Lateral Tibial Plateau Fractures: Diagnosis, Treatment & Recovery

Key Takeaway
For anyone wondering about Lateral Tibial Plateau Fractures: Diagnosis, Treatment & Recovery, Plateau fractures lateral are intra-articular breaks in the tibial bone, specifically affecting the outer side. These fractures are common due to the lateral plateau's relatively softer subchondral bone and the knee's valgus axis. Direct trauma inducing a valgus force often drives the lateral femoral condyle into the soft lateral tibial plateau, causing this injury.
Introduction and Epidemiology
Lateral tibial plateau fractures represent a complex cohort of intra-articular injuries that fundamentally disrupt the load-bearing mechanics of the lower extremity. These fractures involve the articular surface of the proximal tibia and frequently result in malalignment of the joint surface, predisposing the joint to mechanical instability and subsequent posttraumatic osteoarthritis. As intra-articular fractures, the primary objective of intervention is the restoration of articular congruity, axial alignment, and joint stability.

The epidemiology of lateral tibial plateau fractures demonstrates a classic bimodal distribution, reflecting distinct pathogenetic mechanisms based on patient age and bone density. Split or wedge fractures (Schatzker Type I) predominantly occur in younger patients subjected to high-energy trauma, such as motor vehicle collisions or falls from height. In these scenarios, the subchondral bone is dense and resists compression, resulting in sheer failure and a wedge-shaped fracture fragment. Conversely, pure depression fractures (Schatzker Type II and III) occur more frequently in older patients with osteoporotic bone. The reduced trabecular density in this demographic renders the subchondral bone less able to withstand axial compression, leading to central or peripheral articular impaction without gross cortical splitting.
The pathogenesis of these fractures is intimately linked to the mechanism of injury. Several anatomic factors contribute to the higher incidence of lateral as opposed to medial plateau fractures. The relative softness of the subchondral bone of the lateral plateau, the physiologic valgus axis of the lower extremity, and the susceptibility of the leg to a medially directed force all lead to a prevalence of lateral plateau fractures in low-energy injuries. The most frequent mechanism causing a lateral plateau fracture is a direct trauma to the proximal tibia and knee joint. This induces a valgus force and drives the lateral femoral condyle into the softer lateral tibial plateau. Indirect axial forces often develop in high-energy injuries and may be associated with complex bicondylar or highly comminuted tibial plateau fractures. Twisting injuries account for only five to ten percent of tibial plateau fractures and are most commonly associated with sports injuries, such as alpine skiing.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous and soft tissue anatomy of the proximal tibia is requisite for precise preoperative planning and execution of surgical approaches. The tibial plateau consists of three primary osseous structures including the lateral plateau, the medial plateau, and the intercondylar eminence.
Osseous Architecture
The lateral plateau is smaller, narrower, and convex in the sagittal plane, whereas the medial plateau is larger, broader, and slightly concave. Both plateaus are covered by a meniscus, which serves as a critical shock absorber, distributes load, and improves the congruency of the femorotibial joint. The lateral plateau sits slightly higher than the medial joint surface, forming an angle of three degrees of varus with respect to the mechanical axis of the tibial shaft. This specific osseous geometry is helpful in identifying the lateral plateau on the lateral radiograph during fluoroscopic evaluation.

The intermediate, nonarticular intercondylar eminence serves as the tibial attachment footprint for the anterior and posterior cruciate ligaments. Anteriorly, the tibial tuberosity and the tubercle of Gerdy are prominent bony landmarks located in the subcondylar region. The tibial tuberosity serves as the insertion site for the patellar tendon, while Gerdy's tubercle, situated anterolaterally, is the insertion site for the iliotibial tract. These landmarks are critical for planning surgical incisions and determining the trajectory of periarticular hardware.
Biomechanics and Load Distribution
The anatomy of the tibial plateau leads to an eccentric load distribution in which the lateral plateau bears approximately forty percent of the knee’s axial load during normal bipedal ambulation. This asymmetric weight-bearing results in increased medial subchondral bone formation and a stronger, denser medial plateau over time. Consequently, the lateral plateau is more susceptible to depression from the lateral femoral condyle under valgus stress.

