Minimally Invasive Anterolateral Approach for Proximal Tibia Fractures: Perfecting Soft Tissue Preservation
Key Takeaway
The minimally invasive anterolateral approach for proximal tibia fractures preserves soft tissue integrity through precise incision placement and meticulous handling. It aims to enhance vascularity, reduce infection, and expedite recovery by achieving stable fixation while minimizing risks to critical neurovascular structures like the common peroneal nerve. This optimizes patient outcomes and reduces surgical morbidity.
Introduction and Epidemiology
Proximal tibia fractures represent a significant portion of lower extremity trauma, exhibiting a classic bimodal distribution. High-energy mechanisms, such as motor vehicle collisions or falls from height, typically cause complex, comminuted injuries in younger demographics. Conversely, low-energy falls frequently result in split-depression or pure depression fractures in osteoporotic older adults. The complex anatomy of the proximal tibia, characterized by its load-bearing capacity, articulation with the femur and fibula, and proximity to critical neurovascular structures, renders these injuries challenging to manage. While traditional extensive open approaches offer direct articular visualization, they are historically associated with significant soft tissue dissection, devascularization of metaphyseal bone fragments, elevated rates of wound necrosis, deep infection, and delayed union.
The evolution of surgical techniques has driven a paradigm shift toward Minimally Invasive Plate Osteosynthesis for metaphyseal and select articular fractures of the proximal tibia. These approaches prioritize the preservation of the soft tissue envelope, maintenance of the fracture hematoma, and protection of the periosteal blood supply. The anterolateral approach remains the workhorse for accessing the lateral tibial plateau and proximal metaphysis. It is highly efficacious for fractures that do not overtly involve the posterior joint surface, or where the intra-articular component can be reduced and stabilized indirectly or via limited submeniscal arthrotomy.
The concept of perfecting the line of the skin in minimally invasive proximal tibia surgery transcends mere cosmesis. It embodies a meticulous understanding of underlying angiosomes, fracture mechanics, and soft tissue biology. Precise incision placement, the avoidance of excessive retraction, and judicious tissue handling are paramount to minimizing soft tissue compromise. This comprehensive surgical reference details the critical aspects of the minimally invasive anterolateral approach, emphasizing strategies for achieving stable anatomical reduction while mitigating surgical morbidity.
Surgical Anatomy and Biomechanics
A thorough understanding of regional osteology, myology, and neurovascular topography is indispensable for the safe application of minimally invasive techniques to the proximal tibia.
Bony Anatomy
The proximal tibia consists of the medial and lateral condyles, the tibial plateau, the tibial tuberosity, and the proximal metaphysis. The lateral plateau is convex in the sagittal plane and extends further proximally than the concave medial plateau. The lateral condyle is structurally less robust, possessing thinner subchondral bone, making it highly susceptible to shear and depression forces. The anterolateral surface of the proximal tibia, specifically Gerdy's tubercle, serves as the primary insertion site for the iliotibial band and acts as a crucial bony landmark for surgical incisions.
Soft Tissue Anatomy and Angiosomes
The skin and subcutaneous tissue overlying the anterolateral aspect of the proximal tibia are thin and vulnerable to shearing trauma. The blood supply to this region is predicated on a delicate network derived from the anterior tibial recurrent artery, the inferior lateral genicular artery, and perforators from the anterior tibial artery. Surgical incisions must respect these angiosomes. Broad stripping of the periosteum disrupts the centrifugal blood supply to the tibial cortex, increasing the risk of nonunion and osteomyelitis. Minimally invasive techniques rely on preserving this fascial and periosteal vascularity by creating submuscular, extra-periosteal tunnels.
Musculature and Fascial Compartments
The anterolateral compartment of the leg contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and fibularis tertius muscles. The fascial envelope enclosing this compartment is unyielding, rendering it highly susceptible to acute compartment syndrome following high-energy trauma or fluid extravasation during arthroscopically assisted reduction. The tibialis anterior muscle originates from the lateral condyle and the proximal two-thirds of the lateral tibial diaphysis. Its robust anterior belly serves as a primary barrier to direct diaphyseal access, necessitating careful submuscular elevation during plate insertion.
Neurovascular Structures
The most critical neurovascular structures at risk during an anterolateral approach to the proximal tibia include the common peroneal nerve and the anterior tibial artery. The common peroneal nerve courses posterolaterally around the fibular neck before bifurcating into the deep and superficial peroneal nerves within the substance of the peroneus longus muscle. While typically safe during standard proximal anterolateral incisions, distal extension or percutaneous screw placement in the proximal third of the leg places this nerve at risk. The anterior tibial artery passes anteriorly through the proximal interosseous membrane. Plating techniques that involve excessive posterior retraction or drills plunging through the posterior cortex risk catastrophic injury to this vessel.
