Masterclass in Tibial Plateau Fractures: Surgical Management

Key Takeaway
Tibial plateau fractures represent complex intra-articular injuries demanding meticulous soft-tissue management and precise articular restoration. This guide explores high-energy fracture-dislocations, the Schatzker and Hohl-Moore classifications, and evidence-based surgical techniques. Successful outcomes rely on anatomic joint reduction, stable internal fixation, and early mobilization, mitigating risks of post-traumatic arthritis and joint instability.
Introduction to Tibial Plateau Fractures
Proximal tibial articular fractures, commonly referred to as tibial plateau fractures, represent a heterogeneous group of injuries ranging from subtle, low-energy osteoporotic depressions to devastating, high-energy fracture-dislocations. Because the proximal tibia is a critical weight-bearing axis, any disruption to its articular congruity or ligamentous stability can lead to rapid joint degeneration, post-traumatic osteoarthritis, and profound functional disability.
High-energy mechanisms—such as motor vehicle collisions or pedestrian-versus-auto ("bumper strike") injuries—are frequently associated with severe complications, including compartment syndrome, vascular compromise, deep vein thrombosis (DVT), and extensive soft-tissue crush injuries. Conversely, low-energy mechanisms, such as falls in the elderly population, typically produce isolated depression or split-depression patterns due to underlying osteopenia.
Biomechanics and Mechanism of Injury
The specific fracture pattern sustained is directly dictated by the vector of the applied force, the degree of knee flexion at the time of impact, and the patient's bone quality. Schulak and Gunn extensively mapped the relationship between the type of fracture produced, the frequency of collateral ligament injury, and the specific forces applied to the knee.
Axial loading combined with valgus or varus stress drives the femoral condyles into the tibial plateau like a wedge. Because the lateral plateau is convex and structurally weaker than the concave, denser medial plateau, lateral-sided fractures are significantly more common.
Clinical Pearl: Ligamentous injuries occur more frequently in minimally displaced, local compression, and split-compression fractures. It is imperative to obtain stress radiographs or MRI to evaluate the collateral and cruciate ligaments, as bony stability does not guarantee soft-tissue integrity.
Soft-Tissue Envelope and Complex Knee Trauma
Tscherne and Lobenhoffer revolutionized the understanding of these injuries by emphasizing the critical distinction between "pure" plateau fracture patterns and fracture-dislocation patterns.
In their landmark review of 190 proximal tibial articular fractures, they found:
* Meniscal Injuries: 67% occurred in "pure" plateau fracture patterns.
* Cruciate Ligament Injuries: 96% occurred in fracture-dislocation patterns.
* Medial Collateral Ligament (MCL) Injuries: 85% occurred in fracture-dislocation patterns.
* Peroneal Nerve Injury: Twice as common in fracture-dislocation patterns.
These authors introduced the term complex knee trauma to describe injuries involving significant damage to two or more of the following compartments: the soft-tissue envelope, the ligamentous stabilizers, and the bony structures of the distal femur and proximal tibia.
Surgical Warning: Complex fractures involving both the femoral and tibial articular surfaces carry a 25% incidence of vascular injury and a 25% incidence of compartment syndrome. In severe soft-tissue injuries, vascular injury rates can climb to 31%, compartment syndrome to 31%, and peroneal nerve injury to 23%. A high index of suspicion and serial neurovascular examinations are mandatory.
Comprehensive Classification Systems
Accurate determination of the fracture pattern is the cornerstone of preoperative planning. Two primary classification systems dominate the academic and clinical landscape: the Hohl and Moore classification and the Schatzker classification.
Hohl and Moore Classification (Articular Fractures)
Originally proposed by Hohl and later modified by Moore and Hohl, this system distinguishes between five primary fracture patterns and five fracture-dislocation patterns.