The stability of the knee joint is predicated on the integrity of the cruciate ligaments, the collateral ligaments, the menisci, and the joint capsule. Meniscal injuries have been reported in up to fifty percent of tibial plateau fractures, particularly lateral meniscus tears associated with Schatzker II fractures. Meniscal injuries are a major determinant of prognosis because meniscal integrity is paramount for joint stability and hoop stress distribution, which may partially compensate for minor articular incongruity.
Indications and Contraindications
The natural history of lateral tibial plateau fractures depends heavily on the degree of articular depression, axial alignment, and coronal or sagittal knee stability. Knee instability may result from the fracture itself, particularly if the condylar width is expanded, but may also result from accompanying soft tissue injuries like meniscal incarcerations or rupture of the cruciate or collateral ligaments. For nondisplaced or minimally displaced fractures, the prognosis with non-operative management is generally favorable. However, displaced fractures, especially in combination with knee instability, inevitably tend to result in early posttraumatic arthritis if left untreated.

The physical examination should always include a thorough assessment of the soft tissue envelope. The marginal soft tissue envelope of the proximal tibia predisposes to open fractures and the development of severe tissue necrosis. It is imperative to assess severe soft tissue injury because profound swelling, fracture blisters, or impending compartment syndrome may preclude primary plating of the fracture, necessitating temporizing external fixation.

| Management Strategy | Indications | Contraindications |
|---|---|---|
| Non-Operative Management | Nondisplaced or incomplete fractures; < 2-3 mm articular depression; Stable knee in full extension and 20° flexion; Non-ambulatory patient; Severe medical comorbidities precluding anesthesia. | Open fractures; Acute compartment syndrome; Vascular compromise; Displaced fractures with instability; Associated ligamentous avulsions requiring repair. |
| Temporizing External Fixation | Severe soft tissue compromise (Tscherne II/III); Fracture blisters; Polytrauma requiring damage control orthopedics; Highly comminuted fractures with significant shortening. | Definitive fixation is feasible and safe; Uncompromised soft tissue envelope. |
| Open Reduction Internal Fixation | Articular step-off > 3 mm (relative, debated up to 5 mm in older patients); Condylar widening > 5 mm; Coronal plane instability > 10 degrees; Open fractures (after debridement). | Active local infection; Unresolved severe soft tissue swelling; Medically unstable patient. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for the successful execution of lateral tibial plateau fracture fixation. Standard radiographic evaluation must include an anteroposterior, lateral, and bilateral oblique views of the knee. The plateau typically features a posterior slope of 10 degrees; therefore, a 10-degree caudocranial tilt view (plateau view) can be highly advantageous for accurately visualizing the articular surface without overlapping the anterior and posterior rims.

Advanced Imaging Protocols
Computed tomography with two-dimensional multiplanar reconstructions and three-dimensional surface rendering is now considered the gold standard and is mandatory for all displaced tibial plateau fractures. CT imaging allows for the precise mapping of articular comminution, identification of the primary fracture lines, and localization of central depression voids that are often obscured on plain radiographs. The Kfuri and Schatzker CT-based classification system further divides the plateau into anterior, posterior, medial, and lateral quadrants, aiding in the determination of the optimal surgical trajectory. Magnetic Resonance Imaging may be utilized in cases where high suspicion of meniscal or ligamentous pathology exists, though it is rarely required in the acute trauma setting.
Patient Positioning and Preparation
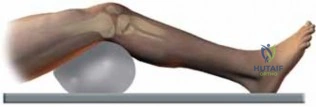
The patient is positioned supine on a fully radiolucent operative table to allow unimpeded intraoperative fluoroscopy. A bump is placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the patella points directly toward the ceiling. This facilitates a true anteroposterior fluoroscopic view. A sterile tourniquet is applied to the proximal thigh to provide a bloodless surgical field, though its inflation should be minimized to reduce the risk of postoperative deep vein thrombosis and soft tissue ischemia.

The contralateral leg is carefully padded and secured. The C-arm fluoroscopy unit is typically positioned on the contralateral side of the operative table, coming in perpendicular to the patient. Prior to incision, the surgeon must confirm that perfect AP and lateral fluoroscopic images of the proximal tibia can be obtained without obstruction from the table column or contralateral limb.
Detailed Surgical Approach and Technique
The surgical management of lateral tibial plateau fractures requires meticulous soft tissue handling, anatomic articular reduction, and stable internal fixation to permit early range of motion. The standard approach for isolated lateral plateau fractures (Schatzker I, II, III) is the anterolateral approach.
Surgical Approach
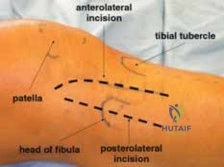
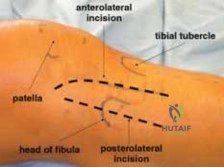
The incision is centered over Gerdy’s tubercle, extending proximally toward the lateral epicondyle of the femur and distally along the anterolateral aspect of the tibial shaft, just lateral to the tibial crest. The length of the incision is dictated by the planned plate length. Full-thickness fasciocutaneous flaps are maintained to preserve the precarious vascular supply to the skin.