Indications and Contraindications
The minimally invasive anterolateral approach is highly versatile but requires careful patient selection based on fracture morphology and soft tissue status. It is primarily indicated for lateral plateau fractures and proximal metaphyseal fractures where the medial column remains intact or can be stabilized independently.
Operative Indications
Ideal candidates for this approach include patients with Schatzker Type I, II, and III fractures, as well as select Type V and VI fractures when combined with a separate posteromedial approach. Extra-articular proximal tibial metaphyseal fractures (AO/OTA 41-A2, A3) are also prime indications for submuscular anterolateral plating.
Contraindications
Absolute contraindications include active infection at the surgical site and severe, unresuscitative soft tissue compromise (e.g., Tscherne Grade 3 closed injuries with severe blistering, or open fractures requiring extensive serial debridement). In such scenarios, temporary joint-spanning external fixation is mandated until the soft tissue envelope recovers. Relative contraindications include highly comminuted posterior shear fractures that cannot be visualized or reduced from an anterior trajectory, necessitating a dedicated posterolateral or direct posterior approach.
| Parameter | Operative Indications | Non Operative Indications |
|---|---|---|
| Articular Step Off | > 2 mm to 3 mm depression or step-off | < 2 mm step-off, anatomically aligned |
| Condylar Widening | > 5 mm of condylar widening | Minimal widening, contained fragment |
| Instability | Varus or valgus instability > 10 degrees | Stable joint under varus/valgus stress |
| Fracture Pattern | Schatzker I through VI (with caveats) | Non-displaced Schatzker I or IV |
| Patient Factors | Ambulatory, medically optimized | Non-ambulatory, severe comorbidities |
| Soft Tissue Status | Resolved swelling, positive wrinkle sign | Severe blistering (delay surgery) |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful minimally invasive osteosynthesis. The inability to directly visualize the entire fracture necessitates a comprehensive understanding of the fracture geometry derived from advanced imaging.
Imaging and Templating
Standard orthogonal radiographs (Anteroposterior and Lateral) of the knee and full-length tibia are mandatory. A fine-cut Computed Tomography scan with 2D multiplanar and 3D reconstructions is critical for articular mapping. The CT scan allows the surgeon to identify the primary fracture lines, the location of articular depression, and the presence of posterior coronal plane fragments. Preoperative digital templating is utilized to determine the appropriate plate length, the required number of metaphyseal locking screws, and the trajectory of subchondral raft screws to support elevated articular segments.
Positioning and Fluoroscopy
The patient is positioned supine on a radiolucent operating table. A bump is placed beneath the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring the patella faces directly anteriorly. This facilitates true AP and lateral fluoroscopic imaging. A sterile tourniquet may be applied to the proximal thigh, though its routine use is debated due to the potential for exacerbating ischemic injury to compromised soft tissues. The fluoroscopy C-arm is brought in from the contralateral side. The surgeon must verify that perfect AP and lateral views of the proximal tibia can be obtained without obstruction before prepping and draping.
Detailed Surgical Approach and Technique
The minimally invasive anterolateral approach is executed in a stepwise fashion, prioritizing the preservation of the periosteal blood supply and the overlying skin.
Incision Placement and Soft Tissue Handling
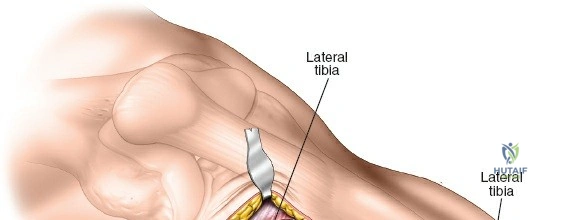
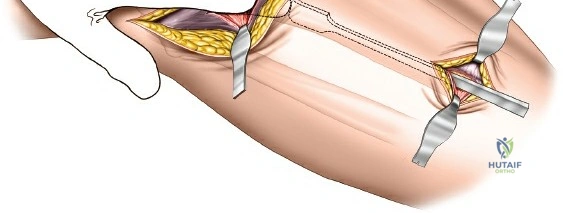
To perfect the line of the skin, the primary incision must be meticulously planned. An S-shaped or gentle hockey-stick incision is typically utilized, beginning 2 to 3 centimeters proximal to Gerdy's tubercle, curving distally along the lateral border of the tibial tuberosity, and extending approximately 3 to 5 centimeters along the anterior crest of the tibia. This incision allows access to the lateral plateau for articular reduction while maintaining a robust full-thickness skin flap.