The primary fracture patterns include:
1. Type 1 (Minimally Displaced): Stable injuries often amenable to conservative management.
2. Type 2 (Local Compression): Central articular depression with an intact cortical rim.
3. Type 3 (Split Compression): A lateral wedge split combined with articular depression.
4. Type 4 (Total Condyle): Involves the entire medial or lateral condyle.
5. Type 5 (Bicondylar): Involves both plateaus but maintains metaphyseal-diaphyseal continuity.
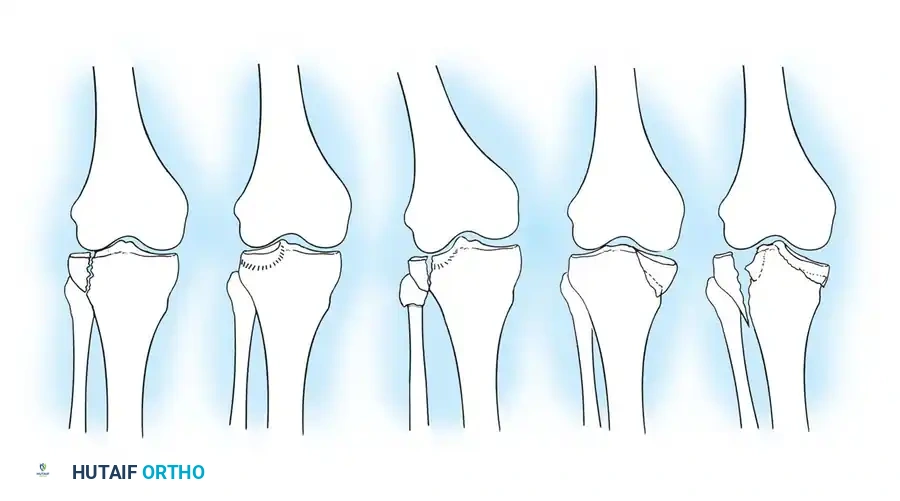
Schatzker Classification System
The Schatzker classification is the most universally utilized system, guiding both prognosis and surgical tactics. It closely mirrors the Hohl and Moore system but adds a critical sixth category for metaphyseal-diaphyseal dissociation.
- Type I (Pure Cleavage): A typical wedge-shaped, uncomminuted fragment is split off and displaced laterally and downward. Common in younger patients with dense bone. If displaced, it is fixed with transverse cancellous lag screws.
- Type II (Cleavage Combined with Depression): A lateral wedge is split off, and the articular surface is driven into the metaphysis. Common in older individuals. If depression exceeds 5–8 mm or instability is present, treatment requires open reduction, elevation of the joint surface, bone grafting of the metaphyseal void, and lateral buttress plating.
- Type III (Pure Central Depression): The articular surface is driven into the plateau with an intact lateral cortex. Occurs almost exclusively in osteoporotic bone. Requires elevation, grafting, and support with a raft of screws or a buttress plate.
- Type IV (Medial Condyle Fracture): A high-energy injury that may split as a single wedge or present with comminution and depression. The tibial spines are often involved. These tend to angulate into varus and require robust medial buttress plating. Always rule out a knee dislocation.
- Type V (Bicondylar Fracture): Both tibial plateaus are fractured, but the metaphysis and diaphysis retain continuity. Requires bilateral stabilization, often utilizing a lateral locking plate and a medial anti-glide plate.
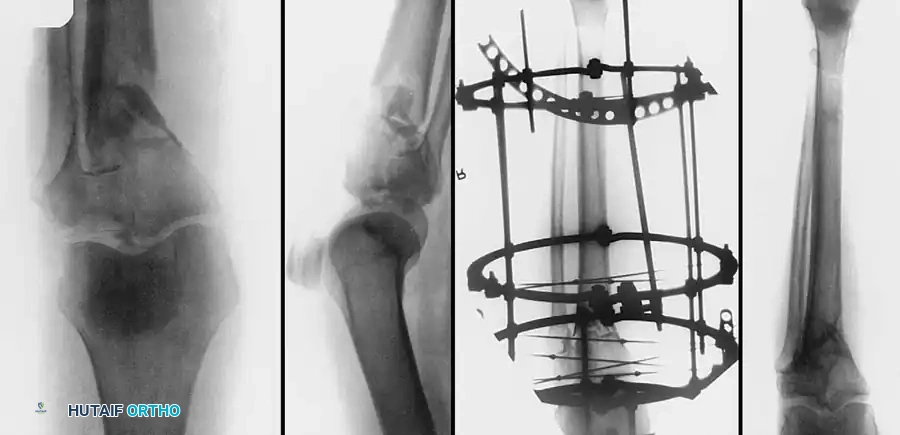
- Type VI (Metaphyseal-Diaphyseal Dissociation): A transverse or oblique fracture separates the articular/metaphyseal segment from the tibial shaft. Highly unstable and unsuitable for traction. Requires dual plating or fine-wire external fixation.
