Transfer of Extensor Hallucis Longus with Arthrodesis of the Interphalangeal Joint of the Hallux
Key Takeaway
The transfer of the extensor hallucis longus (EHL) combined with arthrodesis of the interphalangeal (IP) joint is a powerful surgical technique for correcting supple hallux varus deformities. By fusing the IP joint, the flexor hallucis longus acts exclusively on the metatarsophalangeal joint, correcting extension contractures. This guide details the Johnson and Spiegl technique, providing orthopedic surgeons with step-by-step instructions, biomechanical rationale, and critical pearls for optimal patient outcomes.
Introduction to Hallux Varus and Dynamic Tendon Transfers
Iatrogenic hallux varus is a complex, multiplanar deformity most commonly encountered as a complication following aggressive hallux valgus corrective surgery. The deformity is characterized by medial deviation of the great toe at the metatarsophalangeal (MTP) joint, often accompanied by MTP joint extension and interphalangeal (IP) joint flexion (a claw toe or malleus deformity). The underlying pathophysiology typically involves over-resection of the medial eminence, excessive lateral soft tissue release, or inadvertent excision of the fibular sesamoid, leading to a profound musculotendinous imbalance.
When conservative measures fail, surgical intervention is dictated by the flexibility of the MTP and IP joints. For a static, rigid, or arthritic MTP joint, arthrodesis remains the gold standard. However, for a supple deformity of the MTP joint, dynamic tendon transfer—specifically the transfer of the extensor hallucis longus (EHL) combined with IP joint arthrodesis—is highly recommended.
The Johnson and Spiegl technique is the premier surgical method for this dynamic reconstruction. By rerouting the EHL tendon to act as a lateral tether and plantarflexor at the MTP joint, the deforming forces are neutralized, restoring the biomechanical axis of the first ray.
Biomechanical Rationale and Surgical Indications
Understanding the biomechanics of the first ray is critical for executing this procedure successfully.
Why Arthrodese the Interphalangeal Joint?
When the EHL is detached from its insertion at the distal phalanx to be transferred proximally, the hallux loses its primary active extensor of the IP joint. If the IP joint is left intact, the unopposed pull of the flexor hallucis longus (FHL) will rapidly drive the toe into a rigid flexion deformity (clawing).
Furthermore, fusion of the IP joint provides a distinct biomechanical advantage at the MTP joint. By eliminating motion at the IP joint, the FHL's excursion and force are redirected entirely to the MTP joint. The FHL becomes a powerful plantarflexor of the great toe at the MTP joint, directly counteracting the MTP extension contracture that is universally present in hallux varus.
Surgical Pearl: Transferring only half of the EHL tendon (split transfer) in an attempt to preserve IP joint motion is biomechanically inappropriate. A split transfer requires a single muscle belly to perform two simultaneous, conflicting actions: extension of the IP joint and adduction/plantarflexion of the MTP joint. This inevitably leads to weakness, recurrent deformity, and surgical failure.
Indications
- Supple Hallux Varus: The MTP joint must be passively correctable to a neutral alignment without significant degenerative joint disease.
- Dynamic MTP Extension Deformity: Often seen in conjunction with varus.
- Failed Soft Tissue Reconstructions: Patients who have failed isolated medial capsular reefing or abductor hallucis release.
Contraindications
- Rigid/Fixed Deformity: If the MTP joint cannot be passively reduced, a tendon transfer will fail. MTP arthrodesis is required.
- Severe Degenerative Joint Disease: Osteoarthritis of the first MTP joint precludes a joint-sparing procedure.
- Neuromuscular Disorders: Spasticity or profound neuropathy (e.g., advanced Charcot arthropathy) compromises the predictability of tendon transfers.
Preoperative Planning and Patient Counseling
Thorough preoperative counseling is mandatory. The patient must be explicitly informed that while the tendon transfer is planned, intraoperative findings may necessitate a primary MTP joint arthrodesis if the deformity proves more rigid than anticipated.
Furthermore, patients must understand that the primary goal of this surgery is a stable, plantigrade, and well-aligned toe. Both the EHL transfer and the IP joint arthrodesis will reduce the overall arc of motion of the great toe. The patient must be willing to accept a reduction in MTP joint motion in exchange for the correction of the deformity.
Surgical Technique: The Johnson and Spiegl Procedure
The procedure is performed under regional or general anesthesia with a well-padded calf or thigh tourniquet to ensure a bloodless surgical field. The patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position.
Step 1: Incision and Exposure
Begin with an L-shaped incision to maximize exposure of both the MTP and IP joints while respecting the dorsal angiosomes of the hallux.
- Initiate the incision in the first web space, between the midportions of the first and second metatarsals.
- Extend the incision distally along the dorsolateral aspect of the great toe.
- Curve the incision medially as it approaches the insertion of the EHL tendon at the base of the distal phalanx.