The iliotibial band is incised in line with its fibers. The anterior tibialis muscle is elevated off the proximal lateral tibia. There is no true internervous plane here, but the dissection occurs between the iliotibial tract (gluteal nerves) and the anterior compartment musculature (deep peroneal nerve). To visualize the articular surface, a submeniscal arthrotomy is performed. The coronary ligaments attaching the anterior horn and body of the lateral meniscus to the tibia are carefully incised, and the meniscus is elevated superiorly using non-absorbable stay sutures. This maneuver exposes the lateral articular surface and allows direct visualization of the fracture reduction.
Fracture Reduction Techniques
In cases of a pure split fracture (Schatzker I), the lateral fragment is opened like a book. The joint is irrigated to remove hematoma and osteochondral debris. The fragment is then reduced anatomically using a large pointed reduction forceps.

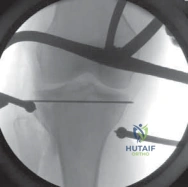
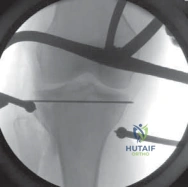
For split-depression (Schatzker II) or pure depression (Schatzker III) fractures, the depressed articular fragments must be elevated. A cortical window is created in the anterolateral metaphyseal bone, distal to the fracture line. A curved bone tamp is inserted through this window and directed proximally beneath the depressed articular segment. Under direct visualization through the submeniscal arthrotomy and concurrent fluoroscopic guidance, the articular fragments are gently elevated to restore the joint line.
Elevation of the depressed fragments invariably leaves a substantial metaphyseal bone void. To prevent postoperative subsidence of the articular surface, this void must be filled. Options include autologous bone graft (typically harvested from the ipsilateral iliac crest), allograft (cancellous chips), or synthetic bone substitutes (calcium phosphate cement). Calcium phosphate is highly favored in modern practice due to its high compressive strength, which supports the elevated articular fragments during the healing phase.
Internal Fixation
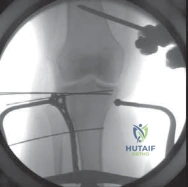
Once the articular surface is reduced and the metaphyseal void is grafted, definitive fixation is applied. A pre-contoured lateral proximal tibial locking plate is utilized. The plate functions as a buttress to resist the valgus shear forces inherent to the lateral plateau.
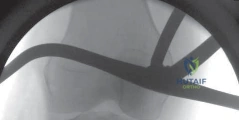
Subchondral raft screws (typically 3.5 mm or 4.5 mm) are inserted through the proximal holes of the plate, positioned parallel to the joint surface and as close to the subchondral bone as possible to support the elevated articular fragments. The distal aspect of the plate is secured to the tibial shaft using a combination of cortical and locking screws.
Prior to closure, the lateral meniscus must be meticulously repaired back to the capsule and tibial rim using the previously placed stay sutures. Failure to restore meniscal stability leads to rapid joint degeneration. The iliotibial band and fascia are closed loosely over a suction drain, followed by careful subcutaneous and skin closure.
Complications and Management
The management of lateral tibial plateau fractures is fraught with potential complications, ranging from acute limb-threatening conditions to chronic debilitating joint dysfunction. The physical examination must continuously assess for these pathologies both preoperatively and postoperatively.

Compartment syndrome is the most devastating acute complication. The high-energy nature of many plateau fractures, combined with the closed fascial compartments of the leg, creates an environment ripe for elevated intracompartmental pressures. A high index of suspicion must be maintained, particularly in patients with disproportionate pain, tense compartments, or pain with passive stretch of the toes. If compartment syndrome is suspected, immediate measurement of compartmental pressures and four-compartment fasciotomies are mandatory.
Infection and wound dehiscence are significant risks due to the thin soft tissue envelope surrounding the proximal tibia. Meticulous surgical technique, appropriate timing of surgery, and the use of incisional negative pressure wound therapy can mitigate these risks.
| Complication | Estimated Incidence | Pathophysiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Compartment Syndrome | 5% - 10% | Hemorrhage and edema within rigid fascial compartments; High-energy trauma. | Emergent four-compartment fasciotomy; Delayed primary closure or skin grafting. |
| Surgical Site Infection | 3% - 8% | Thin soft tissue envelope; Early surgical intervention through compromised skin. | Aggressive surgical debridement; Intravenous antibiotics; Hardware removal if union achieved; Flap coverage for exposed hardware. |
| Posttraumatic Osteoarthritis | 20% - 40% | Residual articular incongruity; Meniscal loss; Altered mechanical axis. | Conservative management (NSAIDs, injections); Corrective osteotomy for malalignment; Total knee arthroplasty for end-stage disease. |
| Loss of Reduction / Subsidence | 5% - 15% | Inadequate structural support of metaphyseal void; Premature weight-bearing; Osteoporosis. | Revision open reduction and internal fixation with structural grafting; Conversion to arthroplasty in severe cases. |
| Peroneal Nerve Injury | 1% - 3% | Traction injury during varus stress or iatrogenic injury during lateral retractor placement. | Observation and ankle-foot orthosis (AFO) for neuropraxia; Nerve exploration if transection is suspected or no recovery at 3-6 months. |
Post Operative Rehabilitation Protocols
Rehabilitation following lateral tibial plateau fracture fixation must balance the competing demands of mechanical stability for bone healing and early joint mobilization to prevent arthrofibrosis and promote cartilage nutrition. The integrity of the fixation and the status of the meniscus dictate the pace of the rehabilitation protocol.