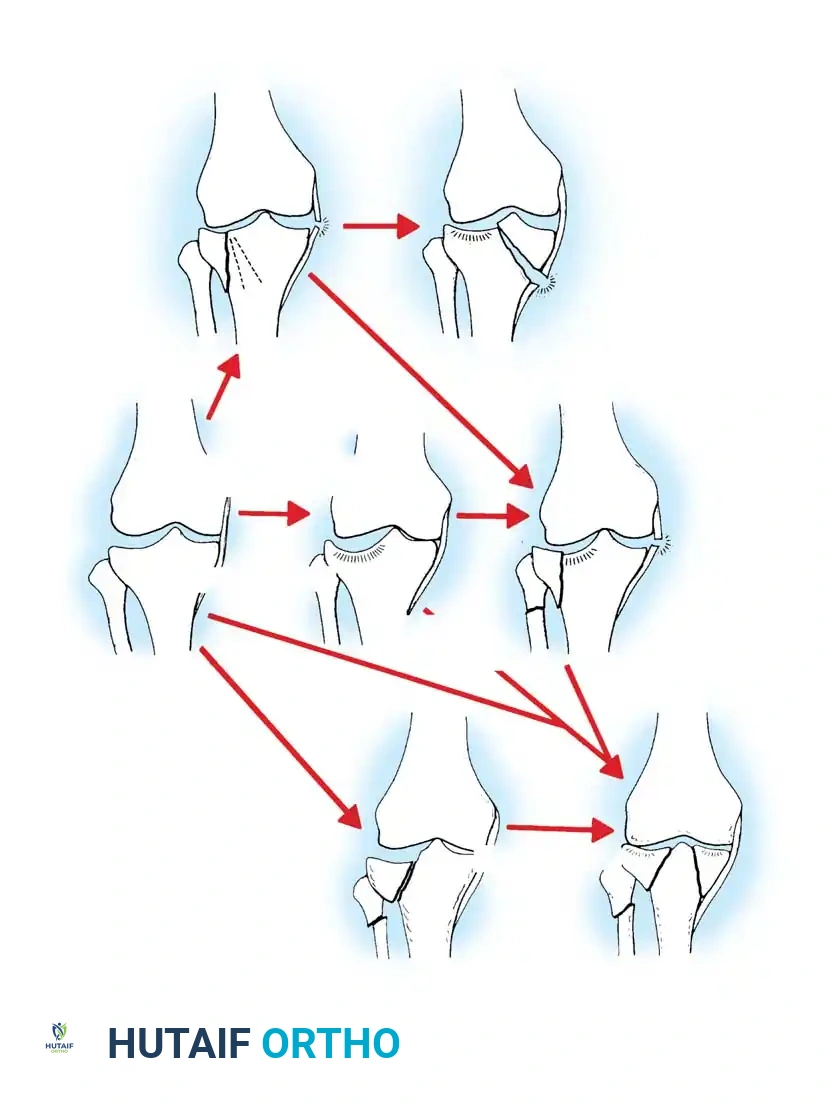
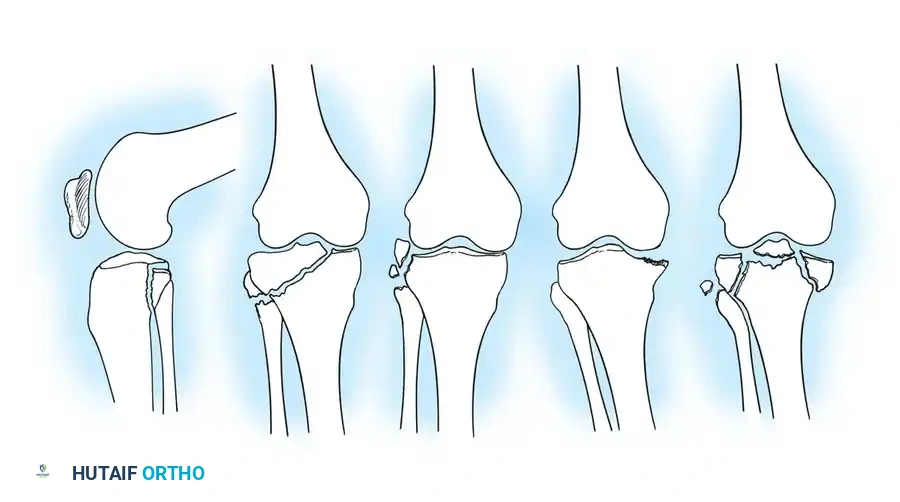
Hohl and Moore Fracture-Dislocation Patterns
Fracture-dislocations occur roughly one-seventh as frequently as pure fractures but carry a dramatically higher morbidity profile, including irreparable meniscal tears and a 15% overall rate of neurovascular injury.