Surgical Warning: Meticulous dissection is required to identify and protect the dorsal medial and dorsal lateral cutaneous nerves of the hallux. Injury to these nerves will result in a painful postoperative neuroma, which can severely compromise an otherwise successful structural correction. Additionally, avoid violating the germinal matrix of the nail bed during the distal exposure.
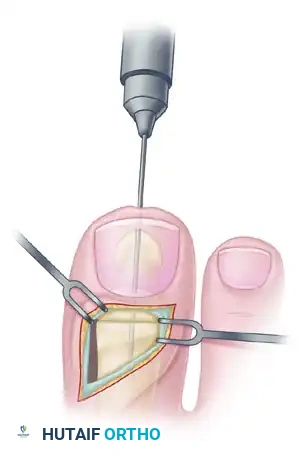
Step 2: EHL Tendon Harvest
- Identify the EHL tendon at its distal insertion on the base of the distal phalanx.
- Sharply divide the tendon directly at its bony insertion to maximize functional length.
- Dissect the EHL tendon free from the extensor hood mechanism and its proximal fascial attachments. Mobilize the tendon 5 to 6 cm proximal to the MTP joint to ensure adequate excursion for the transfer.
Step 3: Preparation for Interphalangeal Joint Arthrodesis
With the EHL detached, the IP joint is easily accessed.
- Perform a transverse arthrotomy of the IP joint.
- Acutely flex the distal phalanx to expose the articular surfaces of both the head of the proximal phalanx and the base of the distal phalanx.
- Using a microsaw or rongeur, resect the articular cartilage down to bleeding subchondral bone. The cuts should be flat and parallel to permit a neutral position in both the sagittal and coronal planes.

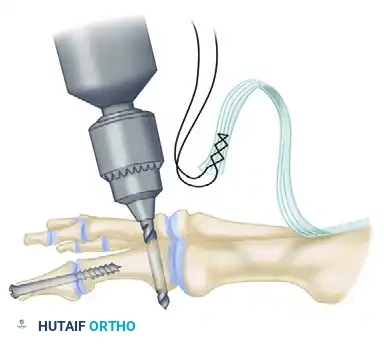
Step 4: IP Joint Fixation (Shives and Johnson Technique)
Rigid internal fixation is paramount for a successful arthrodesis. The use of a 4.0-mm cancellous lag screw, as advocated by Shives and Johnson, provides excellent compression and rotational stability.
- Retrograde Drilling: Drill a 2.0-mm diameter hole longitudinally in a retrograde manner starting at the center of the denuded articular surface of the distal phalanx.
- The drill bit should exit the skin at a point exactly 5 mm plantar to the tip of the nail in the midline of the toe.

- Antegrade Drilling: Appose the denuded articular surfaces of the proximal and distal phalanges in neutral alignment. Insert the drill bit distally at the tip of the toe (through the previously created exit hole) and advance it proximally.
- Follow the previously placed retrograde hole, cross the IP joint, and drill into the base of the proximal phalanx, advancing down the center of its medullary canal.

- Overdrilling and Tapping: To achieve a true lag effect, overdrill the distal phalanx (the near cortex) with a 2.7-mm drill bit to create a gliding hole. Tap the entire drill path with a 3.5-mm tap to prepare for the cancellous screw.
- Screw Insertion: Following the drill path in a proximal direction, insert a 4.0-mm partially threaded cancellous bone screw.
- As the screw head engages the distal phalanx, the lag effect will produce robust compression across the arthrodesis site, ensuring firm fixation.

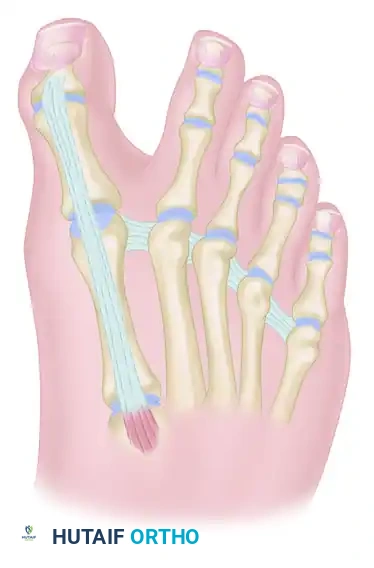
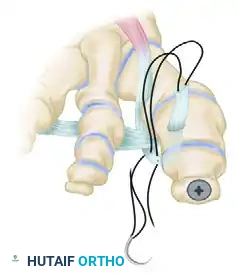
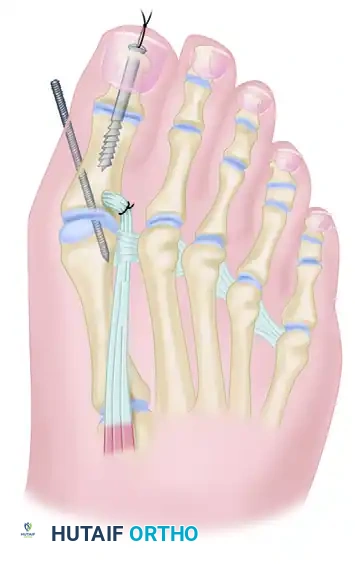
Step 5: EHL Tendon Routing and Transfer
With the IP joint securely fused, attention is turned to the dynamic correction of the MTP joint. The goal is to route the EHL tendon to act as a lateral collateral ligament substitute and a plantarflexor.
- Identify the deep transverse metatarsal ligament in the first web space.
- Pass the mobilized EHL tendon plantar to the deep transverse metatarsal ligament. This critical step changes the vector of the EHL pull from dorsal-medial to plantar-lateral.