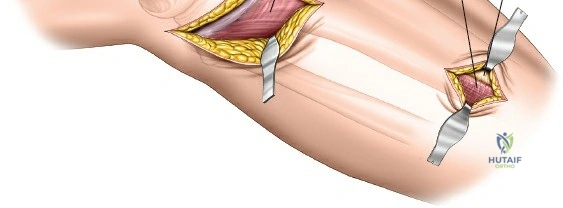
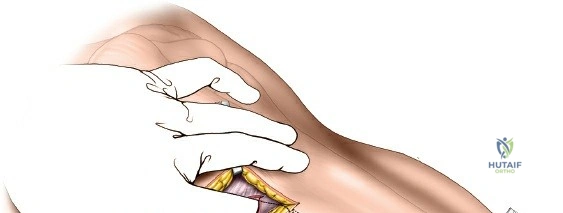
Subcutaneous dissection is kept to an absolute minimum. Full-thickness fasciocutaneous flaps are elevated to expose the iliotibial band and the fascia over the anterior compartment. Retractors must be placed with care; excessive traction on the skin edges is a primary cause of postoperative wound edge necrosis.
Deep Dissection and Submuscular Tunneling
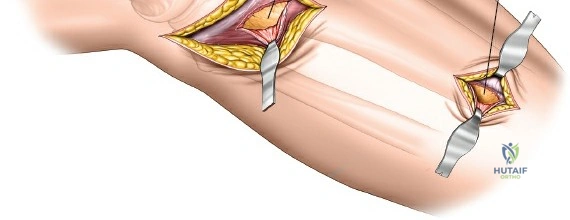
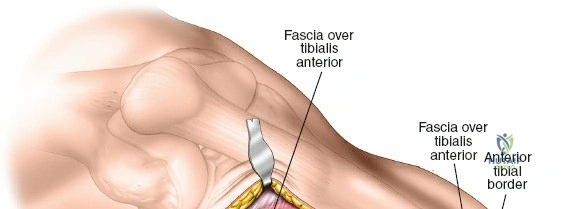
A submeniscal arthrotomy is performed by incising the coronary ligament, allowing the lateral meniscus to be elevated with a suture to visualize the articular surface. For the metaphyseal and diaphyseal extension, the fascia over the tibialis anterior is incised longitudinally, approximately 1 centimeter lateral to the tibial crest.
Using a Cobb elevator or a specialized tunneling periosteal elevator, a submuscular, extra-periosteal plane is bluntly created between the deep surface of the tibialis anterior muscle and the lateral surface of the tibia. This tunnel must be strictly extra-periosteal to preserve the cortical blood supply. The elevator is advanced distally to accommodate the pre-templated length of the locking compression plate.
Fracture Reduction Strategies
In minimally invasive surgery, reduction precedes fixation and must be achieved indirectly or via limited direct manipulation.
For articular depression (Schatzker II or III), a cortical window is created in the anterolateral metaphysis. A bone tamp is introduced through this window to elevate the depressed articular fragments under direct visual and fluoroscopic guidance. Once the articular surface is restored, the metaphyseal void is filled with autograft, allograft, or bone substitute to support the reduction.
For metaphyseal dissociation or malalignment, indirect reduction techniques are employed. A femoral distractor or external fixator can be applied to restore length and mechanical axis. Percutaneous point-reduction clamps, Schanz pins used as joysticks, and strategic bump placement under the fracture apex are highly effective for correcting varus, valgus, and translational deformities. Fluoroscopy is utilized extensively to confirm the restoration of the medial and lateral cortices and the overall mechanical axis.
Plate Application and Fixation
An anatomically pre-contoured proximal lateral tibia locking plate is introduced through the proximal incision and slid distally along the prepared submuscular tunnel. The plate must sit flush against the lateral cortex. If the plate is prominent or stands off the bone distally, it will create undue tension on the skin, leading to delayed necrosis.
Initial fixation is typically achieved with a standard non-locking cortical screw in the diaphyseal segment to pull the plate to the bone, followed by a proximal non-locking screw or K-wires to secure the plate to the lateral condyle. Once the plate is appropriately positioned and the fracture is reduced, subchondral locking screws (raft screws) are placed proximally to support the articular surface. Distal fixation is completed using percutaneous stab incisions, taking care to spread the soft tissues longitudinally down to the plate to avoid injuring branches of the superficial peroneal nerve. A combination of locking and non-locking screws is used depending on bone quality and the need for dynamic compression.
Complications and Management
Despite the advantages of minimally invasive techniques, complications can still occur. Anticipation, early recognition, and aggressive management are essential.