- Type I (Coronal Split): Accounts for 37% of fracture-dislocations. The fracture line runs at 45 degrees to the medial plateau in an oblique coronal-transverse plane. Often associated with avulsions of the fibular styloid or Gerdy's tubercle.
- Type II (Entire Condyle): Distinguished by a fracture line extending into the opposite compartment beneath the intercondylar eminence. The opposite collateral ligament is involved in 50% of cases.

- Type III (Rim Avulsion): Involves the lateral plateau with avulsion of the capsular attachment. Disruption of cruciate ligaments is common. Neurovascular injuries occur in 30% of these cases.
- Type IV (Rim Compression): The tibia subluxates, allowing the femoral condyle to compress the anterior, posterior, or middle articular rim. Almost always unstable.
- Type V (Four-Part Fracture): A devastating injury with a 50% rate of neurovascular compromise. Both collateral ligaments are disrupted, and the intercondylar eminence is a separate fragment, resulting in total loss of cruciate stability.
Preoperative Evaluation and Damage Control
Initial management prioritizes the soft-tissue envelope. In high-energy Type V and VI fractures, immediate open reduction and internal fixation (ORIF) through compromised soft tissues carries an unacceptable risk of wound dehiscence and deep infection (historically up to 82% in early dual-plating series).
Damage Control Orthopedics (DCO):
For severe swelling, fracture blisters, or polytrauma, a knee-spanning external fixator is applied immediately. This restores length, alignment, and rotation while allowing the soft tissues to recover over 10 to 21 days.
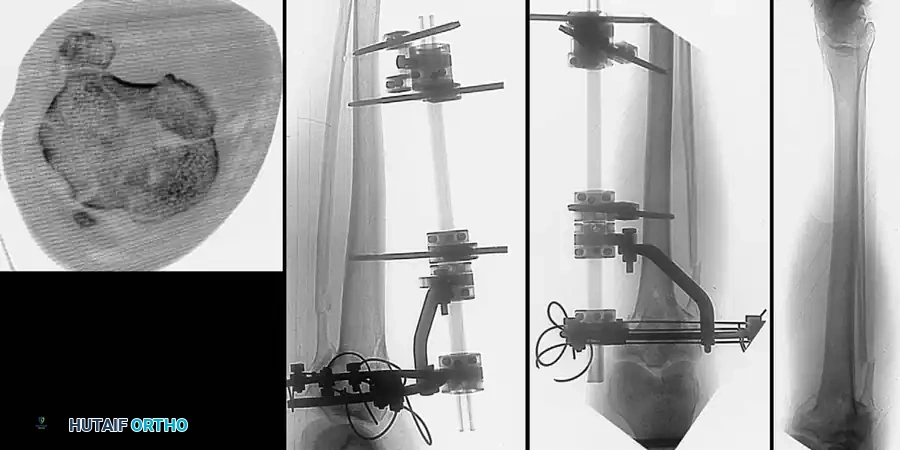
Advanced imaging is mandatory. A fine-cut CT scan with 2D and 3D reconstructions is the gold standard for mapping articular comminution, identifying coronal plane fractures (e.g., posterior medial shear fragments), and planning surgical approaches.