Phase I: Maximum Protection (Weeks 0-6)
Immediately postoperatively, the knee is typically placed in a hinged knee brace locked in full extension to protect the soft tissues during ambulation. However, early passive and active-assisted range of motion is initiated within the first 48 hours to prevent capsular contracture. Continuous Passive Motion machines may be utilized, aiming for 0 to 90 degrees of flexion within the first two weeks. Weight-bearing is strictly restricted to non-weight-bearing or toe-touch weight-bearing (less than 20 lbs) to prevent subsidence of the articular fragments. If a meniscal repair was performed, flexion beyond 90 degrees may be restricted for the first 4 to 6 weeks to protect the repair from shear forces.
Phase II: Progressive Loading (Weeks 6-12)
At six weeks postoperatively, clinical and radiographic evaluations are performed to assess callus formation and maintenance of articular reduction. If radiographic healing is progressing satisfactorily, the patient is transitioned to partial weight-bearing, typically advancing by 25% of body weight per week. Range of motion exercises are intensified to achieve full, symmetric flexion and extension. Closed kinetic chain strengthening is initiated, focusing on quadriceps and hamstring co-contraction to dynamically stabilize the knee.
Phase III: Return to Function (Weeks 12+)
Full weight-bearing is generally permitted by 10 to 12 weeks, contingent upon radiographic union. The focus of rehabilitation shifts to advanced strengthening, proprioceptive training, and functional restoration. Return to high-impact activities or sports is typically delayed until 6 to 9 months postoperatively, requiring symmetric lower extremity strength and complete radiographic consolidation.
Summary of Key Literature and Guidelines
The academic discourse surrounding lateral tibial plateau fractures is extensive, with several landmark studies shaping contemporary surgical management. The seminal work by Schatzker et al. established the morphological classification system that remains the lingua franca of orthopedic traumatology. Schatzker’s assertion that displaced intra-articular fractures require anatomic reduction and stable fixation to prevent osteoarthritis remains a core tenet of modern practice.

More recently, the integration of computed tomography has revolutionized our understanding of fracture morphology. Kfuri and Schatzker proposed a CT-based three-dimensional classification system that highlights the importance of the posterior coronal fracture line, a feature often missed on plain radiographs. This has led to an increased recognition of posterolateral shear fragments, necessitating modified surgical approaches, such as the posterolateral approach with fibular osteotomy, to achieve adequate buttressing.
The debate regarding the critical threshold for articular depression that warrants surgical intervention continues. While classic literature suggested 3 to 5 mm of depression as the threshold, modern consensus emphasizes that the absolute measurement is less critical than the presence of associated joint instability. A 2 mm depression in a highly active patient with a concomitant meniscal tear may warrant surgery, whereas a 5 mm central depression in an elderly, low-demand patient with a stable knee may be managed non-operatively.
The management of metaphyseal voids has also evolved. Studies comparing autograft to calcium phosphate cement have demonstrated that calcium phosphate provides superior compressive strength and lower rates of articular subsidence in Schatzker II and III fractures, without the donor site morbidity associated with iliac crest bone grafting.
Ultimately, the successful management of lateral tibial plateau fractures relies on a synthesis of meticulous preoperative planning, respect for the soft tissue envelope, anatomic articular restoration, and a biologically sound rehabilitation protocol. Adherence to these principles minimizes the risk of early posttraumatic arthritis and maximizes long-term functional outcomes for the patient.
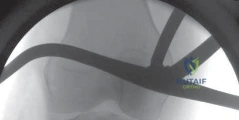
Clinical & Radiographic Imaging