Acute Compartment Syndrome
The proximal tibia is a classic location for acute compartment syndrome, particularly following high-energy trauma. The risk is not entirely eliminated by minimally invasive plating; in fact, bleeding from the fracture site contained by a tightly closed fascia can precipitate it. Continuous clinical monitoring is required. If compartment syndrome is suspected, immediate four-compartment fasciotomy is mandatory.
Soft Tissue Necrosis and Infection
Wound dehiscence and deep infection remain significant concerns. Minimizing retraction time, keeping tissues moist, and ensuring tension-free closure are critical preventative measures. If superficial necrosis occurs, it can often be managed with local wound care and oral antibiotics. Deep infections involving the hardware require aggressive surgical debridement, targeted intravenous antibiotics, and potentially hardware removal if union has been achieved or if the infection cannot be suppressed.
Hardware Prominence and Nerve Irritation
The anterolateral tibia has minimal soft tissue coverage. Prominent hardware, particularly proximally at Gerdy's tubercle or distally along the tibial crest, can cause localized pain and skin irritation. Symptomatic hardware may necessitate removal after complete radiographic and clinical union, typically no earlier than 12 to 18 months postoperatively. Iatrogenic injury to the superficial peroneal nerve during distal percutaneous screw placement can result in paresthesias or painful neuromas.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Compartment Syndrome | 5% to 10% | Avoid fluid extravasation; emergent 4-compartment fasciotomy. |
| Deep Surgical Site Infection | 3% to 8% | Delay surgery until soft tissue recovers; aggressive serial debridement, IV antibiotics, flap coverage if needed. |
| Wound Edge Necrosis | 5% to 15% | Avoid excessive retraction, tension-free closure; local wound care, negative pressure wound therapy. |
| Nonunion / Delayed Union | 2% to 5% | Preserve periosteal blood supply, avoid over-distraction; bone grafting, revision fixation, or dynamization. |
| Loss of Reduction / Varus Collapse | 3% to 7% | Utilize rigid locking constructs, adequate subchondral rafting; revision osteotomy and re-plating. |
| Common Peroneal Nerve Palsy | 1% to 3% | Avoid aggressive posterior retraction; ankle-foot orthosis (AFO), nerve exploration if no recovery at 3-6 months. |
Post Operative Rehabilitation Protocols
Rehabilitation following minimally invasive anterolateral plating of the proximal tibia is phased, balancing the need for early joint mobilization with the mechanical requirements of fracture healing.
Phase I Early Mobilization
The immediate postoperative phase (0 to 6 weeks) focuses on edema control, wound healing, and the restoration of knee range of motion. Continuous Passive Motion machines or early active-assisted range of motion exercises are initiated immediately to prevent arthrofibrosis. Weight-bearing is strictly limited to non-weight-bearing or toe-touch weight-bearing (up to 20 pounds) to protect the articular reduction and the hardware construct from shear forces.
Phase II Progressive Weight Bearing
Between 6 and 12 weeks, clinical and radiographic assessments dictate the progression of weight-bearing. Once bridging callus is evident on orthogonal radiographs and the patient exhibits minimal pain at the fracture site, partial weight-bearing is initiated. This is progressively advanced over several weeks. Strengthening exercises for the quadriceps, hamstrings, and hip abductors are intensified to restore dynamic joint stability.
Phase III Full Function
Beyond 12 weeks, assuming radiographic union is progressing satisfactorily, patients are transitioned to full weight-bearing without assistive devices. Advanced proprioceptive training, agility drills, and work-specific or sport-specific conditioning are introduced. Maximum medical improvement and final functional recovery may take up to 12 to 18 months, and patients must be counseled accordingly.
Summary of Key Literature and Guidelines
The evolution of the minimally invasive anterolateral approach is heavily supported by biomechanical and clinical literature. Foundational studies by the AO Foundation and the Orthopaedic Trauma Association have established the superiority of locking plate technology in osteoporotic bone and comminuted metaphyseal segments.
Clinical series have consistently demonstrated that Minimally Invasive Plate Osteosynthesis reduces the incidence of deep infection and soft tissue complications compared to traditional extensile open approaches. Research focusing on the vascularity of the tibia has highlighted the critical importance of extra-periosteal tunneling to preserve the centrifugal blood flow to the cortex, significantly lowering nonunion rates.
Furthermore, anatomical studies detailing the "safe zones" for percutaneous screw placement in the distal segment of the anterolateral plate have provided critical guidelines for avoiding the superficial peroneal nerve and the anterior tibial artery. Adherence to these evidence-based principles—meticulous preoperative planning, respect for soft tissue biology, indirect reduction techniques, and stable biological fixation—ensures the highest probability of successful outcomes in the management of complex proximal tibia fractures.