Surgical Approaches
The choice of surgical approach is dictated by the fracture morphology identified on the CT scan.
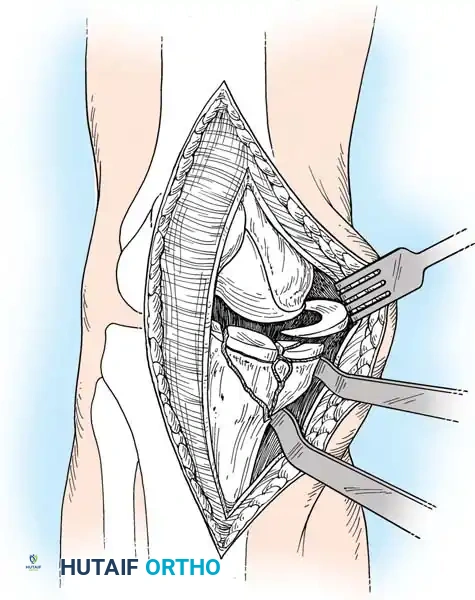
Anterolateral Approach
Utilized for Schatzker I, II, and III fractures.
1. An incision is made from the lateral femoral condyle, extending distally over Gerdy's tubercle.
2. The iliotibial band is incised, and the origin of the extensor digitorum longus is elevated off the proximal tibia.
3. A submeniscal arthrotomy is performed. The anterior horn of the lateral meniscus is tagged with a non-absorbable suture and elevated to visualize the articular surface directly.
Posteromedial Approach
Essential for Schatzker IV fractures and the medial component of Schatzker V/VI fractures.
1. The patient is positioned supine with a bump under the contralateral hip, allowing external rotation of the operative leg.
2. An incision is made along the posteromedial border of the tibia.
3. The pes anserinus is retracted anteriorly, and the medial head of the gastrocnemius is retracted posteriorly, exposing the posteromedial crest of the tibia.
Step-by-Step Operative Technique
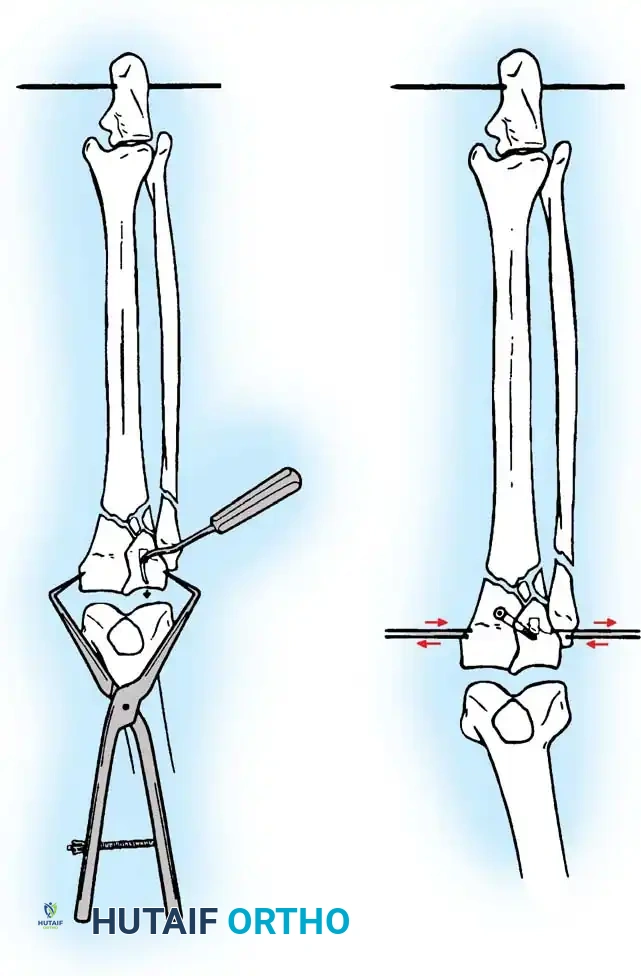
1. Articular Reduction and Elevation
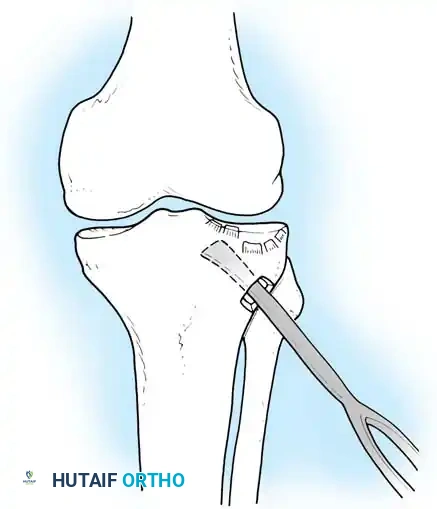
For depressed fractures (Schatzker II and III), the articular surface must be elevated anatomically.
