-12): The patient is transitioned to supportive athletic footwear with a custom orthotic or supportive heel cup. Formal physical therapy focuses on intrinsic foot muscle strengthening, Achilles tendon stretching, and proprioceptive training.
- Return to Play: Most patients, including high-level athletes, can expect to return to full, unrestricted sporting activities (such as running) between 3 and 4 months postoperatively, provided they are pain-free and have regained full baseline strength.
COMPLICATIONS
While generally safe and effective, operative management of plantar fasciitis carries specific risks:
* Lateral Column Overload: The most common biomechanical complication, resulting from an over-aggressive (>50%) release of the plantar fascia. Patients present with new-onset pain over the cuboid or base of the 5th metatarsal.
* Nerve Injury: Iatrogenic injury to the medial calcaneal nerve branches (causing heel numbness) or Baxter's nerve (causing chronic neuropathic pain).
* Infection and Wound Dehiscence: Particularly in diabetic or obese patients.
* Persistent Pain: Failure to achieve pain relief occurs in 5-10% of patients, often due to inadequate nerve decompression, incorrect initial diagnosis, or irreversible degenerative changes within the heel pad.
You Might Also Like