- Route the tendon dorsally to the base of the proximal phalanx.
- Prepare a drill hole through the base of the proximal phalanx from lateral to medial. Pass the EHL tendon through this osseous tunnel.
- Apply tension to the EHL tendon while holding the MTP joint in approximately 10 to 15 degrees of extension and neutral coronal alignment (correcting the varus).
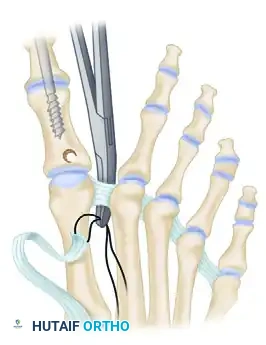
- Suture the tendon back onto itself using non-absorbable braided suture (e.g., #2-0 FiberWire or Ethibond) to secure the transfer under appropriate physiological tension.

Clinical Pearl: The tensioning of the EHL transfer is the most technically demanding aspect of the procedure. Over-tensioning will result in a rigid, plantarflexed MTP joint that causes significant pain during the toe-off phase of gait. Under-tensioning will fail to correct the varus deformity. The toe should rest naturally in neutral alignment without manual support once the tendon is secured.
Step 6: Closure and Radiographic Confirmation
- Deflate the tourniquet and achieve meticulous hemostasis.
- Close the subcutaneous tissues with absorbable sutures and the skin with non-absorbable monofilament.

- Obtain intraoperative fluoroscopy (AP, Lateral, and Oblique views) to confirm the concentric reduction of the MTP joint, the correction of the varus angle, and the optimal placement and compression of the 4.0-mm IP joint screw.

Postoperative Protocol and Rehabilitation
Strict adherence to the postoperative protocol is essential to protect the tendon transfer and ensure bony union of the IP joint.
- Weeks 0-2: The patient is placed in a bulky, sterile compressive dressing and a rigid postoperative shoe or short leg splint. The patient is strictly non-weight-bearing (NWB) on the operative extremity. Elevation is critical to minimize edema and protect the incision.
- Weeks 2-6: Sutures are removed at 14 days, provided the incision is fully healed. The patient is transitioned to a short leg cast or a rigid CAM boot. Weight-bearing is restricted to heel-touch only. The tendon transfer requires a minimum of 6 weeks to achieve initial biologic fixation to the bone.
- Weeks 6-8: Radiographs are obtained to assess the consolidation of the IP joint arthrodesis. If clinical and radiographic signs of union are present, the patient may begin progressive weight-bearing in a stiff-soled shoe.
- Physical Therapy: Gentle, active range of motion of the MTP joint is initiated. Passive stretching into extreme extension is avoided to prevent stretching out the EHL transfer.
Complications and Pitfalls
While highly effective, the Johnson and Spiegl technique carries specific risks that the orthopedic surgeon must anticipate:
- Nonunion of the IP Joint: Occurs in up to 5-10% of cases. Risk factors include inadequate cartilage resection, failure to achieve lag screw compression, and patient non-compliance with weight-bearing restrictions. If asymptomatic, it may be observed; if painful, revision arthrodesis with bone grafting is required.
- Hardware Prominence: The head of the 4.0-mm screw at the distal tip of the phalanx can occasionally cause irritation against closed-toe shoes. If this occurs after solid bony union is achieved (typically >6 months post-op), the screw can be removed in a minor outpatient procedure.
- Recurrent Deformity (Undercorrection): Usually secondary to inadequate mobilization of the EHL, failure to route the tendon deep to the transverse metatarsal ligament, or insufficient tensioning during fixation.
- Overcorrection (Hallux Valgus): Rare, but can occur if the EHL is tensioned excessively or if the medial capsular structures were aggressively released during the index procedure.
- Stiffness: As warned preoperatively, a reduction in MTP joint motion is an expected outcome, not necessarily a complication. However, severe arthrofibrosis can occur if postoperative rehabilitation is delayed.
Conclusion
The transfer of the extensor hallucis longus with concomitant arthrodesis of the interphalangeal joint is a highly reliable, biomechanically sound procedure for the correction of supple hallux varus. By converting the EHL from a deforming dorsal force into a corrective lateral and plantar tether, and by utilizing the FHL to stabilize the MTP joint via IP fusion, the surgeon can restore a functional, plantigrade first ray. Mastery of the Johnson and Spiegl technique, meticulous soft tissue handling, and precise tensioning are the cornerstones of achieving excellent, long-lasting clinical outcomes.
You Might Also Like