* A cortical window is created in the anterolateral metaphysis distal to the fracture.
* A bone tamp is introduced through the window, and the depressed articular fragments are gently elevated "en masse" under direct vision and fluoroscopic guidance.
2. Bone Grafting and Defect Management
Elevation of the articular surface leaves a significant metaphyseal void. If left unfilled, the articular surface will inevitably subside under physiological loading.
* The void is packed tightly with autograft (iliac crest), allograft (cancellous chips), or osteoconductive calcium phosphate cement. Calcium phosphate provides excellent compressive strength and immediate structural support.
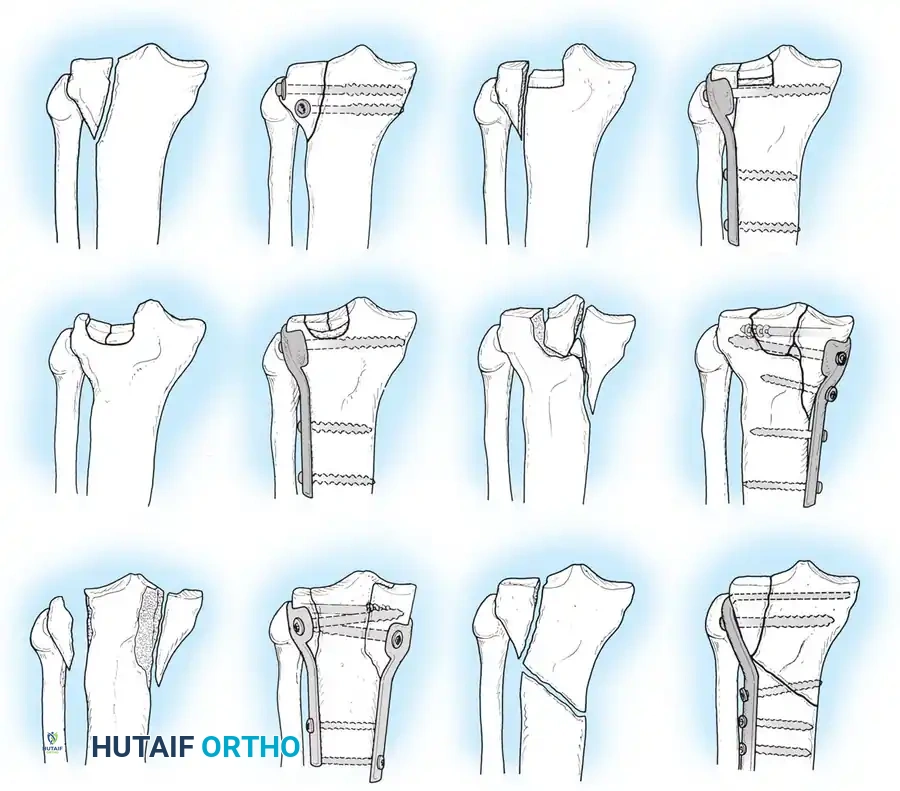
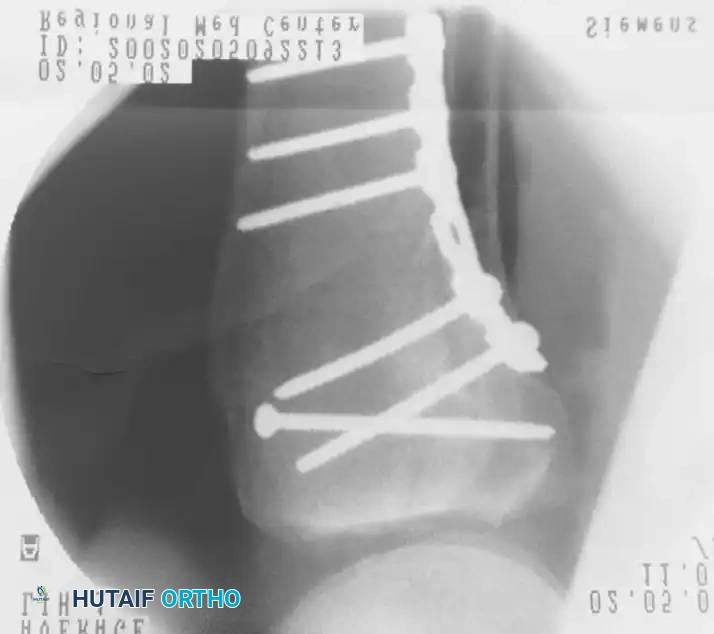
3. Internal Fixation Strategies
Once the articular surface is reduced and grafted, it is provisionally held with K-wires. Definitive fixation relies on the principles of absolute stability for the articular surface and relative stability for the metaphyseal-diaphyseal component.
- Lag Screws: Subchondral 6.5mm or 7.3mm cancellous screws are placed parallel to the joint line to compress the split fragments.
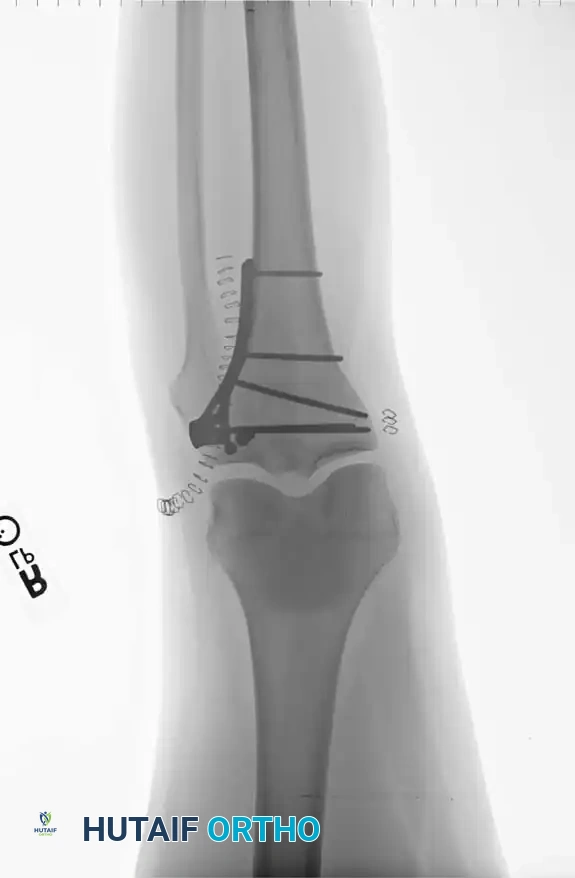
- Buttress Plating: A pre-contoured proximal tibial locking plate is applied to neutralize axial and shearing forces.
For bicondylar fractures (Schatzker V and VI), dual plating is often required. The more comminuted condyle is stabilized with a robust locking plate, while the less involved condyle is supported with a smaller anti-glide plate to prevent varus/valgus collapse.
Intraoperative fluoroscopy must confirm anatomic joint reduction, restoration of the mechanical axis, and appropriate hardware placement without intra-articular penetration.

Postoperative Protocol and Rehabilitation
The ultimate goal of tibial plateau fracture management is a stable, painless, and mobile knee. Postoperative care must balance the need for early range of motion (to nourish the articular cartilage and prevent arthrofibrosis) with the necessity of protecting the fracture fixation.
-
Immediate Postoperative Phase (0-2 Weeks):
- The knee is placed in a hinged knee brace locked in extension for weight-bearing transfers only.
- Strict non-weight-bearing (NWB) status is maintained on the operative extremity.
- Continuous Passive Motion (CPM) or active-assisted range of motion (AAROM) is initiated immediately, aiming for 0 to 90 degrees of flexion.
-
Intermediate Phase (2-6 Weeks):
- Sutures are removed at 14 days.
- ROM is progressed to full flexion as tolerated.
- NWB status is strictly maintained. Radiographs are obtained at 2 and 6 weeks to monitor for subsidence or hardware failure.
- Late Phase (6-12 Weeks):
- At 8 to 10 weeks, if radiographic evidence of callus formation and clinical stability are present, progressive partial weight-bearing (PWB) is initiated (e.g., 25% body weight increments per week).
- Full weight-bearing is typically achieved by 12 weeks.
- Strengthening focuses on the quadriceps and hamstrings to provide dynamic stability to the knee joint.
Pitfall: Premature weight-bearing is the leading cause of articular subsidence and hardware failure in osteoporotic patients. Always err on the side of caution and delay weight-bearing until definitive radiographic union is visible.
By adhering to strict biomechanical principles, respecting the soft-tissue envelope, and executing precise articular reductions, orthopedic surgeons can mitigate the devastating complications of tibial plateau fractures and restore optimal function to the traumatized knee.
📚 Medical References
- tibial plateau fractures, Clin Orthop Relat Res 240:53, 1989.
- Buck BE, Malinin TE, Brown MD: Bone transplantation and human immunodefi ciency virus: an estimate of risk of acquired immunodeficiency syndrome (AIDS), Clin Orthop Relat Res 240:129, 1989.
- Buck BE, Malinin TI: Human bone and tissue allografts, Clin Orthop Relat Res 303:8, 1994.
- Bunnell S, ed: Surgery of the hand, 2nd ed, Philadelphia, 1948, JB Lippincott. Burchardt H: Biology of bone transplantation, Orthop Clin North Am 18:198, 1987.
- Campbell WC: Ununited fractures, Arch Surg 8:782, 1924.
- Chapman MW, Bucholz R, Cornell CN: Treatment of acute fractures with a collagen calcium phosphate graft material: a randomized clinical trial, J Bone Joint Surg 79A:495, 1997.
- Cobden RH, Thrasher EL, Harris WH: Topical hemostatic agents to reduce bleeding from cancellous bone, J Bone Joint Surg 58A:70, 1976.
- Cole WH: The treatment of claw-foot, J Bone Joint Surg 22:895, 1940.
- Colterjohn NR, Bednar DA: Procurement of bone graft from the iliac crest, J Bone Joint Surg 79A:756, 1997.
- Connolly J, Guse R, Lippiello L, et al: Development of an osteogenic bone-marrow preparation, J Bone Joint Surg 71A:684, 1989.
- Cornell CN: Initial clinical experience with use of Collagraft as a bone graft substitute, Tech Orthop 7:55, 1992.
- Coventry MB, Tapper EM: Pelvic instability: a consequence of removing iliac bone for grafting, J Bone Joint Surg 54A:83, 1972.
- Crenshaw AG, Hargens AR, Gershuni DH, et al: Wide tourniquet cuffs more effective at lower infl ation pressures, Acta Orthop Scand 59:447, 1988.
- Dirschl DR, Wilson FC: Topical antibiotic irrigation in the prophylaxis of operative wound infections in orthopedic surgery, Orthop Clin North Am 22:419, 1991.
- Dobner JJ, Nitz AJ: Postmeniscectomy tourniquet palsy and functional sequelae, Am J Sports Med 10:211, 1982.
- Doppelt SH, Tomford WW, Lucas AD, et al: Operational and financial aspects of a hospital bone bank, J Bone Joint Surg 63A:1472, 1981.
- Enneking WF, Mindell ER: Observations on massive retrieved human allografts, J Bone Joint Surg 73A:1123, 1991.
- Estrera AS, King RP, Platt MR: Massive pulmonary embolism: a complication of the technique of tourniquet ischemia, J Trauma 22:60, 1982.
- Fahmy NR, Patel DG: Hemostatic changes and postoperative deep-vein thrombosis associated with the use of a pneumatic tourniquet, J Bone Joint Surg 63A:461, 1981.
- Flynn JM, Springfi eld DS, Mankin HJ: Osteoarticular allografts to treat distal femoral
